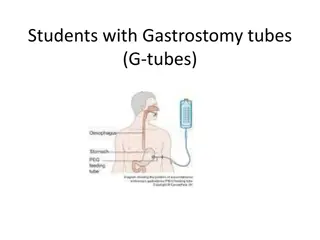
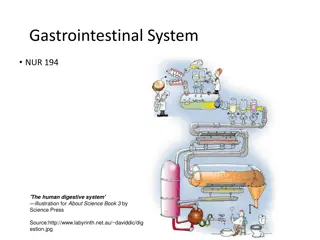
Understanding the Anatomy of the Stomach
The stomach, also known as the gaster or venter, is a vital organ in the digestive system. It is a muscular bag that plays a crucial role in food digestion and absorption. This article covers the surface anatomy, external and internal features, blood supply, nerve supply, lymphatic drainage, clinical anatomy, and the location and shape of the stomach. Detailed descriptions and diagrams are provided to enhance understanding and knowledge of this essential organ.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
STOMACH Dr.Manjula Vastrad Asst.Prof Dept of Rachana Shareera SMVVS RKM AMC Vijayapur Email: manjula.prasad2010@gmail.com
CONTENTS CONTENTS INTRODUCTION INTRODUCTION SURFACE ANATOMY SURFACE ANATOMY EXTERNAL & INTERNAL FEATURES EXTERNAL & INTERNAL FEATURES RELATIONS OF THE STOMACH RELATIONS OF THE STOMACH BLOOD SUPPLY BLOOD SUPPLY NERVE SUPPLY NERVE SUPPLY LYMPHATIC DRAINAGE LYMPHATIC DRAINAGE CLINICAL ANATOMY CLINICAL ANATOMY
INTRODUCTION INTRODUCTION The stomach is also known as The stomach is also known as GASTER GASTER or VENTER. VENTER. DEFINITION DEFINITION- - The stomach is a muscular The stomach is a muscular bag forming the widest and bag forming the widest and most distensible part of most distensible part of digestive tube. digestive tube. EXTENT EXTENT It is connected above to the It is connected above to the lower end of Esophagus lower end of Esophagus and below to the and below to the Duodenum. Duodenum.
LOCATION OF THE STOMACH LOCATION OF THE STOMACH The stomach lies obliquely in the upper and left part of the abdomen, occupying the EPIGASTRIC, UMBLICAL & LEFT HYPOCHONDRIAC REGIONS. SHAPE OF STOMACH SHAPE OF STOMACH Empty Empty J shaped (vertical) J shaped (vertical) (ii) Partially distended Partially distended Pyriform (iii) In obese persons In obese persons - - Horizontal (i) (i) Pyriform Horizontal (ii) (iii)
SURFACE ANATOMY SURFACE ANATOMY CARDIAC ORIFICE CARDIAC ORIFICE- - A point on the 7 cartilage,2.5cm away from midline. It is represented by two cartilage,2.5cm away from midline. It is represented by two lines 1.25cm apart lines 1.25cm apart. . A point on the 7th th costal costal PYLORIC ORIFICE PYLORIC ORIFICE- - A point on the on the right side 1.25cm away from the midline. on the right side 1.25cm away from the midline. A point on the transpyloric transpyloric plane and plane and LESSER CURVATURE LESSER CURVATURE- - Join right margin of to the upper margin of pylorus by means of curved J shape to the upper margin of pylorus by means of curved J shape line. line. Join right margin of cardic cardic orifice orifice FUNDUS FUNDUS- - Point in the left 5 Point in the left 5th thintercostal space just below the nipple. Draw a line joining the left margin of cardiac the nipple. Draw a line joining the left margin of cardiac orifice with above point. orifice with above point. intercostal space just below GREATER CURVATURE GREATER CURVATURE- - Draw tip of 9 tip of 9th th & 10 & 10th th costal cartilage. Draw a curved line convex to the left costal cartilage. Draw a curved line convex to the left from from fundus fundus to the point marked and reaching downwards to the to the point marked and reaching downwards to the subcostal subcostal plane and then reaching the lower margin of pylorus plane and then reaching the lower margin of pylorus. Draw subcostal subcostal plane. Put a pt. b/w the plane. Put a pt. b/w the
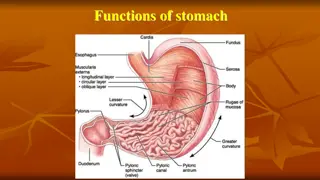
EXTERNAL FEATURES EXTERNAL FEATURES THE STOMACH HAS THE STOMACH HAS- - (i) TWO ORIFICES i.e Cardiac orifice & pyloric orifice. (ii) TWO CURVATURES TWO CURVATURES i.e lesser curvature and greater curvature. (iii) TWO SURFACES TWO SURFACES i.e anterior & posterior surface. (iv) PARTS OF STOMACH PARTS OF STOMACH i.e fundus , body , pyloric antrum & pyloric canal.
