Understanding Mild Traumatic Brain Injury and Treatment Options

Exploring the pathophysiology and clinical recovery of mild traumatic brain injury (mTBI), along with the risk factors for persisting post-concussive symptoms. The importance of diagnosing mTBI and the impact it has on individuals. Highlighting the neurometabolic cascade and functional injuries associated with mTBI, as well as proposed clinical correlates. Additionally, discussing symptom-focused psychological treatments to address lingering post-concussive symptoms.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Mild Traumatic Brain Injury: Symptom-focused Treatment of Persisting Post-Concussive Symptoms Matthew R. Powell, PhD, LP, ABPP Mayo Clinic Rochester, Minnesota
Overview Review pathophysiology and typical clinical recovery following mild traumatic brain injury (mTBI) Discuss risk and maintenance factors of persisting postconcussive symptoms (PCS). Discuss symptom-focused psychological treatments that target lingering PCS.
Diagnosing mTBI: Clarifying Moment of Injury mTBI is about what happened to the patient at the time of the injury event and defined by the characteristics and course of clinical signs and symptoms during the acute period. James P. Kelly, MD Director, National Intrepid Center for TBI <30 minutes loss of consciousness <24 hours PTA After 30 minutes, GCS = 13-15 -American Congress of Rehabilitation Medicine, 1993
mTBI: Whats the Big Deal? 2-4 million mTBI estimated annually in US. Hospitalizations Due to Head Injury However, 30-50% never seek care. True incidence unclear. Moderate 10% Severe 10% 80% of TBI hospitalizations due to mTBI. Mild 80% estimates vary, but 5%-20% go on to develop PCS. Billions spent on mTBI on healthcare, lost work productivity.
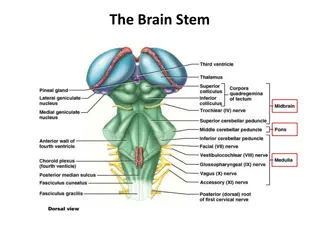
Neurometabolic Cascade 1. Nonspecific depolarization creates action potentials Excitatory neurotransmitter (EAA) release Massive efflux of potassium Calcium influx Disrupts ATP (pumps) Increased ionic pump activity (homeostasis) Increased energy demand Decreased blood flow and supply of glucose and oxygen. In more severe injury can be cell death, microtubule destruction, axon and white matter injury. 2. 3. 4. 5. 6. 7. 8. 9. Giza & Hovda Neurosurgery (2014)
Neurometabolic Cascade Giza & Hovda Neurosurgery (2014)
Pathophysiology Functional Injury oIonic shifts oMetabolic changes oImpaired neurotransmission Microstructural injury oChanges to integrity of white matter (DTI)
Physiology & Clinical Correlates Physiological perturbations after concussion and proposed clinical correlates. Post-TBI pathophysiology Acute symptom / clinical correlate Ionic flux Migraine headache, photophobia, phonophobia Energy crisis Vulnerability to second injury Axonal injury Impaired cognition, slowed processing, slowed reaction time Impaired neurotransmission Impaired cognition, slowed processing, slowed reaction time Giza & Hovda 2014
mTBI Spectrum Brief symptoms, resolving within seconds to minutes. Other end merges with moderate TBI. Loss of consciousness with post-traumatic amnesia lasting for < 24 hours. (complicated mild with some micro or macro neuropath may exist).
Typical Recovery of mTBI
Research & mTBI Population based research is very difficult as it requires following a large representative sample longitudinally. Studying Clinic samples are not ideal as this research is inherently biased as many individuals do not seek treatment following mTBI. Sport designs have provided a compromise; they give access to large populations at risk but there is some bias (young, healthy population).
