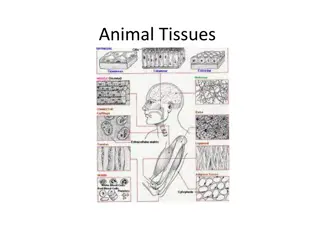
Tissue Regeneration, Repair, and Inflammation Explained

Tissue regeneration and repair processes involve either regeneration of cells or connective tissue repair, depending on the type of cells injured. In cases where regeneration is not possible, healing occurs through the formation of scar tissue. The healing process aims to restore the structural continuity of the injured tissue, with phases involving angiogenesis, fibroblast migration, extracellular matrix deposition, and tissue remodeling. Fibrosis and organization may also occur in certain tissues as part of the repair process.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
TISSUE REGENERATION TISSUE REPAIR INFLAMMATION PROF. DR. DALYA BASIL
TISSUE REGENERATION AND REPAIR Injured or damaged tissues can be repaired in one of two ways, by regeneration or connective mechanism used for repair will depend upon the type of cells that were injured. Certain cells in the body are fully or partially capable of regenerating after an injury, whereas other cell types are not and can only be replaced with connective (scar) tissue. tissue replacement. The
TISSUE REGENERATION AND REPAIR The primary objective of the healing process is to fill the gap created by tissue destruction and to restore the structural continuity of the injured part. Tissue regeneration refers to the restoration of injured tissue to its normal structure and function by proliferation of adjacent surviving cells. Cell renewal occurs continuously in labile tissues such as gastrointestinal epithelium and skin. Regeneration can also occur in parenchymal organs with stable cell populations, usually is a limited process, with the exception of the liver (Hepatocytes have unlimited and unique regenerative capacity). It should be pointed out that extensive regeneration can occur only if the residual tissue is structurally and functionally intact.
HEALING BY CONNECTIVE TISSUE REPAIR When regeneration cannot occur, healing by replacement with a connective (fibrous) tissue occurs, a process that terminates in scar formation. The term fibrosis is often used to describe the extensive deposition of collagen that occurs in organs such as the lungs,liver,or kidney as a result of chronic inflammation or injury. If fibrosis occurs in any tissue space occupied by an inflammatory exudate, it is called organization. It occurs in serous cavities such as the pericardium and peritoneal cavities. In the pericardium, fibroblasts secrete and organize collagen within fibrous strands. Fibrous strands sometimes become organized within the peritoneal cavity following abdominal surgery or peritonitis.These strands of collagen,called adhesions,can trap loops of bowel and cause obstruction.
ORGANIZED STRANDS OF COLLAGEN (ARROWS) IN CONSTRICTIVE PERICARDITIS
PHASES OF REPAIR Repair by connective tissue deposition can be divided into three phases: (1) angiogenesis and ingrowth of granulation tissue (2) emigration of fibroblasts and deposition of extracellular matrix (3) maturation and reorganization of the fibrous tissue (remodeling). It usually begins within 24 hours of injury and is evidenced by the migration of fibroblasts and the induction of fibroblast and endothelial cell proliferation.By 3 to 5 days,a special type of tissue called granulation tissue is apparent. The granulation tissue then progressively accumulates connective tissue, eventually resulting in the formation of a scar, which is then remodeled.
CUTANEOUS WOUND HEALING Cutaneous Wound Healing: This is a process that involves both epithelial cell regeneration and formation of connective tissue (scar formation). Healing by Primary and Secondary Intention: Depending on the extent of tissue loss, wound closure and healing occur by primary or secondary intention. A sutured surgical incision is an example of healing by primary intention. Larger wounds (e.g., burns and large surface wounds) that have a greater loss of tissue and contamination heal by secondary intention. Healing by secondary intention is slower than healing by primary intention and results in the formation of larger amounts of scar tissue. A wound that might otherwise have healed by primary intention may become infected and heal by secondary intention.
PRIMARY INTENTION VS SECONDARY INTENTION
PHASES OF CUTANEOUS WOUND HEALING Cutaneous wound healing is commonly divided into three phases: (1) inflammatory phase (2) proliferative phase (3) maturational or remodeling phase. The duration of the phases is fairly predictable in wounds healing by primary intention. In wounds healing by secondary intention, the process depends on the extent of injury and the healing environment.
