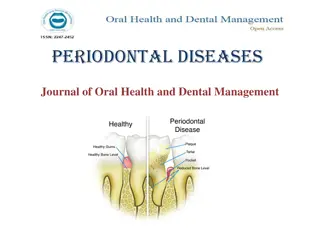
Understanding the Impact of Stress on Periodontal Health
STRESS ON PERIODONTIUM
Dr.Radhika.,M.D.S
Dept of Periodontology
CONTENTS
Introduction
Stress definition
Stress as a common pathway for chronic disease
Possible mechanisms of action of stress on periodontal tissues
Bi-directional effect of stress
Stress induced changes in leukocyte distribution
Effects of stress on periodontium
Impact of stress on the development of severity of periodontitis
Effects of stress on periodontal treatment
Effects of stress on wound healing
Stress on subgingival microflora
Oxidative stress
Clinical implications of stress on periodontal practice
Management
Conclusion
References
INTRODUCTION
Periodontitis is a multifactorial disease in which dental
plaque harbors specific periodontal pathogens as its primary
etiological factor .In addition to this there are several risks
and susceptibilities associated with periodontitis like systemic
diseases, some genetic polymorphisms, socio-economic status
,psychological stress.
chronic stress is commonly thought to have a negative
effect on the efficacy of the Immune response ,leading to
imbalance between host and parasites, which consequently
resulting in periodontal breakdown.
For necrotizing periodontitis , stress has been shown to represent a
secondary etiological factor. Many studies proved that stress may play
a major role in the development of periodontal disease,
Linden et al 1996
suggested a relation ship between occupational
stress and progression of periodontitis
DEFINITION
Stress is defined as a state of physiological or psychological strain
caused by an adverse stimuli, physical, mental or emotional,
internal or external that tend to disturb the functioning of an
organism and which the organism naturally desires to avoid.
(GPT 4
th
edition)
Stress can be defined as the psychological response of an
organism to a perceived threat or challenge.
(Breivik et al 1996)
•
Selye et al 1936
proposed that the hypothalamus-pituitary adrenal
cortex axis (HPA axis) response to stress was beneficial in short
term, however prolonged stress was detrimental to the body by
diminishing its ability to respond to a perceived challenge a
termed as
General adaptation syndrome.
•
Stress can be based (involuntary stress ,voluntary stress)and also
stress can be physiological or psychological stress.
STRESS AS A COMMOM
PATHWAY FOR CHRONIC
DISEASES
•
Psychological stress impact the periodontal disease through
alterations in immune system.
•
Stress related immune system changes clearly have the potential
to affect the pathogenesis of periodontal disease as well.
•
Stress can modulate immune system through the neural and
endocrine systems by
production of cortisol.
Autonomic nervous system pathways.
Release of neuropeptides.
Alteration of Th1/Th2 cells.
Production of cortisol / HPA axis:
Autonomic nervous system pathways:
•
It is the second pathway to be activated by the stress
•
Emotional stress results in the release of adrenaline and
noradrenaline from the cells of adrenal medulla.
Release of neuropeptides/neurotransmitters:
•
Stress may effect the cellular immune response directly through
an increased level of neurotransmitters (epinephrine,
norepinephrine, neurokinin, substance p) which will further
interact with lymphocytes, neutrophils, monocytes via receptors
causing increase in tissue destruction.
Alteration in Th1/Th2 cell ratio:
•
Th1 stimulate cellular immunity through increase in IL-2,
Interferons (protective)
•
Th2 stimulate humoral immunity through the release of IL-
4,5,6,10(destructive)
•
Marshall et al
demonstrated Th2 cell response increase in
stressful conditions.
•
Stress increases cortisol increases Th2 response(Breivik et
al)
POSSIBLE MECHANISMS OF ACTION OF STRESS ON
PERIODONTAL TISSUES
Neglect of oral hygiene results in plaque accumulation
which is detrimental to periodontal tissue
Change in dietary intake(over eating) Immunosuppression
through increase in cortisol.