Symptom Recovery: How Long? Rate of Postinjury Recovery in HS and College Athletes (n=790) Total (%) Cumulative Total (%) Rapid (< 1 day) 21.1 21.1 Gradual (1 to 7 days) 64.3 85.4 Prolonged (1 week 1 month) 11.9 97.3 Persistent (> 1 month) 2.7 100.0
Cognitive Recovery Following mTBI Meta-Analytic Studies and Reviews: Frencham, 2004; Belanger et al., 2005; Schretlin & Shapiro, 2003; Broglio et al 2008;; Rohling et al 2011 < 24 hours 1-6 Days 7-30 Days 30-90 Days 0 -0.2 -0.4 Effect Sizes (d) -0.6 -0.8 Effect Sizes: 0.2 Small, 0.5 Medium, 0.8 Large -1 < 0.3 Difficult to detect in individual patients; large overlap b/n patients and control group mTBI impact on cognition varies as a function of time since injury -1.2 -1.4 -1.6
Post Concussion Syndrome
What is PCS? mTBI + symptom persistence beyond 3 months and interfere with daily functioning. Symptoms: o Cognitive: concentration or memory problems o Somatosensory: headache, fatigue; sensitivity to light, noise; visual disturbances o Emotional: irritability, depression, insomnia o Vestibular: balance problems, dizziness PCD - DSM-IV (symptoms lasting more than 3 months, objective evidence of cognitive problems) PCS - ICD-10 (history of head trauma with symptoms > 4 weeks). DSM-V (i.e., Minor Neurocognitive Disorder due to Traumatic Brain Injury or Somatic Symptom Disorder).
Cognitive-behavioral model of illness (PCS) 3 Ps : o Predisposition: Biology, Psychology, or Situation that set one up for an outcome o Precipitating: The straw that broke the camel s back (injury, stress) o Perpetuation: Biology, Psychology, or Situation that maintain symptoms. Deary et al. (2007). Cog behavioral model of medically unexplained symptoms. Clinical Psychology Review. Beck (1976). Cognitive therapy and emotional disorders.
Who develops PCS? How can 2 people with mTBI have such different outcomes? -- Outcome is associated with a complex interaction among predisposing, precipitating and perpetuating variables. -- What processes are involved in the transition from acute symptoms to symptom persistence (PCS) for the miserable minority (i.e., atypical outcome of mTBI). Deary et al. (2007). Cog behavioral model of medically unexplained symptoms. Clinical Psychology Review. Beck (1976). Cognitive therapy and emotional disorders.
Predisposing Factors (Vulnerabilities) Prospective Studies* Preinjury psychiatric history* structured interview (Ponsford, 2012; Morgan et al., 2015) Family psychiatric history (Morgan et al., 2015) Preinjury ADHD (Iverson et al., 2016) Preinjury Substance Abuse (Iverson et al., 2016) Pre-injury adverse life events (Radanov, 1991) Stressful life events (Ponsford et al., 2012) Pre-injury family and personal stressors (Smyth, 2013) Combat stress (Cooper et al., 2014) and PTSD Treatments need to have targets that are modifiable.
Predisposing Factors Prospective Studies* Baseline somatic complaints* (McCrea, 2016) Preinjury health problems (Ponsford et al. 2012) Past history of concussion (Kristman et al., 2008) Migraine history (Morgan et al., 2015; Iverson et al., 2015 Nampiaparampil, 2008) Severity of injury (Dikmen, 2016; Waljas, 2015; McCrea, 2013), this is not a consistent finding. Gender (Morgan et al., 2015; Iverson et al., 2015) Genetics (APOEe4 allele; Kristman et al., 2008)
Perpetuating Factors Prospective Studies* Post-injury anxiety and depression (Ponsford, 2012; Silverberg & Iverson, 2011; Powell et al., 2019) Post traumatic stress symptoms* (Silverberg and Iverson, 2011, Belanger et al., 2011). Stressful life events* Cognitive-behavioral factors o Negative beliefs *about recovery (Mittenberg et al., 1992; Whittaker, 2007). o Expectations as etiology - misattributions (Mittenberg et al., 1992)
Perpetuating Factors Prospective Studies* Low activity level. Administration of exercise for slow to recover adolescents improved symptoms (Gagnon et al., 2009) Headache intensity (Cooper et al., 2014). Sleep disturbance (Lavigne et al., 2015) Injury severity; Acute injury characteristics* (McCrea, 2013), not a consistent finding White matter integrity (Yuh et al, 2014; Waljas et al. 2016), mixed findings o mTBI vs controls. o Mixed regarding relationship with symptoms Cognition* does not predict postconcussive symptoms in post-acute phase (Ponsford, 2012; McCrea, 2013; Cicerone, 1997).
