Understanding Fibroadenoma - A Benign Breast Tumor

Fibroadenomas are common benign breast tumors, with unknown pathogenesis but linked to hormonal factors. They typically present as painless, movable masses and are often diagnosed through ultrasound or mammogram. Management involves monitoring or surgical excision based on size, growth rate, patient factors, and desire for removal.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
1 Benign Breast Tumors DR. MAHMOUD AL-BALAS CONSULTANT BREAST ONCOPLASTIC, RECONSTRUCTIVE AND AESTHETIC SURGERY ASSISTANT PROFESSOR OF SURGERY HASHEMITE UNIVERSITY
Introduction 2 Fibroadenoma Intraductal Papilloma Lipoma Hamartoma Granular Cell Tumor Radial Scar Gynecomastia
Fibroadenoma 3 Benign Tumor Incidence: 8-10% (1955) BUT recent studies estimate it as high as 25% in Asymptomatic Women. Any age; mainly 20-30 yrs. Old Composed of epithelial and stromal elements. Arise form TDLU Might arise from bcl-2 positive mesenchymal cells similar to solitary fibrous tumors.
Fibroadenoma 4 Pathogenesis Unknown Hormonal stimulation (increased estrogen sensitivity, OCP in young age) EBV in immunosuppressed women
Fibroadenoma 5 Clinical Presentation: Most are asymptomatic If symptomatic: Firm, movable mass. Painless BUT may be associated with discomfort when large or in pressure area (i.e. wire of female brassiere) Multiple, bilateral in 20% of cases Medical attention ? Pain Rapid growth Cosmetic effect Fear of malignancy
Fibroadenoma 6 Radiologic Findings: Ultrasound: Usually the first radiologic modality of diagnosis. Round, oval, or lobular well circumscribed hypoechoic mass. Mammogram: Female > 35 years old Personal or Family history of BC. Clinically suspicious lesion
Fibroadenoma 7 Pathologic Classification Size: < 5 cm > or equal 5 cm (Giant fibroadenoma or Juvenile giant fibroadenoma in young age) Microscopic architecture of ductal elements: Pericanalicular. Intracanalicular. Simple Vs. Complex (i.e. with hyperplasia, metaplasia or sclerosing adenosis) Rare types: Tubular (pure) adenoma prominent adenosis with very little stroma Lactational adenoma lactational changes in secretory glands in fibroadenoma of pregnant or breast feeding women.
Fibroadenoma 8 Management: Follow up if < 2.5 cm , low growth, no personal or family history of BC Excision High growth rate Fibroepithelial lesion Complex lesions (i.e. may have slightly higher risk for BC) Patient desire, pain, cosmetics Older women FH of BC Surgical excision vs. US-Guided vacuum-assisted biopsy device (i.e. ling term data for recurrence not yet available)
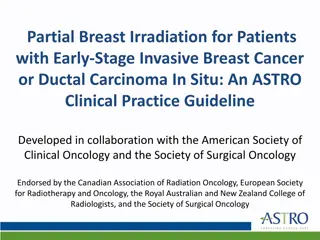
Management of Fibroadenoma in women younger than 35 years old 9 Breast Mass Physical Examination Ultrasound FNA / CNB Compatible with FA NO Yes Enlarged Regression FU Q6 months Until age 35 FU until complete regression Excise No change Age 35
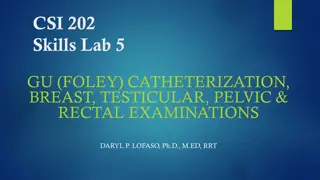
Management of Fibroadenoma in women older than 35 years old 10 Breast Mass Physical Examination Ultrasound Mammography FNA / CNB Compatible with FA NO Yes Complete regression Enlarged FU 6-12 months Routine follow up Excise Incomplete regression
Intraductal Papilloma 11 Benign rare neoplasms. Incidence 2-3% of population. Usually age 30-55 Develop within the mammary duct Typically small (few mm) and may grow to several centimeters.