Smoking and other harmful oral habits circulating nicotine
results in vasoconstriction due to release of adrenaline causing
suppression of secondary antibody responses, inhibition of
neutrophil function)
Bruxism (which is taught to be induced by stress)
Gingival circulation(stress causes constriction of blood vessels
which eventually decreases utilization of oxygen)
Alteration in saliva flow and components increase or decrease
in saliva adversely affect periodontium, changes chemical
composition, pH of the saliva)
Lowered host resistance Release of adrenaline/noradrenaline
induce a decrease in blood flow and decrease blood elements
necessary for maintaining resistance to microbes(increases IL-
10,decreases IL-12)
Psychological stress
Behavioral change
Poor oral hygiene Over eating
Poor compliance
Smoking
Bacterial infection
cortisol
Decreased
immunity
Periodontal
disease
BI-DIRECTIONAL EFFECT OF STRESS
•
Immunosuppressive,mainly in chronic stress which suppress
the recruitment of leukocyte from blood to skin)
•
Immunoenhancement, mainly in acute stress which
stimulate major recruitment of leukocytes from blood to
skin)
•
These physiological changes are normally adaptive when
stress is acute, but can result in damage when stress is
chronic and long term.
STRESS
STRESS INDUCED CHANGES IN LEUKOCYTE
DISTRIBUTION
•
Change in either the expression /affinity of surface adhesion
molecules on leukocyte/ on endothelial cells.
•
Specific leukocyte populations retains in those compartments
provided that they encounter a glucocorticoid-induced adhesion
match on the endothelial cells decrease in the leukocyte in blood.
•
Glucorticosteriods influence the production of cytokines,
lipocortins, which affect the ability of leukocyte endothelial
adhesion properties.
EFFECTS OF STRESS ON PERIODONTIUM
Stress may affect the periodontium directly/indirectly
DIRECT
Alteration of
resistance of
periodontium to
infection
INDIRECT
Psychological aspect of
person with behavioural
changes like poor oral
hygiene,smoking
,bruxism etc.
Gingivitis
Stress diminishes saliva flow and chemical composition
and increase plaque formation.
Deinzer et al
( stress was shown to be a risk factor for
gingival inflammation with increasing crevicular IL-1
β
levels and a diminution of the quality of oral hygiene.)
Axtelius et al
showed the presence of cortisol in the
gingival crevicular fluid is higher by person showing
depression signs.
ANUG and stress
ANUG is the most studied periodontal disorder in relation
to psychosocial factor.
Psychological factors probably predispose to the disease
by favoring bacterial growth/weakening host resistance
ANUG patients presented by decrease in PMN’S
chemotaxis ,phagocytosis, reduced proliferation of
lymphocytes.
Host tissue resistance may change during stress by acting
through ANS and endocrine glands and increases the cortisol
adrenaline, noradrenaline which reduce gingival micro
circulation and salivary flow and increase
prevotella intermedia
and at the same time depresses the neutrophils ,lymphocytes
functions which facilitates bacterial invasion and tissue damage.
Presence of ANUG in soldiers stressed by war time
conditions in the trenches led to one of the early
diagnostic term named as
“Trench mouth”
.
( a study by
pinborg et al 1951).
Stress and aggressive periodontitis
There is a link existing between aggressive periodontitis and
psychosocial factors and loss of appetite
(Page et al 1983).
A case control study on 1196 subjects showed people with
aggressive periodontitis were more depressed and socially
isolated than people with chronic periodontitis / control
group
.(Monterio silva et al 1996)
Chronic periodontitis
Axtelius
has suggested that patients with psychosocial strain did
not respond well with periodontal treatment as compared to non
stressed individuals.
Genco et al
in cross-sectional study assessed role of stress
causing greater alveolar bone loss and periodontal attachment
loss.
•
Belting and Gupta (1961)
using the Russell Periodontal
Index, found that periodontal disease was more severe in the
psychiatric patients as compared to controls when oral
hygiene frequency, level of calculus, age, bruxism and
clenching were held constant.
IMPACT OF STRESS ON THE DEVELOPMENT
AND SEVERITY OF PERIODONTITIS
Immune cell response plays a crucial role in the healing of
periodontal tissues, some cytokines, Interleukins, TNF-
α
are
involved in the repair of the injured site and regulate the
production of fibroblasts and epithelial cells.