Diathesis Stress of PCS Straw that broke the camel s back Biopsychosocial Diathesis A B Perpetuating
Symptom focused Treatment: Modifiable Targets Psychological CBT approaches, social supports Cognitive Communication Complaints cognitive rehab compensatory (Speech) Pain, fatigue, hypersensitivities (activate, light aerobic exercise, gradual exposure) Dizziness vestibular therapies Migraine (meds, CBT with mindfulness) Neurobiological risk (e.g., temperament, high autonomic arousal) psychotropics, CBT with mindfulness Structural change - ? (acute mgmt, time)
Symptom Focused Treatment of PCS
Rest ? #1 Behavioral activation is important Existing literature does not support strict rest. (Thomas et al., 2015; Silverberg & Iverson, 2012). What is appropriate?: Rest for a few days, followed by active recovery period (i.e., gradually increasing activity) (Silverberg & Iverson, 2012). Aerobic activity can facilitate symptom recovery (Makdissi et al., 2017).
Can rest be harmful? Rest can lead to avoidance Fuels preoccupation somatic preoccupation Psychological and practical impact of missing work Falling behind in school, peer relationships Physical deconditioning Mood disturbance Anxiety Isolation
Early Education and Reassurance Reassurance: through feedback, guiding objective appraisal of self, injury and recovery. Early education and reassurance is associated with lower symptom reporting after 3 6 months after mTBI (Ponsford, 2002; Mittenberg et al., 1996) and lower stress (Ponsford, 2002). Neuropsychology consultation with feedback and education component significantly reduces postconcussive symptoms at later point (Kirkwood, 2016). Borg et al. (2004) Non-Surgical Intervention MTBI; Comper et al. (2005). Review of Treatments MTBI Nygren-de Boussard et al. (2014). Non-surgical interventions after mild traumatic brain injury: A systematic review. Results of the International Collaboration on mild traumatic brain injury.
Why Cognitive Behavioral Therapy? Cognitive restructuring Self- and Injury- Appraisals Expectations as Etiology Good old Days Bias Diagnosis Threat (work, role in family, identity) Self efficacy? ( identity threat ) Behavioral activation o Re-engage in activity o Exercise o Cognitive rehab
Cognitive Behavioral Therapy Patients selected for who were At Risk for PCD. o expectations that PCS symptoms persist and have catastrophic outcomes Groups remained under care of physician at regular intervals. Randomly assigned to treatments o Education Alone 1, 3 hour session o Education+ CBT 6 sessions Silverberg et al. 2013
Cognitive Behavioral Therapy Findings (at 3 months) o % of PCS diagnoses (N=24) CBT + education = 53% Education alone = 91% Effects of CBT (effect sizes) o Personal control (large) o Post concussive symptom reporting (moderate) o Depression (moderate) o Anxiety (no effect)
Distress Tolerance CBT may not target anxiety (generalized, traumatic) as effectively as depressive symptoms. o Distress tolerance techniques are helpful, particularly for patients with significant somatic symptoms or irritable mood. Deep breathing Distraction Self-soothing
Integrated Care for mTBI Supervising Physician Specialty Consults (Headache Clinic, etc) Interdisciplinary Rehabilitation for Modifiable Symptoms. Early Education o Provide information about injury, specific symptoms, and expected recovery early. Symptom Management (OT, Speech, PT, Psych) o Physical Therapy o Cognitive Rehabilitation o Cognitive Restructuring o Psychotherapy for PTSD or distress tolerance o Sleep Hygiene o Pain Management o Biofeedback for headaches o Moderation McCrea & Powell, 2012
Summary Educate those with mTBI about their injury and what to expect about recovery as early as possible (shape expectations early). Individualized, integrated care should be considered for patients who have symptoms that persist beyond a few weeks to a month.
