Periodontal Response to External Forces in Periodontics

Adaptive capacity of the periodontium in response to occlusal forces is variable, influenced by factors like magnitude, direction, duration, and frequency. Trauma from occlusion occurs when occlusal forces exceed tissue's adaptive capacity, leading to tissue injury. It is classified into acute and chronic types, with manifestations like tooth pain, mobility, and discomfort. Acute trauma may cause tooth sensitivity and pain, while chronic trauma involves gradual changes due to factors like tooth wear, drifting, and parafunctional habits.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
PERIODONTAL RESPONSE TO EXTERNAL FORCES DR. A. CHAITANYA, READER SIBAR INSTITUTE OF DENTAL SCIENCES DEPARTMENT OF PERIODONTICS
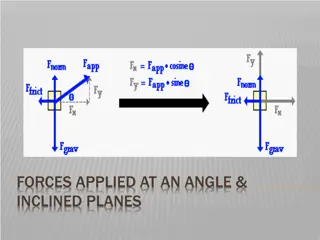
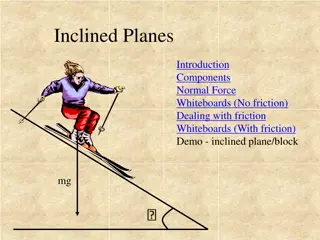
INTRODUCTION Adaptivecapacityof periodontium toforces exertedisvariable Occlusalforces Magnitude Direction Duration Frequency Magnitude -wideningof the PDLspace -increasein the no.&width of PDLfibers -increasein the densityofalveolarbone
Direction -Reorientation of stress &strain -Principal fibers of PDL Occlusal forces along the long axis of thetooth -Lateral/Horizontal &Torque/Rotational: Injure the periodontium Duration -Constant pressure >intermittent Frequency -Frequent application of intermittentforce: injurious
TRAUMA FROM OCCLUSION DEFINITION Whenocclusalforcesexceedthe adaptive capacityof the tissues,tissue injury results. Theresultantinjury istermedastraumafrom occlusion An occlusion that produces forces that cause an injury to the attachment apparatus -Carranza
CLASSIFICA TION I. Acute &Chronic II. Primary &Secondary
ACUTE TFO Causes: An abrupt occlusalimpact Restorations/prosthetic appliances Manifestations: Toothpain Sensitivity topercussion Increased toothmobility
Forcedissipated i. ii. Shift in toothposition Wearing heals & subsides iii. Correction ofrestoration Orelse Periodontalinjury Necrosis+ periodontalabscess or Cementumtears
CHRONIC TFO More common&significant Gradualchangesby: - toothwears - drifting movement&extrusion - parafunctionalhabits
PRIMARY TFO Definition: Injuryresultingintissuechangesfromexcessive occlusalforcesappliedtoatoothor teethwith normalsupport
Causes Highfilling Prostheticreplacement Drifting/ extrusion Orthodontic movement into functionally unacceptable positions Primary TFO - no changes in connective tissue attachment level & no pocket formation
SECONDARY TFO Definition Injuryresultingintissuechangesfromnormalor excessiveocclusalforcesappliedto a tooth withreducedsupport
THREE STAGES OF TFO 1. INJURY 2. REPAIR 3. ADAPTIVE REMODELING OF THE PERIODONTIUM
I NJU R Y Excessive Occlusal forces: Tissue Injury Repair of injury & Restoration of periodontium if- i. Forces are diminished ii. Tooth drifts away from them
Occlusalforces:Toothrotation arounda Fulcrum/AxisofRotation Junctionofmiddle& apicalthirdofclinical root Areasof pressure& tensioncreatedon oppositesidesof thefulcrum
SLIGHTLY EXCESSIVE PRESSURE Resorptionof the alveolarbone Numerous blood vessels-reduced insize SLIGHTLY EXCESSIVE TENSION Elongation of the PDLfibers Apposition of alveolarbone Enlarged bloodvessels
GREATER PRESSURE GradationofChanges Compressionof fibers Areasofhyalinization Injury to fibroblasts&other cells:Necrosisof PDL Vascular changes occurs within 30minutes