In a stressed subject with periodontitis the production rate is
high, resulting in an increase in the severity of periodontal
damage.
Studies have shown that some hormones released under stress
cause a proliferation of certain bacteria such as
“Fusobacterium nucleatum”
there fore aggravating the
severity of periodontal damage.
Animal studies have shown a link between stress and
bFGF(basic fibroblast growth factor)
and the severity of
periodontitis .Individuals with an inadequate stress response
also have a decreased response to non surgical periodontal
treatments than other patients.
Lu et al
stated that there will be stress- induced ANS
stimulation, which results in the release of neurotransmitters
which are capable of binding to
α
1 adrenergic receptors
present on the surface of periodontal cells .Thus decreasing
biological activity and causing a massive release of
inflammatory factors .
STRESS ON PERIODONTAL TREATMENT
Kamma and baehni
et al found that supportive periodontal
care was more effective in patients with aggressive
periodontitis having less stress.
Stress impairs the inflammatory response and matrix
degradation after surgery.
Greater psychological stress significantly associated with
lower levels of IL-2 and MMP-2 as well as significantly
more painful, poorer and show slow recovery.
Studies shows that increase GCF elastase levels in
stressed patients with non surgical periodontal therapy.
Wimmer et al
demonstrated that patients with
maladaptive coping with stress have more advanced
disease and poor response to a non surgical periodontal
treatment.
EFFECTS OF STRESS ON WOUND HEALING
Stress releases highly active hormones like catecholamine,
which results in altered blood flow, peripheral
vasoconstriction may affect oxygen dependent healing
mechanisms which impairs wound healing.
Results in
I.
Hyperglycemia--- impairs neutrophil formation and
impairs initial phase of wound healing.
II.
Decrease level of growth factors.
III.
Decrease MMP level,which impairs tissue turn over .
IV.
Alters cytokine profile.
EFFECT OF STRESS ON SUBGINGIVAL
MICROFLORA
In an recent study of the levels of sub gingival micro flora in adult
smokers with periodontitis found higher levels of
Prevotella
Intermedia , peptostrepto coccus micros, Fusobacterium nucleatum,
Bacteriods forsythus ,Campylobacter rectus.
Stress can stimulate a 10-fold increase the catecholamine release
like epinephrine, noradrenaline which may serve as biological signals
to modify the growth of individual organisms within subgingival
biofilms.
Numerous
Actinomycetes species, streptocoocus
show
accelerated growth due to catecholamines
Two organisms which are important in the pathogenesis
of NUG are
F.nucleatum, ssp vincentii
which demonstrate
an increase in growth under the influence of adrenaline
and
P. intermedia
which revealed a trend for increased
growth.
It also suggests that these catecholamines cause
destabilization of iron binding by proteins(eg:
transferrin,lactoferrin) there by assisting iron uptake by
microbes.
ROLE OF OXIDATIVE STRESS IN
PERIODONTITIS
Oxidative stress is an imbalance between oxidants and anti
oxidants.
Oxidative stress is a key driver of chronic inflammation and as
a result has a central role in the pathogenesis of a wide range
of chronic inflammatory diseases.
It can cause tissue damage by altering molecules such as
proteins, lipids, DNA. Thus damaging cells directly/indirectly
that leads to downstream of gene expression changes and
production of pro-inflammatory molecules.
Generation of ROS by
fibroblasts, PMNL’S
Oxidative
stress
Release of inflammatory mediators
Inactivation of TIMPS
Recruitment and activation of hyper
responsive PMNL
Periodontal tissue damage
CLINICAL IMPLICATIONS OF STRESS IN
PERIODONTAL PRACTICE
Evaluate stress status in patients with periodontal disease.
Provide information on possible association to patients
Address indirect effects/habits induced by stress (smoking,
poor oral hygiene.
Avoid surgical treatment during acute phases of stress
Referral to physician/psychiatrist for counseling.
MANAGEMENT
Periodontal management
careful case history.
Debridement of root surfaces.
Optimizing oral hygiene.
Utilization of anti microbial substances.
Adjunct use of growth factors in various delivery
vehicles
.