INFLAMMATORY PHASE The inflammatory phase begins at the time of injury and is a critical period because it prepares the wound environment for healing.It includes:hemostasis,vascular and cellular phases of inflammation. a) Hemostatic processes are activated immediately at the time of injury. There is vasoconstriction of injured blood vessels and initiation of blood clotting by way of platelet activation and aggregation. b) Vascular phase: After a brief period of constriction, the same vessels dilate and capillaries increase their permeability,allowing plasma and blood components to leak into the injured area. c) The cellular phase of inflammation: Migration of phagocytic white blood cells that digest and remove invading organisms,fibrin,extracellular debris,and other foreign matter.
PROLIFERATIVE PHASE The proliferative phase of healing usually begins within 2 to 3 days of injury and may last as long as 3 weeks in wounds healing by primary intention.The primary processes during this time focus on the building of new tissue to fill the wound space. The key cell during this phase is the fibroblast. The fibroblast is a connective tissue cell that synthesizes and secretes collagen and other intercellular elements needed for wound healing. Fibroblasts also produce a family of growth factors that induce angiogenesis and endothelial cell proliferation and migration.
PROLIFERATIVE PHASE As early as 24 to 48 hours after injury, fibroblasts and vascular endothelial cells begin proliferating to form the granulation tissue that serves as the foundation for scar tissue development.This tissue is fragile and bleeds easily because of the numerous, newly developed capillary buds. The final component of the proliferative phase is epithelialization, which is the migration, proliferation, and differentiation of the epithelial cells at the wound edges to form a new surface layer that is similar to that destroyed by the injury.
PROLIFERATIVE PHASE In wounds that heal by primary intention, these epidermal cells proliferate and seal the wound within 24 to 48 hours. Because epithelial cell migration requires a moist vascular wound surface and is impeded by a dry or necrotic wound surface, epithelialization is delayed in open wounds until a bed of granulation tissue has formed. When a scab has formed on the wound, the epithelial cells migrate between it and the underlying viable tissue; when a significant portion of the wound has been covered with epithelial tissue,the scab lifts off.
PROLIFERATIVE PHASE As the proliferative phase progresses, there is continued accumulation of collagen and proliferation of fibroblasts. Collagen synthesis reaches a peak within 5 to 7 days and continues for several weeks, depending on wound size. By the second week, the white blood cells have largely left the area, the edema has diminished, and the wound begins to blanch as the small blood vessels become thrombosed and degenerate.
REMODELING PHASE Remodeling Phase. The third phase of wound healing, the remodeling process, begins approximately 3 weeks after injury and can continue for 6 months or longer, depending on the extent of the wound. There is a continuing remodeling of scar tissue by simultaneous synthesis of collagen by fibroblasts and lysis by collagenase enzymes. As a result of these two processes, the architecture of the scar becomes reoriented to increase the tensile strength of the wound.
REMODELING PHASE An abnormality in healing by scar tissue repair is keloid formation. Keloids are benign tumor like masses caused by excess production of scar tissue. They tend to develop in genetically predisposed individuals and are more common in African Americans, Asian Americans, Latin Americans, and other ethnic groups with darker pigmented skin. The majority of keloids lead to considerable cosmetic defects, but can grow to sufficient size to become symptomatic by causing deformity or limiting joint mobility.
FACTORS THAT AFFECT WOUND HEALING Nutritional Status: Successful wound healing depends in part on adequate stores of proteins, carbohydrates, fats, vitamins, and minerals. It is well recognized that malnutrition slows the healing process, causing wounds to heal inadequately or incompletely. Protein deficiencies prolong the inflammatory phase of healing and impair fibroblast proliferation,collagen and protein matrix synthesis,angiogenesis,and wound remodeling. Carbohydrates are needed as an energy source for white blood cells. Fats are essential constituents of cell membranes and are needed for the synthesis of new cells. Most vitamins are essential cofactors for the daily functions of the body,vitamins A and C play an essential role in the healing process.Vitamin C is needed for collagen synthesis.
FACTORS THAT AFFECT WOUND HEALING The role of minerals in wound healing is less clearly defined. The macrominerals, including sodium, potassium, calcium, and phosphorus, as well as the microminerals such as copper and zinc,must be present for normal cell function.Zinc is a cofactor in a variety of enzyme systems responsible for cell proliferation. In previous studies, zinc has been found to aid in re- epithelialization.