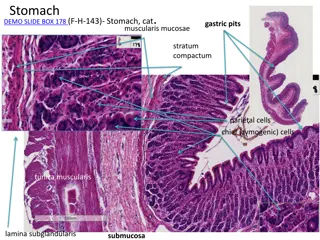
INTERNAL INTERNAL FEATURES FEATURES The stomach wall is composed of four basic layers : MUCOSA MUCOSA SUB SUB- -MUCOSA MUCOSA MUSCULARIS MUSCULARIS SEROSA SEROSA MUCOSA MUCOSA Consist of ( Consist of (i i) surface mucous cells ) surface mucous cells (ii)Lamina Lamina propria propria (iii) (iii) Muscularis Muscularis mucosa Mucosa of empty stomach is thrown into folds termed Mucosa of empty stomach is thrown into folds termed RUGAE. RUGAE. Mucosa form columns of Mucosa form columns of secretery GLANDS GLANDS. . (i) (i) (ii) (ii) (iii) (iii) (iv) (iv) (ii) mucosa secretery cells called cells called GASTRIC GASTRIC
SUB SUB- -MUCOSA MUCOSA- - composed of areolar connective tissue composed of areolar connective tissue MUSCULARIS MUSCULARIS- - composed of three layers of smooth muscles composed of three layers of smooth muscles i.e. i.e. OUTER LONGITUDINAL OUTER LONGITUDINAL MIDDLE CIRCULAR MIDDLE CIRCULAR (iii) INTERNAL OBLIQUE INTERNAL OBLIQUE (i) (i) (ii) (ii) (iii) SEROSA SEROSA- - composed of simple squomous epithelium composed of simple squomous epithelium
RELATIONS RELATIONS OF OF STOMACH STOMACH PERITONEAL RELATIONS PERITONEAL RELATIONS The stomach is lined by peritoneum on both it surfaces The stomach is lined by peritoneum on both it surfaces. At lesser curvature, the layers of peritoneum lining the At lesser curvature, the layers of peritoneum lining the anterior and posterior surface meet and become anterior and posterior surface meet and become continous continous with lesser with lesser omentum omentum. . Along the greater part of greater Along the greater part of greater curvature,the meet to form the greater meet to form the greater omentum curvature,the layers omentum. . layers Near Near fundus fundus, the two layers meet to form GASTRO , the two layers meet to form GASTRO- - SPLENIC LIGAMENT. SPLENIC LIGAMENT. Near Near cadiac cadiac end, the peritoneum on the posterior surface end, the peritoneum on the posterior surface is reflected on the diaphragm as GASTROPHRENIC is reflected on the diaphragm as GASTROPHRENIC LIGAMENT. LIGAMENT.