Stress management
Removal /alteration of the source of stress
Learning alternate ways of coping
Reducing the effect on your body that causing
stress
Learning to change how you see the stressful
event
CONCLUSION
Stress could be a contributing factor in the process of
periodontal destruction in the presence of periodontal
pathogens in susceptible individuals and it is associated
with more severe disease as well as delayed healing response
to traditional periodontal surgery.
Assessing the patient stress level during periodontal
treatment may be valuable in providing another prognostic
tool.
REFERENCES
1.
Clinical periodontology, Carranza, 10
th
edition.
2.
The role of stress in periodontal disease and wound healing,
periodontitis 2000,vol.44,2007,195-210.
3.Carranza's Clinical Periodontology – 11th edition.
4.Jan Lindhe – Clinical Periodontology and Implant Dentistry – 4th
edition.
5.Shalu Chandna,Manish Bathla : Stress and Periodontium-A
review of concept, JOHCD 4:17-22, 2010.
6.Malathi , Dhanesh Sabale : Stress And Periodontitis-A review ,
IOSR-JDMS 9:4, 2012.
7.Satheesh Mannem , Vijay K Chava : The effect of stress on
periodontitis, Journal of Indian Society Of Periodontology
16:365-369, 2012.
8.Sachin Goyal, Garima Gupta, Besty Thomas : Stress and
Periodontal disease-The link and logic, Industrial Psychiatry
Journal 22:4-11, 2013.
9.The role of stress in periodontal disease and wound healing,
Periodontology 2000, Vol. 44, 2007, 195–210
10. Emotional stress effects on immunity, gingivitis and
periodontitis,EurJOralSci1996:104:327-334
11. Stress, Depression, Cortisol, and Periodontal Disease, J
Periodontol 2009;80:260-266
12. Effects of academic stress on oral hygiene – a potential link
between stress and plaque associated diseaseJ Clin Periodontol 2001;
28: 459–464
13. Psychosocial stress, lifestyle and periodontal health, J Clin
Periodontol 2002; 29: 3214. Psychosocialfactors in inflammatory
periodontal diseases, /ClinPeriodontol1995:22:516-526
15. Chromogranin A: Novel biomarker between periodontal disease
and psychosocial stress, Journal of Indian Society of Periodontology-
Vol 17, Issue 2, Mar-Apr 2013
16. Models to Evaluate the Role of Stress in Periodontal Disease,
Ann Periodontol 1998;3: 288-302.
17.coping with stress, its influence on periodontal diseases,J
Periodontal,2002,73,1343-1351.
6–335
Periodontitis is a complex disease influenced by various factors, including stress. Chronic stress can negatively affect the immune response, leading to periodontal breakdown. This article explores the relationship between stress and periodontal health, discussing the mechanisms of action, effects on leukocyte distribution, impact on severity of periodontitis, treatment outcomes, wound healing, subgingival microflora, and oxidative stress. Management strategies and clinical implications are also addressed.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
STRESS STRESS ON ON PERIODONTIUM PERIODONTIUM Dr.Radhika.,M.D.S Dept of Periodontology
CONTENTS Introduction Stress definition Stress as a common pathway for chronic disease Possible mechanisms of action of stress on periodontal tissues Bi-directional effect of stress Stress induced changes in leukocyte distribution Effects of stress on periodontium Impact of stress on the development of severity of periodontitis Effects of stress on periodontal treatment Effects of stress on wound healing Stress on subgingival microflora Oxidative stress Clinical implications of stress on periodontal practice Management Conclusion References
INTRODUCTION Periodontitis is a multifactorial disease in which dental plaque harbors specific periodontal pathogens as its primary etiological factor .In addition to this there are several risks and susceptibilities associated with periodontitis like systemic diseases, some genetic polymorphisms, socio-economic status ,psychological stress. chronic stress is commonly thought to have a negative effect on the efficacy of the Immune response ,leading to imbalance between host and parasites, which consequently resulting in periodontal breakdown.