FACTORS THAT AFFECT WOUND HEALING Blood Flow and Oxygen Delivery: For healing to occur, wounds must have adequate blood flow to supply the necessary nutrients and to remove the resulting waste, local toxins, bacteria, and other debris. Oxygen is required for collagen synthesis and killing of bacteria by phagocytic white blood cells. It has been shown that even a temporary lack of oxygen can result in the formation of less stable collagen.Wounds in ischemic tissue become infected more frequently than wounds in well- vascularized tissue.
FACTORS THAT AFFECT WOUND HEALING Impaired Inflammatory and Immune Responses: Inflammation is essential to the first phase of wound healing, and immune mechanisms prevent infections that impair wound healing. Among the conditions that impair inflammation and immune function are disorders of phagocytic function, diabetes mellitus,and therapeutic administration of corticosteroid drugs. Wound healing is a problem in persons with diabetes mellitus, particularly those who have poorly controlled blood glucose levels. Studies have shown delayed wound healing, poor collagen formation, and poor tensile strength in diabetes mellitus.Of particular importance is the effect of hyperglycemia on phagocytic function.
FACTORS THAT AFFECT WOUND HEALING The decreases the inflammatory process and may delay the healing process. These drugs decrease capillary permeability during the early stages of inflammation, impair the phagocytic property of the leukocytes,and inhibit fibroblast proliferation and function. therapeutic administration of corticosteroid drugs
FACTORS THAT AFFECT WOUND HEALING Infection, Wound Separation, and Foreign Bodies: Infection impairs all dimensions of wound healing. It prolongs the inflammatory phase, impairs the formation of granulation tissue, and inhibits proliferation of fibroblasts and deposition of collagen fibers. Approximation of the wound edges (i.e., suturing of an incision type of wound) greatly enhances healing and prevents infection. Epithelialization of a wound with closely approximated edges occurs within 1 to 2 days. Large, gaping wounds tend to heal more slowly because it is often impossible to effect wound closure with this type of wound.
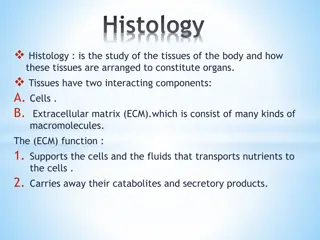
INFLAMMATION Inflammation is a complex response intended to minimize the effects of injury or infection, remove the damaged tissue, and generate new tissue. It accomplishes this by diluting, destroying, or otherwise neutralizing the harmful agents. Inflammation is the reaction of vascularized tissues to cell injury or death, characterized by the elaboration of inflammatory mediators and the movement of fluid and leukocytes from the vascular system into the extravascular tissues.
GENERAL FEATURES OF INFLAMMATION Inflammatory conditions are commonly named by adding the suffix -itis to the affected organ or system. For example, appendicitis refers to inflammation of the appendix, pericarditis to inflammation of the pericardium, and neuritis to inflammation of a nerve. Inflammation can be acute or chronic. Acute inflammation is the adaptive response that is triggered by noxious stimuli and conditions, such as infection and tissue injury, and is of relatively short duration, lasting from a few minutes to several days. It is characterized by the exudation of fluid and plasma proteins and emigration of leukocytes,predominantly neutrophils. Chronic inflammation is of a longer duration, lasting for days to years, and is associated with the proliferation of blood vessels, tissue necrosis, and fibrosis (scarring).
CELLS OF INFLAMMATION Many cells and tissue components are involved in the inflammatory process, including the endothelial cells that line blood vessels, circulating platelets and leukocytes, connective tissue cells (mast cells, fibroblasts, tissue macrophages),and components of the extracellular matrix. The principal leukocytes in acute inflammation are neutrophils, whereas macrophages, lymphocytes and plasma cells, eosinophils, and mast cells predominate in chronic inflammation.
CELLS OF INFLAMMATION Endothelial Cells: Endothelial cells comprise the single-cell-thick epithelial lining of blood vessels. They produce antiplatelet and antithrombotic agents that maintain vessel patency, as well as vasodilators and vasoconstrictors that regulate blood flow. Endothelial cells are also key players in the inflammatory response. As such, they provide a selective permeability barrier to exogenous (microbial) and endogenous inflammatory stimuli; regulate leukocyte extravasation, and release of inflammatory mediators; and regulate immune cell proliferation through secretion of hematopoietic colony-stimulating factors (CSFs).