Impairment&stasisofbloodflow in2-3hours bloodvesselspackedwith RBC sfragment in 1-7days disintegrationof bloodvesselwalls-contents dischargedinto the surrounding tissues Increasedresorptionof alveolarbone& toothsurface
SEVERE TENSION WideningofPDL Thrombosis Haemorrhage Tearingof thePDL Resorptionof the alveolarbone
SEVERE PRESSURE Forcethe root againstbone Necrosisof the PDL&bone Undermining Boneresorptionfrom viablePDL& marrow spaces Resorption Mostsusceptibleareasof Injury-Furcations
REPAIR Normalperiodontium: Constantrepair TFO-increasedreparativeactivity Damagedtissuesremoved& formationofnew Cells Fibers Bone Cementum
Forces are traumatic as long as injury exceeds the repair Boneresorbedbyexcessiveocclusalforces Thinnedbonytrabeculaereinforcedwithnew bone Buttressing bone formation: Important featureof RepairafterTFO Central buttressing: Occurs within thejaw Newbonedeposition
Peripheral buttressing: Facial& lingualsurfacesof thealveolarplate LIPPING: Severe shelflike thickeningofthe alveolarmargin Pronouncedbulgeinthecontourofthefacial & lingualbone
ADAPTIVE REMODELING OF THE PERIODONTIUM Repair= Destruction:remodeled PDL Thickened &funnelshapedatthecrest Angulardefectsinthebone Nopockets Teethbecomeloose
HISTOMETRIC DIFFERENTIA TION Injuryphase: resorption formation Repairphase: resorption formation Adaptive remodeling: both return tonormal
EFFECT OF INSUFFICIENT OCCLUSAL FORCES Injurioustoperiodontium Thinningof thePDL Atrophyoffibers Osteoporosisof the alveolarbone Reductionin boneheight
Canresultfrom: Open-biterelationship Absenceof functionalantagonists Unilateralchewinghabits
FREMITUS TEST Measurement of the vibratory patterns of the teeth when the teeth are placedincontacting positions&movements Finger buccal& labialsurfaces-maxillary teeth T apthe teeth togetherin themaximum intercuspalposition Grind symmetrically in lateral, protrusive & lateral-protrusive contacting movements
CLASS I: Mild vibrationdetected CLASS II: Easilypalpablevibrationbut novisible movement CLASS III: Movementvisiblewith thenakedeye
RADIOGRAPHIC ASSESSMENT Degreeof bonelossfrom the CEJ to the apex. Width of the PDLspacearoundeachtooth Examinefor angularbonydefects Butthesefindingsnot necessarilywith TFO
PATHOLOGIC TOOTH MIGRATION DEFINITION Tooth displacement that results when the balance among the factors that maintain physiologictoothpositionisdisturbedby periodontaldisease
Common& earlysign Anteriorsfrequent Anydirection Mobility &Rotation Extrusion:Pathologicmigrationin theincisal/ occlusalaspect
WEAKENED PERIODONTAL SUPPORT Unableto maintainnormalposition Movesawayfrom opposingforceunless restrainedbyproximalcontact Forcesacceptedbynormalperiodontium becomeinjurious
CHANGES IN FORCES EXERTED ON THE TEETH A. Unreplaced missingteeth Driftinginto edentulousspaces Not dueto periodontaldestruction Conducivefor periodontaldiseases
B.FailuretoreplaceFirstMolars Second& third molarstiltreducingthe vertical dimension Premolars-distally& mandibularincisors-drift lingually Anterior overbite increased & mandibular incisors traumatize the gingiva Maxillary incisors pushed labially & laterally Anterior teeth extrude because incisal apposition has largely disappeared Diastema created- anterior teeth
OTHER CAUSES Pressure from the tongue Pressure from granulation tissue of periodontal pocket