For necrotizing periodontitis , stress has been shown to represent a secondary etiological factor. Many studies proved that stress may play a major role in the development of periodontal disease, Linden et al 1996 suggested a relation ship between occupational stress and progression of periodontitis
DEFINITION Stress is defined as a state of physiological or psychological strain caused by an adverse stimuli, physical, mental or emotional, internal or external that tend to disturb the functioning of an organism and which the organism naturally desires to avoid. (GPT 4th edition) Stress can be defined as the psychological response of an organism to a perceived threat or challenge. (Breivik et al 1996)
Selye et al 1936 proposed that the hypothalamus-pituitary adrenal cortex axis (HPA axis) response to stress was beneficial in short term, however prolonged stress was detrimental to the body by diminishing its ability to respond to a perceived challenge a termed as General adaptation syndrome. Stress can be based (involuntary stress ,voluntary stress)and also stress can be physiological or psychological stress.
STRESS STRESS AS AS A A COMMOM COMMOM PATHWAY PATHWAY FOR FOR CHRONIC CHRONIC DISEASES DISEASES
Psychological stress impact the periodontal disease through alterations in immune system. Stress related immune system changes clearly have the potential to affect the pathogenesis of periodontal disease as well. Stress can modulate immune system through the neural and endocrine systems by production of cortisol. Autonomic nervous system pathways. Release of neuropeptides. Alteration of Th1/Th2 cells.
Autonomic nervous system pathways: It is the second pathway to be activated by the stress Emotional stress results in the release of adrenaline and noradrenaline from the cells of adrenal medulla.
Release of neuropeptides/neurotransmitters: Stress may effect the cellular immune response directly through an increased level of neurotransmitters (epinephrine, norepinephrine, neurokinin, substance p) which will further interact with lymphocytes, neutrophils, monocytes via receptors causing increase in tissue destruction.
Alteration in Th1/Th2 cell ratio: Th1 stimulate cellular immunity through increase in IL-2, Interferons (protective) Th2 stimulate humoral immunity through the release of IL- 4,5,6,10(destructive) Marshall et al demonstrated Th2 cell response increase in stressful conditions. Stress increases cortisol increases Th2 response(Breivik et al)
POSSIBLE MECHANISMS OF ACTION OF STRESS ON PERIODONTAL TISSUES Neglect of oral hygiene results in plaque accumulation which is detrimental to periodontal tissue Change in dietary intake(over eating) Immunosuppression through increase in cortisol. Smoking and other harmful oral habits circulating nicotine results in vasoconstriction due to release of adrenaline causing suppression of secondary antibody responses, inhibition of neutrophil function)
Bruxism (which is taught to be induced by stress) Gingival circulation(stress causes constriction of blood vessels which eventually decreases utilization of oxygen) Alteration in saliva flow and components increase or decrease in saliva adversely affect periodontium, changes chemical composition, pH of the saliva) Lowered host resistance Release of adrenaline/noradrenaline induce a decrease in blood flow and decrease blood elements necessary for maintaining resistance to microbes(increases IL- 10,decreases IL-12)
Psychological stress Behavioral change Poor oral hygiene Over eating Poor compliance Smoking Bacterial infection cortisol Decreased immunity Periodontal disease
BI-DIRECTIONAL EFFECT OF STRESS Immunosuppressive,mainly in chronic stress which suppress STRESS STRESS the recruitment of leukocyte from blood to skin) Immunoenhancement, mainly in acute stress which stimulate major recruitment of leukocytes from blood to skin) These physiological changes are normally adaptive when stress is acute, but can result in damage when stress is chronic and long term.
STRESS INDUCED CHANGES IN LEUKOCYTE DISTRIBUTION Change in either the expression /affinity of surface adhesion molecules on leukocyte/ on endothelial cells. Specific leukocyte populations retains in those compartments provided that they encounter a glucocorticoid-induced adhesion match on the endothelial cells decrease in the leukocyte in blood. Glucorticosteriods influence the production of cytokines, lipocortins, which affect the ability of leukocyte endothelial adhesion properties.
EFFECTS OF STRESS ON PERIODONTIUM Stress may affect the periodontium directly/indirectly Alteration of resistance of periodontium to infection DIRECT Psychological aspect of person with behavioural changes like poor oral hygiene,smoking ,bruxism etc. INDIRECT
Gingivitis Stress diminishes saliva flow and chemical composition and increase plaque formation. Deinzer et al ( stress was shown to be a risk factor for gingival inflammation with increasing crevicular IL-1 levels and a diminution of the quality of oral hygiene.) Axtelius et al showed the presence of cortisol in the gingival crevicular fluid is higher by person showing depression signs.