VISCERAL VISCERAL RELATIONS RELATIONS ANTERIOR ANTERIOR RELATIONS RELATIONS The anterior surface of The anterior surface of stomach is related to the: stomach is related to the:- - ( (i i) LIVER ) LIVER (ii) DIAPHGRAM (ii) DIAPHGRAM (iii) ANTERIOR ABDOMINAL (iii) ANTERIOR ABDOMINAL WALL WALL
POSTERIOR POSTERIOR RELATION RELATION The posterior surface of The posterior surface of stomach is related to stomach is related to structures forming the structures forming the STOMACH BED STOMACH BED. . These structures are: These structures are:- - (i) (i) DIAPHRAGM DIAPHRAGM (ii) (ii) LEFT KIDNEY LEFT KIDNEY (iii) (iii) LEFT SUPRA LEFT SUPRA- -RENAL GLAND (iv) (iv) PANCREAS PANCREAS (v) (v) TRANSVERSE MESOCOLON TRANSVERSE MESOCOLON (vi) (vi) SPLENIC FLEXURE OF SPLENIC FLEXURE OF COLON COLON (vii) (vii) SPLENIC ARTERY SPLENIC ARTERY RENAL GLAND
BLOOD SUPPLY BLOOD SUPPLY The stomach is supplied by: The stomach is supplied by:- - (i) (i) The left Gastric Artery, a branch of COELIAC TRUNK. The left Gastric Artery, a branch of COELIAC TRUNK. (ii) (ii) The right Gastric The right Gastric Artery,a Artery,a branch of COMMON HEPATIC ARTERY. branch of COMMON HEPATIC ARTERY. (iii) (iii) Right Gastro Right Gastro- -epiploic epiploic artery, a branch of Gastro artery, a branch of Gastro- -deudonal (iv) (iv) Left Gastro Left Gastro- -epiploic epiploic artery, a branch of artery, a branch of Splenic (v) (v) 5 5- -7 short gastric arteries. 7 short gastric arteries. deudonal artery artery. artery Splenic artery. VENOUS DRAINAGE VENOUS DRAINAGE The veins of stomach drain into portal , Superior The veins of stomach drain into portal , Superior mesentric Splenic Splenic veins. veins. mesentric and and
LYMPHATIC LYMPHATIC DRAINAGE DRAINAGE AREA AREA A A PANCREATICO PANCREATICO- - SPLENIC AREA SPLENIC AREA GASTRIC NODES EPIPLO IC NODES AREA AREA B B DRAINS TO LEFT DRAINS INTO DRAINS INTO DRAINS INTO GASTRIC NODES RIGHT RIGHT GASTRO GASTRO- - EPIPLO IC NODES DIRECTION AREA AREA C C AREA AREA D D DRAINS INTO DIFFERENT DIRECTION DRAINS TO LEFT DIFFERENT DRAINS INTO DRAINS INTO PANCREATRCO PANCREATRCO- - SPLENIC NODES SPLENIC NODES COELIAC NODES COELIAC NODES INTESTINAL LYMPH TRUNK INTESTINAL LYMPH TRUNK CISTERNA CHYLI CISTERNA CHYLI HEPATIC NODES HEPATIC NODES
NERVE NERVE SUPPLY SUPPLY STOMACH IS SUPPLIED BY STOMACH IS SUPPLIED BY SYMPATHETIC SYMPATHETIC PARASYMPATHETIC PARASYMPATHETIC (T (T6 6 to T to T9 9 via via Coeliac Coeliac Plexus) Plexus) (Anterior & Posterior (Anterior & Posterior Vagus Vagus N.) N.)
CLINICAL ANATOMY CLINICAL ANATOMY GASTRITIS GASTRITIS (i) (i) Gastritis means inflammation of Gastritis means inflammation of the gastric mucosa the gastric mucosa (ii) (ii) In Gastritis, the gastric mucosal In Gastritis, the gastric mucosal barrier become inflamed due to barrier become inflamed due to the ingestion of certain the ingestion of certain substances like substances like Alcohal These substances when often These substances when often ingested can be very damaging to ingested can be very damaging to the protective gastric mucosal the protective gastric mucosal barrier barrier i.e i.e to the mucous gland to the mucous gland and tight epithelial junctions and tight epithelial junctions between the gastric lining cells between the gastric lining cells leading to severe acute or chronic leading to severe acute or chronic gastritis . gastritis . Alcohal & Aspirin. & Aspirin.
GASTRIC PAIN GASTRIC PAIN Gastric pain is felt in the epigastrium because the stomach is supplied from segements T6-T9 of spinal cord, which also supply the upper part of abdominal wall.