CELLS OF INFLAMMATION Platelets or thrombocytes are small membrane-bound disks circulating in the blood that play an active role in normal hemostasis. Activated platelets also release a number of potent inflammatory mediators, thereby increasing vascular permeability and altering the chemotactic, adhesive, and proteolytic properties of the endothelial cells. Leukocytes (WBCs) are the major cellular components of the inflammatory response. They include the granulocytes (neutrophils, eosinophils, and basophils), which contain specific cytoplasmic granules and a multilobed nucleus, and the agranulocytes (monocytes/macrophages and lymphocytes), which lack cytoplasmic granules and have a single nucleus.
CELLS OF INFLAMMATION Neutrophils: Neutrophils are the most numerous leukocytes in the circulating blood,accounting for 60% to 70% of all white blood cells.These leukocytes are referred to polymorphonuclear neutrophils (PMNs). Because of their ability to form pseudopods used in ameboid movement, neutrophils are highly mobile and are therefore the first cells to appear at the site of acute inflammation,usually arriving within 90 minutes of injury.They are capable of engulfing bacteria and other cellular debris through phagocytosis. They have oxygen-dependent metabolic pathways that generate toxic oxygen (e.g., hydrogen peroxide) and nitrogen (e.g., nitric oxide) products that aid in the destruction of engulfed pathogens.
CELLS OF INFLAMMATION Eosinophils: Eosinophils account for 2% to 3% of circulating leukocytes and are recruited to tissues similar to neutrophils. Their appearance at the site of inflammation occurs 2 to 3 hours after the neutrophils. This is, in part, because of their slower mobility and comparatively slower reaction to chemotactic stimuli. The granules of eosinophils, which stain pink with the acid dye eosin, contain a protein that is highly toxic to large parasitic worms that cannot be phagocytized. Eosinophils have a longer life span than neutrophils and therefore present in chronic inflammation.
CELLS OF INFLAMMATION Basophils and Mast Cells: Basophils are account for less than 1% of the circulating leukocytes, they are important participants in inflammatory reactions and are most prominent in allergic reactions mediated by immunoglobulin E (IgE). Monocyte/Macrophages: Monocytes constitute 3%to 8% of the white blood cell count. They have a single kidney-shaped nucleus and are the largest of the circulating leukocytes.The half-life of circulating monocytes is about a day,after which they begin to migrate to the site of injury and undergo transformation into larger macrophages, which have a longer half-life and greater phagocytic ability than do blood monocytes.
CELLS OF INFLAMMATION Lymphocytes and Plasma Cells: Lymphocytes are participate in immune-mediated inflammation caused by infectious agents as well as non immune-mediated inflammation associated with cell injury and death. Both T and B lymphocytes (T and B cells) migrate into inflammatory sites using some of the same adhesion molecules and chemokines that recruit neutrophils and other leukocytes. Plasma cells develop from activated B lymphocytes and produce antibodies directed against persistent antigens in the inflammatory site and against altered tissue components. In some intense chronic inflammatory reactions, the accumulation of lymphocytes and plasma cells may assume the appearance of lymphoid organs, such as lymph nodes. This pattern of lymphocyte accumulation is often seen in the inflamed synovium of persons with long-standing rheumatoid arthritis.
CELLS OF INFLAMMATION Cell Adhesion Molecules and Leukocyte Recruitment:Several families of cell adhesion molecules, including selectins, integrins, and the immunoglobulin superfamily, are involved in leukocyte recruitment and trafficking. The selectins are a family of three closely related proteins (E-selectin, L-selectin, P- selectin) that differ in their cellular distribution but all function in adhesion of leukocytes to endothelial cells. The integrin superfamily consists of 30 structurally similar proteins that promote cell-to-cell interactions. and cell to extracellular matrix
CELLS OF INFLAMMATION The importance of the leukocyte adhesion molecules is demonstrated in persons with an inherited disorder called leukocyte adhesion deficiency (LAD) type I,in which deficiency of a member of the integrin superfamily leads to severe leukocytosis and recurrent infections.A similar deficiency is seen in individuals with impaired expression of a member of the selectin superfamily and has been labeled LAD type 2. There is also evidence that excessive expression of cell adhesion molecules or their receptors contributes to the pathogenesis of some chronic inflammatory diseases such as rheumatoid arthritis.




 IN")