Select Bibliography Borg, J., Holm, L., Peloso, P. M., Cassidy, J. D., Carroll, L. J., von Holst, H., . . . Yates, D. (2004). Non-surgical intervention and cost for mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Journal of Rehabilitation Medicine (43 Suppl), 76-83. Cassidy, J. D., Carroll, L. J., Peloso, P. M., Borg, J., von Holst, H., Holm, L., . . . Coronado, V. G. (2004). Incidence, risk factors and prevention of mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Journal of Rehabilitation Medicine (43 Suppl), 28-60. Cooper, D. B., Bowles, A., A, Kennedy, J. E., Curtiss, G., French, L. M., Tate, D. F., Vanderploeg. R. D. (2016). Cognitive rehabilitation for military service members with mild traumatic brain injury: A randomized clinical trial. Head Trauma Rehabilitation, 1-15, 10.1097/HTR.0000000000000254 Deary, V, Chalder, T. Sharpe, M. (2007). The cognitive behavioural model of medically unexplained symptoms: A theoretical and empirical review. Clinical Psychology Review, 27 (7), 781-797. Giza, C. C., & Hovda, D. A. (2001). The Neurometabolic Cascade of Concussion. Journal of Athletic Training, 36(3), 228-235. Comper, P., Bisschop, S. M., Carnide, N., & Tricco, A. (2005). A systematic review of treatments for mild traumatic brain injury. Brain Injury, 19(11), 863-880. Nelson, L. D., Tarima, S., LaRoche, A. A., Hammeke, T. A., Barr, W. B., Guskiewicz, K., Randolph, C., & McCrea, M. A. (in press). Pre-injury somatization symptoms contribute to post-injury recovery after sport-related concussion. Neurology. McCrea, M. (2008). Mild traumatic brain injury and postconcussion syndrome: The new evidence base for diagnosis and treatment. New York, NY, Oxford University Press. McCrea, M., Guskiewicz, K.M., Randolph, C., Barr, W.B., Hammeke, T.A., Marshall, S.W., Powell, M.R., Ahn, K.W., Wang, Y., Kelly, J.P. Incidence, clinical course and predictors of prolonged recovery time following sport-related concussion in high school and college athletes. Journal of International Neuropsychological Society 19(1):22-33, 2013. McCrea, M., Iverson, G. L., McAllister, T. W., Hammeke, T. A., Powell, M. R., Barr, W. B., et al. (2009). An integrated review of recovery after mild traumatic brain injury (MTBI): Implications for clinical management. The Clinical Neuropsychologist, 23 (8), 1368-1390.