ANUG and stress ANUG is the most studied periodontal disorder in relation to psychosocial factor. Psychological factors probably predispose to the disease by favoring bacterial growth/weakening host resistance ANUG patients presented by decrease in PMN S chemotaxis ,phagocytosis, reduced proliferation of lymphocytes.
Host tissue resistance may change during stress by acting through ANS and endocrine glands and increases the cortisol adrenaline, noradrenaline which reduce gingival micro circulation and salivary flow and increase prevotella intermedia and at the same time depresses the neutrophils ,lymphocytes functions which facilitates bacterial invasion and tissue damage. Presence of ANUG in soldiers stressed by war time conditions in the trenches led to one of the early diagnostic term named as Trenchmouth . ( a study by pinborg et al 1951).
Stress and aggressive periodontitis There is a link existing between aggressive periodontitis and psychosocial factors and loss of appetite (Page et al 1983). A case control study on 1196 subjects showed people with aggressive periodontitis were more depressed and socially isolated than people with chronic periodontitis / control group.(Monterio silva et al 1996)
Chronic periodontitis Axtelius has suggested that patients with psychosocial strain did not respond well with periodontal treatment as compared to non stressed individuals. Genco et al in cross-sectional study assessed role of stress causing greater alveolar bone loss and periodontal attachment loss.
Belting and Gupta (1961) using the Russell Periodontal Index, found that periodontal disease was more severe in the psychiatric patients as compared to controls when oral hygiene frequency, level of calculus, age, bruxism and clenching were held constant.
IMPACT OF STRESS ON THE DEVELOPMENT AND SEVERITY OF PERIODONTITIS Immune cell response plays a crucial role in the healing of periodontal tissues, some cytokines, Interleukins, TNF- are involved in the repair of the injured site and regulate the production of fibroblasts and epithelial cells. In a stressed subject with periodontitis the production rate is high, resulting in an increase in the severity of periodontal damage.
Studies have shown that some hormones released under stress cause a proliferation of certain bacteria such as Fusobacterium nucleatum there fore aggravating the severity of periodontal damage. Animal studies have shown a link between stress and bFGF(basic fibroblast growth factor)and the severity of periodontitis .Individuals with an inadequate stress response also have a decreased response to non surgical periodontal treatments than other patients.
Lu et al stated that there will be stress- induced ANS stimulation, which results in the release of neurotransmitters which are capable of binding to 1 adrenergic receptors present on the surface of periodontal cells .Thus decreasing biological activity and causing a massive release of inflammatory factors .
STRESS ON PERIODONTAL TREATMENT Kamma and baehni et al found that supportive periodontal care was more effective in patients with aggressive periodontitis having less stress. Stress impairs the inflammatory response and matrix degradation after surgery. Greater psychological stress significantly associated with lower levels of IL-2 and MMP-2 as well as significantly more painful, poorer and show slow recovery.
Studies shows that increase GCF elastase levels in stressed patients with non surgical periodontal therapy. Wimmer et al demonstrated that patients with maladaptive coping with stress have more advanced disease and poor response to a non surgical periodontal treatment.
EFFECTS OF STRESS ON WOUND HEALING Stress releases highly active hormones like catecholamine, which results in altered blood flow, peripheral vasoconstriction may affect oxygen dependent healing mechanisms which impairs wound healing. Results in I. Hyperglycemia--- impairs neutrophil formation and impairs initial phase of wound healing. II. Decrease level of growth factors. III. Decrease MMP level,which impairs tissue turn over . IV. Alters cytokine profile.
EFFECT OF STRESS ON SUBGINGIVAL MICROFLORA In an recent study of the levels of sub gingival micro flora in adult smokers with periodontitis found higher levels of Prevotella Intermedia , peptostrepto coccus micros, Fusobacterium nucleatum, Bacteriods forsythus ,Campylobacter rectus. Stress can stimulate a 10-fold increase the catecholamine release like epinephrine, noradrenaline which may serve as biological signals to modify the growth of individual organisms within subgingival biofilms.
