Managing Risk in Brain Injury: Strategies and Considerations

This informative content covers essential aspects of risk management in brain injury, including balancing client needs, promoting independence, and positive risk taking. It delves into the different parts of the brain, their functions, and the potential effects of brain injury on intellectual, behavioral, and neurological aspects. Understanding diagnostic issues, cognitive impairment, and areas of risk is crucial for effective care and support in brain injury cases.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Managing risk in brain injury HEADWAY 2017 BRUCE MOORE NEUROPSYCHIATRIST
Risk management : Its all a balancing act Whats best for the Client Promoting independence Enhancing quality of life Positive risk taking Risk assessment Applying frameworks What is YOUR goal ?
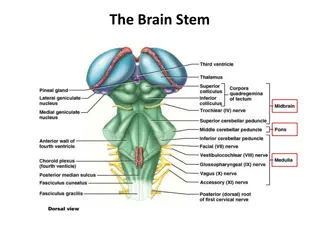
What do the different parts of the brain do? The brain is divided in two (connected by the corpus callosum) Left hemisphere Logic, language, planning, analysing Right hemisphere Social awareness, intuition, creativity In women the hemispheres are very well connected hence they can feel and think simultaneously (!) but men have feeble connections so they can either do listening OR logic but not both together Frontal lobes have 3 main areas: Dorsolateral (where horns might grow!) Mediofrontal (down the middle behind the eyes) Orbitofrontal (over the orbits/eye-sockets)
Function of Frontal lobe regions: Dorsolateral planning (ie what needs to be done) Damage leads to poor planning and prioritising) Mediofrontal initiates activity (connected to limbic/emotion circuits) Damage leads to avolition or worse (abulia = zombie-like absence of initiative) Orbitofrontal monitors activity and inhibits unwanted impulses Damage leads to socially disinhibited behaviour and aggression
Areas of risk DIAGNOSTIC ISSUES COGNITIVE IMPAIRMENT & DYSEXECUTIVE SYNDROME CHAOTIC AIMLESS IMPOVERISHED LIFESTYLE PERSONALITY DISORDER DISINHIBITION & IMPULSIVITY INITIATIVE AND MOTIVATION AGGRESSIVE BEHAVIOUR DEPRESSION & SUICIDE CUMULATIVE RISK ORGANIC PSYCHOSIS, PROSOPAGNOSIA, MORBID JEALOUSY PATHOLOGICAL GAMBLING ABSCONDING, WANDERING, FALLS, SEIZURES, RISK OF HARM & VULNERABLE TO EXPLOITATION & SELF NEGLECT
The effects of brain injury: know exactly what you re treating Intellectual deficits impaired attention, memory, concentration, orientation, planning, problem solving, and executive function. Behavioural problems impulsivity disinhibition, aggression, lack of initiative and motivation, fatigue, irritability, anxiety, mood swings, depression psychosis, OCD Neurological problems headache, epilepsy, dysphasia, dysphagia, autonomic instability, hyperhidrosis, paresis, diabetes insipidus, orthostatic hypotension,
SECONDARY COMPLICATIONS PSYCHOTROPIUC MEDICATION SEIZURES, DIABETES, DEATH DRIVING HAZARDS AND DRUG DRIVING ALCOHOL & DRUG USE ANABOLIC STEROIDS AND LIQUORICE ALLSORTS (SHOE BOX!) FAMILY DYNAMICS MUM OR DAD OR THE GIRLFRIEND PARENTING SKILLS SOCIAL MEDIA (DID YOU KNOW SHE WAS ONLY 15?) MAY NEED TO RESTRICT USE UNDER MCA WHEELCHAIR WARS KNIVES, MACHETES AND BASEBALL BATS AND SO MUCH MORE
Neurological complications Headache Epilepsy Lamotrigine, Carbamazepine, Leviteracetam Hyperhidrosis Botox, propranolol, sympathectomy Paresis/paralysis Botox for spasticity Orthostatic hypotension Avoid hypotensives eg Beta-blockers Diabetes insipidus Medical emergency (&SIADH) Dysphagia SLT assessment and advice Autonomic instability Temperature regulation vasopressin / propranolol Cardiovascular instability medical emergency Gabapentin for pain (and agitation/anxiety)
MR ANGRY-ALL-THE-TIME SEVERE TRAUMATIC BRAIN INJURY RTA IN TEENS TENANT IN VERY SQUALID TERRACED HOUSE PROBLEMS WITH LANDLORD MADE THREATS DEFENDANT INSURERS VIDEO SURVEILLANCE BECAME INCREASINGLY PARANOID ESCALATING CANNABIS USE (MEDICATION RUBBISH ) SACKED ME THEN GOT THE PHONE CALL AFTER ASSAULT CASE SETTLED POSH HOUSE CANNABIS PARANOIA CCTV INSTALLED PARANOIA KITCHEN KNIVES LEFT OUT CRISIS TEAM & POLICE FAMILY SUPPORT INVOLVED
MISS TAKE-ADVANTAGE-OF-ME KICKED IN HEAD BY HER HORSE AT 20 SEVERE TRAUMATIC BRAIN INJURY EMOTIONALLY LABILE AND VERY SOFT FOR A SOB-STORY MEETS MEN (IN PUBS OR ON THE STREET) INVITES THEM HOME THINGS GO MISSING PURSE, HANDBAG SHE MAKES THREATS TO KILL THEM POLICE GET INVOLVED BUT THE CYCLE REPEATS ITSELF RECOMMEND RESIDENTIAL BRAIN INJURY SERVICES UNDER MCA
MR MELANCHOLY HYPOXIC BRAIN INJURY (HANGED SELF IN HOSPITAL) MUM DIED BY SUICIDE (GUILT BAD SON) & STEP-DAD BY SUICIDE 7 YEARS IN RESIDENTIAL SETTING & SECTIONED AGAIN TEXTING CASE MANAGER AT NIGHT RE SUICIDAL IDEATION OUT WITH SUPPORT WORKERS LOOKING OVER BRIDGES PSYCHOLOGICAL TREATMENT DIFFICULT DUE TO MEMORY IMPAIRMENT SEVERE DEPRESSION LIFETIME RISK OF SUICIDE 7-10% SEVERE BRAIN INJURY INCREASES RISK BY 4:1 CRS 30% PARENTAL SUICIDE INCREASES RISK BY 5:1 CRS 150% TWO PARENTS ?? NO STATISTICS
TOP TIPS FOR RISK MANAGEMENT DON T BE SHY BE EXPLICIT ABOUT RISKS YOUR SAFETY AND WELFARE IS OUR PRIORITY IF I M DOING MY JOB RIGHT YOU WONT LIKE ME AT TIMES SHARE RISKS AND CONCERNS WITH TEAM & LAWYERS ASSESS MENTAL CAPACITY HEALTH AND WELFARE, CARE & RESIDENCE INVOLVE RELEVANT AGENCIES POLICE FAMILY SUPPORT, SOCIAL SERVICES BE PREPARED TO DISCHARGE IF NO ENGAGEMENG OR SUPPORT
HEALTH AND WELL-BEING REGIME INCENTIVISE ENGAGEMENT Financial reward or special events Best done with agreement of Financial Deputy Ensure no family collusion Mental Capacity Act (MCA 2005) Need to be explicit about legal frameworks NOT a punishment but aimed at health and well-being Best interests MDT re mental capacity for health carte and residence
THANKYOU FOR LISTENING ! DR BRUCE MOORE HABITAT HEALTH Ltd & Abbey Court appointments.braininjury@gmail.com