Understanding Anorectal Malformations in Pediatric Surgery

Anorectal malformations are congenital abnormalities involving the development of the anal canal and sphincter muscles. They may present with imperforate anus, fistulous connections, or rectal atresia. Classification in males and females helps in determining the types of surgical treatments required. These anomalies have an incidence of 1 in 5000 live births, with varying functional outcomes depending on the type and associated anomalies. Early recognition, proper diagnosis, and staged surgical approaches are essential for managing these conditions successfully.
- Pediatric surgery
- Anorectal malformations
- Congenital abnormalities
- Surgical treatment
- Pediatric anomalies

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
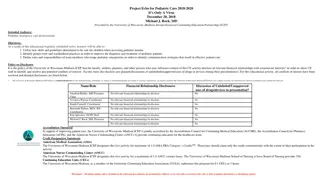
PEDIATRIC SURGERY-2018 No. :6 Attendance: Obligatory Type of lecture: theory Place : Hall no.4 college of medicine Mustansiriyah University . Date : Wednesday 5th of March 2018. Time : 12:00 1:00 AM. Students: 4th year / college of medicine / Mustansiriyah University By : Dr. Ali E. Joda M.B.Ch.B. - F.I.C.M.S. - pediatric surgeon. E. mail : ali.egab.joda@uomustansiriyah.edu.iq
Objectives:- What is Hirschsprung's disease, its pathophysiology, clinical features & way of diagnosis? What are the congenital anorectal malformations, the spectrum of the disease, classification of the types & the options of surgical treatment? By the end of this lecture, you have to be able to: 1. Summarize the main outlines of resuscitation in cases of acute presentation of these conditions. 2. Verifying the staged surgical approach of these conditions.
Anorectal malformation The baby born with congenital absence of anal orifice (imperforate anus), agenesis of anal canal with variable development of sphincteric muscle & it is often associated with fistulous connection to the urinary tract in male or genital tract in female with high possibility of associated anomalies.
Classification :- Male :- 1. Imperforate anus with cutaneous perineal fistula. 2. Imperforate anus with Recto-urethral fistula (most common). 3. Imperforate anus with recto-vesical fistula (bladder neck). 4. Imperforate anus without fistula. 5. Rectal atresia. Female :- 1. Imperforate anus with cutaneous perineal fistula. 2. Imperforate anus with recto-vestibular vestibular fistula (most common). 3. Imperforate anus without fistula. 4. Rectal atresia. Cloaca (common orifice for urethra, vagina, & rectum).
Incidence 1 in 5000 live birth, no specific cause, some genetic predisposition. These anomalies classified into high & low types based on the position of the terminal bowel in relation to the levator ani or pelvic floor in order to decide the type of management and to predict the final outcome. Low types are easily treated with an excellent functional prognosis. High types are difficult to manage & often associated with other anomalies, and have a poor functional prognosis.
Associated anomalies :- Most babies with anorectal malformations have one or more other associated abnormalities that affect other systems. Some of them are simple, incidental findings but others, such as cardiovascular defects, may be life threatening. VACTERL association: V Vertebral anomalies A Anal atresia C Cardiovascular anomalies T Tracheoesophageal fistula E Esophageal atresia R Renal (kidney) and/or radial anomalies L Limb defects
Diagnosis & management :- The diagnosis of absent anal orifice is usually obvious by inspection of perineum & external genitalia but such anomaly may be missed & not discovered until abdominal distension begins or the baby not passing meconium. The initial assessment of neonate with imperforate anus is to answer the followings :- Q / at which level the rectum is ended in relation to sphincter muscle? Q / where is the fistula ? Q/ can the anomaly be corrected by single perineal surgery or need initial colostomy then definitive surgery later on? Q / is there any associated anomalies needs immediate or subsequent correction?
Investigations :- (Invertogram) or (prone cross table lateral film): after 24 hr from birth , the baby is held upside down(invertogram) or placed in prone genu-pectroral position for 3 min., then lateral view X-ray is taken centered on greater trochanter & P-C line (pubis-coccyx) with marker applied at the natal cleft on the site of anal dimple. If the gas shadow in rectum is proximal to P-C line = high type imperforate anus & need initial colostomy while if the gas shadow in rectum is distal to P-C line = low type imperforate anus & no need for colostomy, just perineal anoplasty. Or we measure the bowel skin distance, if more than 2 cm = high type need colostomy, if less than 2 cm = low type , no colostomy is needed just perineal anoplasty.
1) Examination of urine in male: passage of meconium per urethra (meconuria) or air per urethra (pneumatuira) indicate high type impeforate anus with recto-urethral fistula or recto-vesical fistula that need initial colostomy. 2)Plane X-ray showing presence of gas in viscera other than GIT like bladder (recto-vesical fistula) ,or huge colonic gas shadow occupying half the width of abdomen in Congenital Pouch Colon syndrome. 3)Dye study of the fistula: to distinguish between recto-vestibular & ano-vestibular fistula. 4)Ultrasound: perineal ultrasound for measuring the distance between skin & rectal pouch as alternative to invertogram. 5)C.T Scan.
NO decision should be made about doing colostomy or primary anorectoplasty before age of 24 hr. because there should be significant intraluminal pressure for meconium to be forced through fistula orifice.( passing meconium through fistula orifice in perineum indicate low type , while passing meconium with the urine indicate high type). Radiological evaluation should not be done before age of 24 hr. because the rectum is still collapsed & it requires significant intraluminal pressure to overcome the muscle tone surrounding distal rectum. So during the 1st 24 hr. after birth the baby should receive I.V.F , antibiotics , investigated for associated anomalies by Cardiac Echo , continuity of esophagus , renal ultrasound , spinal ultrasound , X-ray of the lumbar spine & sacrum.
Colostomy :- Divided descended colostomy is ideal for anorectal malformation :- o For complete diversion of stool. o Permit doing distal colostogram to give us the detailed anatomy of the defect before anorectoplasty. o Better protection of the anorectoplasty repair. Loop colostomy is not preferable :- o Because it permit passage of stool from proximal stoma into distal bowel then through fistula into urinary tract leading to UTI. o It causes collection of stool in distal rectal pouch , fecal impaction , dilatation of rectum , irreversible hypomotility. o Colostomy prolapse is more common in loop type.
Transvers or right sided colostomy is not preferable :- o Because there will be long segment of defunctional distal colon, atrophied colon & colostomy diarrhea. o The mechanical cleaning of distal colon before definitive repair is much more difficult. o If there is large fistula with the urethra, there will be significant absorption of the urine in the colon before it escape through distal stoma leading to metabolic acidosis. Mid or lower sigmoidostomy is not preferable :- Because it will interfere with the mobilization of rectum during definitive repair of high type imperforate anus.
Operative repair of ano-rectal malformations:- Simple anal cut-back. V-Y anoplasty. Anal transposition. Limited Posterior Ano-Rrectoplasty PARP. Anterior Sagittal Ano-Rrectoplasty ASARP. Posterior Sagittal Ano-Rectoplasty PSARP. (((((((((((((((((((((((((((((((((((((((((((((End)))))))))))))))))))))))))))))))))))))))))))))))))) References: Baily & love's short practice of surgery 26th edition (2013). Ashcraft's pediatric surgery 6th edition (2014). Arnold G. Coran pediatric surgery 7th edition (2014). Newborn surgery 4th edition (2018). Quick guide to Pediatric surgery (2018).










 Examination of urine in male: passage of meconium per")