12 Pathology Composed of breast epithelium supported by underlying stroma and a branching fibrovascular core. May be associated with ductal epithelial hyperplasia, ADH or DCIS. Atypical features associated with Intraductal papilloma carry higher risk of malignancy. Upgrading rate for CIS or IC was variable reported 0-29%
Intraductal Papilloma 13 Classification: Solitary or Multiple ( papillomatosis) Central (subareolar) or peripheral. Clinical presentation: Central: Spontaneous nipple discharge, serous, greenish or bloody (30%) Mass (rare) Peripheral: More frequently are asymptomatic Incidentally discovered on imaging studies. Higher association with malignancy (specially when multiple and Atypia is found)
Intraductal Papilloma 14 Imaging Imaging Modality Central Intraductal Papilloma Peripheral Intraductal Papilloma Mammography Frequently Occult Architectural distortion Nodular densities Mass +/- calcifications Calcifications alone Ultrasound Intraductal mass Complex cystic lesion with dilated duct Ductogram Completely obstructed duct Duct expansion and distortion Intraductal filling defects Wall irregularity
Intraductal Papilloma 15 Treatment: Surgical excision Low risk lesions for upgrading: No microcalcifications Absence of atypia Microscopic size lesions Sufficient amount of tissue on core biopsy.
Lipoma 16 Most common soft tissue tumor of the body (2.1/1000). Benign tumors of bland appearing adipose tissue. Reported in every area of the body. Breast Lipoma incidence is unknown (Lanng, 2004 ~ 4.6%) Reported in Males & Females.
Lipoma 17 Clinical Presentation: Painless, semi-firm, mobile mass, well circumscribed, variable in size. Giant lipoma if at lest 10 cm. Work-up: Triple Assessment
Lipoma 18 Radiologic findings: Mammogram: A mass with a density similar to normal surrounding breast. Very thin surrounding capsule. Benign appearing microcalcifications within the mass (i.e. may represent fat necrosis) Ultrasound: Isoechoic / hyperechoic mass Thin echogenic capsule No posterior acoustic shadow
Lipoma 19 Pathology: Gross smooth, fatty mass, encapsulated +/- lobulations Histologically mature adipocytes with capsule. Management: Observation Liposuction for small lipomas Surgical excision
Hamartoma 20 Definition: Rare breast tumors of breast tissue with stromal tissue and fat without structural organization. First described as mastoma (Prym, 1928) Females and Males. Incidence is unknown Reported among young as well as elderly. Clinical Presentation: Asymptomatic well circumscribed mobile soft non tender mass.
Hamartoma 21 Radiology Difficult to distinguish from other benign breast lesions. Mammogram ~ Breast-in-Breast pattern (similar density to surroundings) Architectural distortion Asymmetric mass with mixed densities and pseudocapsule Well circumscribe nodule Ultrasound Hypoechoic homogenous mass with distinct borders No acoustic shadow
Hamartoma 22 Pathology Gross Appearance: Hamartoma Classification Adenolipoma Characteristics Smooth, lobulated mass Disorganized being glandular, adipose and stromal tissue Pseudocapsule (compressed tissue at border) Benign hyaline cartilage with breast lobules and adipose tissue Smooth muscle component with breast component Variable amount of fat and fibrous tissue on cross sectioning. Associated pathological changes: Chondrolipo ma Myoid Hamartoma Apocrine metaplasia Usual papillary hyperplasia Stromal hyperplasia Cysts Adenosis
Hamartoma 23 Management FNA has little role in precise diagnosis Complete surgical excision is curative No need to obtain margins beyond hamartoma Recurrence is rare; due to incomplete excision Pure forms are not associated with increased risk of breast cancer
Granular Cell Tumor 24 Rare , Benign Occur in both Men and Women Age range 19-70 years (i.e. most frequent in 40 50 years) Neural origin (i.e. Schwann cells) First descried by Arbiskosov in 1926 as a Tongue mass tumor. Can arise in any organ in the body (i.e. Skin, Oral cavity, Digestive tract) 5-8% of GCTs occur in breast. Most commonly observed in African American women.