McCrory , P., Johnston, K., Meeuwisse, W., Aubry, M., Cantu, R., Dvorak, J., Graf-Baumann, T., Kelly, J. Lovell, M. & Schamasch, P. (2005). Summary and agreement statement of the 2nd International Conference on Concussion in Sport, Prague 2004. British Journal of Sports Medicine, 39, 196-204. Miller, L. J., & Mittenberg, W. (1998). Brief cognitive behavioral interventions in mild traumatic brain injury. Appl Neuropsychol, 5(4), 172-183. Mittenberg, W., Canyock, E. M., Condit, D., & Patton, C. (2001). Treatment of post-concussion syndrome following mild head injury. Journal of Clinical and Experimental Neuropsychology, 23(6), 829-836. Mittenberg, W., & Fischera, S. (1993). Recovery from Mild Head Injury: A treatment manual for patients. Psychotherapy in Private Practice, 12, 37-52. Mittenberg, W., Tremont, G., Zielinski, R. E., Fichera, S., & Rayls, K. R. (1996). Cognitive-behavioral prevention of postconcussion syndrome. Archives of Clinical Neuropsychology, 11(2), 139-145. National Center for Injury Prevention and Control (2003). Report to Congress on Mild Traumatic Brain Injury in the United States: Steps to Prevent a Serious Public Health Problem. Atlanta, GA: Centers for Disease Control and Prevention. Nygren-de Boussard et al. (2014). Non-surgical interventions after mild traumatic brain injury: A systematic review. Results of the International Collaboration on mild traumatic brain injury. Ownsworth, T., Fleming, J., Haines, T., Cornwell, P., Kendall, M., Nalder, E., & Gordon, C. (2011). Development of depressive symptoms during early community reintegration after traumatic brain injury. J Int Neuropsychol Soc, 17(1), 112-119. doi: 10.1017/S1355617710001311 Paniak, C., Toller-Lobe, G., Durand, A., & Nagy, J. (1998). A randomized trial of two treatments for mild traumatic brain injury. Brain Injury, 12(12), 1011-1023. Paniak, C., Toller-Lobe, G., Reynolds, S., Melnyk, A., & Nagy, J. (2000). A randomized trial of two treatments for mild traumatic brain injury: 1 year follow-up. Brain Injury, 14(3), 219-226. Ponsford, J., Willmott, C., Rothwell, A., Cameron, P., Ayton, G., Nelms, R., . . . Ng, K. (2001). Impact of early intervention on outcome after mild traumatic brain injury in children. Pediatrics, 108(6), 1297-1303. Ponsford, J., Willmott, C., Rothwell, A., Cameron, P., Ayton, G., Nelms, R., . . . Ng, K. T. (1999). Cognitive and behavioral outcome following mild traumatic head injury in children. Journal of Head Trauma Rehabilitation, 14(4), 360 372
Ponsford, J., Willmott, C., Rothwell, A., Cameron, P., Kelly, A. M., Nelms, R., & Curran, C. (2002). Impact of early intervention on outcome following mild head injury in adults. Journal of Neurology, Neurosurgery and Psychiatry, 73(3), 330-332. Ponsford, J., Willmott, C., Rothwell, A., Cameron, P., Kelly, A. M., Nelms, R., . . . Ng, K. (2000). Factors influencing outcome following mild traumatic brain injury in adults. Journal of the International Neuropsychological Society, 6(5), 568-579. Prichep, L.S., McCrea, M., Barr, W.B., Powell, M.R., Chabot, R. Time course of clinical and electrophysiological recovery following sport-related concussion. Journal of Head Trauma Rehabilitation 28(4):266-73, 2013. Rapoport, M., McCauley, S., Levin, H., Song, J., & Feinstein, A. (2002). The role of injury severity in neurobehavioral outcome 3 months after traumatic brain injury. [Clinical Trial Clinical Trial, Phase III Comparative Study Multicenter Study Research Support, Non-U.S. Gov't Research Support, U.S. Gov't, P.H.S.]. Neuropsychiatry Neuropsychol Behav Neurol, 15(2), 123- 132. Ruff, R. M., Camenzuli, L., & Mueller, J. (1996). Miserable minority: emotional risk factors that influence the outcome of a mild traumatic brain injury. Brain Injury, 10(8), 551-565. Ruff, R. M., & Richardson, A. M. (1999). Mild traumatic brain injury. In J. J. Sweet (Ed.), Forensic Neuropsychology: Fundamentals and practice. Studies on neuropsychology, development and cognition (pp. 315-338). Bristol: Swets & Seitinger. Rutland-Brown, W., Langlois, J. A., Thomas, K. E., & Xi, Y. L. (2006). Incidence of traumatic brain injury in the United States, 2003. J Head Trauma Rehabil, 21(6), 544-548. Teasdale, G. & Jennett, B. (1974). Assessment of coma and impaired consciousness: A practical scale. The Lancet, 2 (7872), 81-84. Williams, D. H., Levin, H. S., & Eisenberg, H. M. (1990). Mild head injury classification. Neurosurgery, 27 (3), 422-428.















")

")