Numerous Actinomycetes species, streptocoocus show accelerated growth due to catecholamines Two organisms which are important in the pathogenesis of NUG are F.nucleatum, ssp vincentii which demonstrate an increase in growth under the influence of adrenaline and P. intermedia which revealed a trend for increased growth. It also suggests that these catecholamines cause destabilization of iron binding by proteins(eg: transferrin,lactoferrin) there by assisting iron uptake by microbes.
ROLE OF OXIDATIVE STRESS IN PERIODONTITIS Oxidative stress is an imbalance between oxidants and anti oxidants. Oxidative stress is a key driver of chronic inflammation and as a result has a central role in the pathogenesis of a wide range of chronic inflammatory diseases. It can cause tissue damage by altering molecules such as proteins, lipids, DNA. Thus damaging cells directly/indirectly that leads to downstream of gene expression changes and production of pro-inflammatory molecules.
Oxidative stress Generation of ROS by fibroblasts, PMNL S Release of inflammatory mediators Inactivation of TIMPS Recruitment and activation of hyper responsive PMNL Periodontal tissue damage
CLINICAL IMPLICATIONS OF STRESS IN PERIODONTAL PRACTICE Evaluate stress status in patients with periodontal disease. Provide information on possible association to patients Address indirect effects/habits induced by stress (smoking, poor oral hygiene. Avoid surgical treatment during acute phases of stress Referral to physician/psychiatrist for counseling.
MANAGEMENT Periodontal management careful case history. Debridement of root surfaces. Optimizing oral hygiene. Utilization of anti microbial substances. Adjunct use of growth factors in various delivery vehicles.
Stress management Removal /alteration of the source of stress Learning alternate ways of coping Reducing the effect on your body that causing stress Learning to change how you see the stressful event
CONCLUSION Stress could be a contributing factor in the process of periodontal destruction in the presence of periodontal pathogens in susceptible individuals and it is associated with more severe disease as well as delayed healing response to traditional periodontal surgery. Assessing the patient stress level during periodontal treatment may be valuable in providing another prognostic tool.
REFERENCES 1. Clinical periodontology, Carranza, 10th edition. 2. The role of stress in periodontal disease and wound healing, periodontitis 2000,vol.44,2007,195-210. 3.Carranza's Clinical Periodontology 11th edition. 4.Jan Lindhe Clinical Periodontology and Implant Dentistry 4th edition. 5.Shalu Chandna,Manish Bathla : Stress and Periodontium-A review of concept, JOHCD 4:17-22, 2010. 6.Malathi , Dhanesh Sabale : Stress And Periodontitis-A review , IOSR-JDMS 9:4, 2012.
7.Satheesh Mannem , Vijay K Chava : The effect of stress on periodontitis, Journal of Indian Society Of Periodontology 16:365-369, 2012. 8.Sachin Goyal, Garima Gupta, Besty Thomas : Stress and Periodontal disease-The link and logic, Industrial Psychiatry Journal 22:4-11, 2013. 9.The role of stress in periodontal disease and wound healing, Periodontology 2000, Vol. 44, 2007, 195 210 10. Emotional stress effects on immunity, gingivitis and periodontitis,EurJOralSci1996:104:327-334
11. Stress, Depression, Cortisol, and Periodontal Disease, J Periodontol 2009;80:260-266 12. Effects of academic stress on oral hygiene a potential link between stress and plaque associated diseaseJ Clin Periodontol 2001; 28: 459 464 13. Psychosocial stress, lifestyle and periodontal health, J Clin Periodontol 2002; 29: 3214. Psychosocialfactors in inflammatory periodontal diseases, /ClinPeriodontol1995:22:516-526 15. Chromogranin A: Novel biomarker between periodontal disease and psychosocial stress, Journal of Indian Society of Periodontology- Vol 17, Issue 2, Mar-Apr 2013
16. Models to Evaluate the Role of Stress in Periodontal Disease, Ann Periodontol 1998;3: 288-302. 17.coping with stress, its influence on periodontal diseases,J Periodontal,2002,73,1343-1351. 6 335















")










 using the Russell")