GASTRIC ATROPHY GASTRIC ATROPHY Due to chronic gastritis, the Due to chronic gastritis, the mucosa gradually becomes mucosa gradually becomes atrophic until little or no atrophic until little or no gastric gland activity gastric gland activity remains. remains. (ii) Loss of stomach secretions Loss of stomach secretions in gastric atrophy leads to in gastric atrophy leads to achlorhydria and achlorhydria and occasionally pernicious occasionally pernicious anaemia. anaemia. (i) (i) (ii)
PERNICIOUS PERNICIOUS ANAEMIA ANAEMIA Pernicious anaemia is a common accompaniment of Pernicious anaemia is a common accompaniment of Achlorhydria Achlorhydria and and Gastric atrophy. Gastric atrophy. Normal gastric secretions contain intrinsic factor Normal gastric secretions contain intrinsic factor which is secreted by parietal cells which helps in which is secreted by parietal cells which helps in the absorption of vitamin B the absorption of vitamin B12 12 from ileum. from ileum. NO INTRINSIC FACTOR NO ABSORPTION OF VIT B NO INTRINSIC FACTOR NO ABSORPTION OF VIT B 12 12 AS A RESULT, MATURATION FAILURE OCCURS IN BONE MARROW , RESULTING AS A RESULT, MATURATION FAILURE OCCURS IN BONE MARROW , RESULTING IN PERNICIOUS ANAEMIA IN PERNICIOUS ANAEMIA
PEPTIC ULCERS PEPTIC ULCERS A PEPTIC ULCER is an excoriated area A PEPTIC ULCER is an excoriated area of the mucosa caused by of the mucosa caused by the digestive action digestive action of gastric juice. TYPES TYPES The two The two main types main types of ( (i i) GASTRIC (II) DUODENAL ) GASTRIC (II) DUODENAL BASIC CAUSE BASIC CAUSE: : Imbalance between the rate of Imbalance between the rate of secretions of gastric juice and secretions of gastric juice and the degree of protection afforded the degree of protection afforded by GASTRODUODENAL MUCOSAL by GASTRODUODENAL MUCOSAL BARRIER as well as BARRIER as well as neutralisation neutralisation of gastric acid by of gastric acid by duodenal juices. duodenal juices. the of gastric juice. of peptic ulcers peptic ulcers
PEPTIC ULCER CAN BE CAUSED BY TWO WAYS PEPTIC ULCER CAN BE CAUSED BY TWO WAYS (i) (i) Excess secreations of acid and pepsin by Excess secreations of acid and pepsin by gastric mucosa. gastric mucosa. (ii) Diminished ability of gastroduodenal mucosal Diminished ability of gastroduodenal mucosal barrier to protect against the digestive barrier to protect against the digestive properties of acid properties of acid- -pepsin complex pepsin complex. (ii)
PYLOROSPASM PYLOROSPASM Abnormality of pyloric Abnormality of pyloric sphincter can occur in sphincter can occur in infants in which smooth infants in which smooth muscle muscle fibres fibres of sphincter fails to relax normally, so fails to relax normally, so food does not pass easily food does not pass easily from stomach to from stomach to doudenum PYLORIC STENOSIS PYLORIC STENOSIS Narrowing of pyloric Narrowing of pyloric sphincter that must be sphincter that must be corrected surgically. The corrected surgically. The hallmark symptom is hallmark symptom is projectile vomiting projectile vomiting- - the spraying of liquid spraying of liquid vomitus vomitus some distance some distance from infant from infant of sphincter doudenum the
9/23/2024 26
ON STOMACH ON STOMACH PRESENTED BY- DR.TANVI MAHAJAN 1 st YEAR P.G SCHOLAR
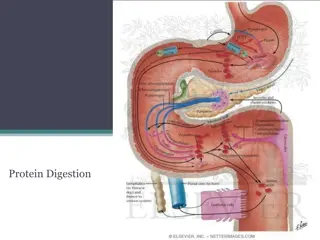
REGULATION OF REGULATION OF HCL HCL SECREATION SECREATION
TREATMENT OF PEPTIC ULCERS TREATMENT TREATMENT : (i) (i) Reduction of stressful situation, that might Reduction of stressful situation, that might lead to excessive acid secretions. lead to excessive acid secretions. (ii) Administration of antacid drugs to neutralize Administration of antacid drugs to neutralize much of the acid in stomach secretions. much of the acid in stomach secretions. (iii) Administration of Anti Administration of Anti- -Histaminic drugs that block the effect of Histamine on H block the effect of Histamine on H2 2 receptors and thereby reduce gastric acid secretions by and thereby reduce gastric acid secretions by 70% 70% - - 80%. 80%. (ii) Histaminic drugs that (iii) receptors