Understanding Periodontal Flap Techniques
Explore the classification and techniques of periodontal flaps for pocket therapy, including modified Widman flap, undispaced flap, and more. Learn about the importance of flap thickness, bone exposure, flap placement, and flap design in periodontal surgery. Discover the different types of pockets and their relation to crestal bone, as well as the number of tooth surfaces involved in periodontal conditions.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Done by ANAGHA . K M CRRI DEPARMENT OF PERIODONTICS
DEFINITION CLASSIFICATION OF FLAP FLAP TECHNIQUES FOR POCKET THERAPY MODIFIED WIDMAN FLAP UNDISPLACED FLAP APICALLY DISPLACED FLAP HEALING AFTER FLAP SURGERY
Periodontal flap is the section of gingiva or mucosa surgically- elevated from the underlying tissue to provide visibility of and access to the bone and root surface
ACCORDING TO THE THICKNES OF THE FLAP/ BONEEXPOSURE AFTER FLAP REFLECTION Full thickness flap/ mucoperiosteal flap: All the soft tissue including the periosteum Indication: if osseous surgery is contemplated Partial thickness/ mucosal flap / split thickness flap: Epithelium and a layer of underlying connective tissue Indication: displacing flap in case of dehiscence and fenestrations
ACCORDING TO THE PLACEMENT OF FLAP AFTER SURGERY Non displaced flap: flap is returned and sutured back in its original position. Displaced flap: repositioned coronal apical or lateral to its original position
ACCORDING TO DESIGN OF THE FLAP/ MANAGEMENT OF THE PAPILLA Conventional flap: splitting the papilla into a facial half and lingual/ palatal half Indication: interdental areas are too narrow Papilla prevention flap: entire papilla is incorperated into one of the flap Indication: esthetic is concern bone regeneration technique are attempt
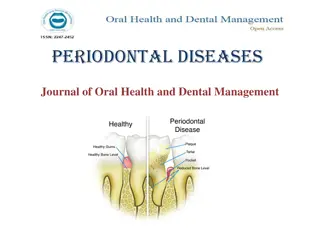
MORPHOLOGY 1. gingival/false/relative pocket 2. periodontal/absolute/true pocket 3. combined pocket
RELATIONSHIP TO CRESTAL BONE suprabony/supracrestal/supra-alveolar pocket Infrabony/intrabony/subcrestal/intra-alveolar pocket 1. 2. NUMBER OF SURFACE INVOLVED Simple pocket- involving one tooth surface Compound pocket- involving two or more surface Complex pocket- where the base of the pocket is not in direct communication with the gingival margin. It is also known as spiral pocket 1. 2. 3.
NATURE OF SOFT TISSUE WALL OF THE POCKET Edematous pocket Fibrotic pocket 1. 2. DISEASE ACTIVITY Active pocket Inactive pocket 1. 2.
FOR CONVENTIONAL FLAP 1. Horizontal Incision internal bevel incision crevicular incision inter dental incision 2. Vertical incision oblique releasing incision FOR PAPILLARY PRESERVATION FLAP crevicular incision with no incision across the interdental papilla is given
INTERNAL BEVEL INCISION Basic incision to most of the flap procedure Starts at a distance from the gingival margin and is aimed at the bone crest EXTERNAL BEVEL INCISION: done for gingivectomy CREVICULAR INCISION : base of the pocket to the crest of the crest of the bone VERTICAL INCISION: can be done one or both ends of the horizontal incision.
Periodontal flap is one of the most employed procedure for elimination or reducing moderate to deep pocket in posterior areas Flap technique are MODIFIED WIDMAN FLAP UNDISPLACED FLAP APICALLY- DISPLACED FLAP
Presented in 1974 by Ramfjord and Nissle PROCEDURE
Here entire soft tissue pocket wall is removed with initial incision Attached gingiva should be remain after removal of the pocket wall PROCEDURE: 1. Internal bevel incision 2. Crevicular incision 3. Flap reflected
4. Inter dental incision 5. The area is debrided, and remove all granulation tissue. 6. Scaling and root planning 7. Continues sling suture is placed 8. Placement of periodontal pack
Used for both pocket eradiation and widening the zone of attached gingiva. PROCEDURE
Immediately after suturing, connection between the flap and the tooth or bone surface is established by the blood clot Clot consist of a fibrin reticulum with many polymorphonuclear leukocyte, erythrocyte, debris from injured cells and capillaries at the edge of the wound
ONE TO THREE DAYS AFTER FLAP SURGERY: Space between the flap and the tooth or bone is thinner and epithelial cell migrate over the border of the flap, when flap is closely adapted to the alveolar process there is only a minimal inflammatory response. ONE WEEK AFTER FLAP SURGERY: An epithelial attachment to the root has been established by means of hemidesmosomes and a basal lamina. The blood clot is replaced by granulation tissue derived from gingival connective tissue, bone marrow and the periodontal ligament.
TWO WEES AFTER SURGERY: Collagen fibers begins to appear paralelto the tooth surface . Union of the flap and the to tooth is still weak but clinicaly it appear almost normal ONE MONTH AFTER SURGERY: A fully epithelized gingival crevice with a well defined attachment is present Supracreastel fibers begins to adapt a functional arrangement
THANK YOU ..