GCTs 25 Clinical Presentation: Any quadrant of the breast (i.e. mostly in medial aspect due to their perineural origin along the path of supraclavicular nerve) Can present as malignant mass Hard Non tender Mobile mass Rarely Skin changes, nipple retraction, breast edema
GCTs 26 Radiologic Findings variable presentation (benign or malignant features) Mammogram Smooth, rounded or lobulated Benign appearance Speculated malignant appearance US Hypoechoic (homo-/heterogenous) with posterior acoustic shadow Anechoic mass MRI also variable appearance (not specific for diagnosis)
GCTs 27 Pathology Gross appearance: Variable size (few centimeters up to 6 cm) Smooth surface Occasionally lobulated and hard Microscopic features (i.e. similar to Schwann cells) Non encapsulated Polygonal cells (in groups, sheets or nests) Eosinophilic cytoplasm Bland nuclei Positive cytoplasmic and nuclear staining for S-100
GCTs (Malignant variant) 28 Rare ; 1-2% of all GCTs Suggestive criteria Size > 5cm Areas of necrosis within the tumor High mitotic activity Nuclear pleomorphism
GCTs 29 Management Needle Biopsy establish the diagnosis Local excision is recommended to exclude coexisting malignant pathology No increase risk for BC in future Recurrence is very low even in close or positive margins No role for radiotherapy or for chemotherapy
Radial Scar 30 Benign breast lesion. Unknown origin Described by prof. Hamperl in 1975 Many other terms used to describe it (e.g. rosette-like lesion, proliferative centers, borderline breast tumors, non-encapsulated sclerosing lesion, etc.) Lesion characteristics: Hyalinized sclerotic center containing abundant elastic and elastoid masses. Lesions radiate into periphery and enclosing lobuli. Lobuli reveal epithelial proliferation range from simple hyperplasia with epithelial villi to other forms of rare true papilloma
Radial Scar 31 Terms correspond to the pathological size: Lesion with size < 9 mm Radial Scar Lesion size > 9 mm Complex sclerosing adenosis True prevalence is unknown (Asymptomatic) Estimated incidence from postmortem studies range between 7- 28% Estimated detection rate with mammogram is 0.03-0.09%
Radial Scar 32 Clinical Presentation Frequently Asymptomatic; incidental mammographic finding Painless firm breast mass (large lesions) role out carcinoma (Triple assessment) Any site of the breast can be involved. No chest wall fixation or skin involvement is reported.
Radial Scar 33 Imaging Mammogram (Tabar and Dean criteria); classical features Architectural distortion with central lucency Radiating long and thin spicules that vary in appearance on different projections. Absence of microcalcifications No clinically palpable mass Not all present with above features; some may lack central lucency and other may have microcalcifications Mammographic resemblance to carcinoma necessitate the need for the biopsy
Radial Scar 34 US 1/3 of cases are not visible on US. Hypoechoic mass or parenchymal distortion No additional information that can differentiate from carcinoma. MRI Not all mammographic detected scars are visible on MRI. Promising tool to differentiate from carcinoma. High negative predictive value for high risk lesions including radial scars specifically.
Radial Scar 35 Gross Pathology Gross similar to carcinoma Firm lesion pale core irregular edges yellow streaks infiltrate adjacent normal breast tissue. Microcysts surrounding radial scars can be seen (not typical for carcinoma) Histology Fibroelastotic core with entrapped ducts and radiating ducts and lobules at varying degree of proliferation. Calcification can be seen. Associated lesion can be seen also (atypical lesions, LN, in-situ or invasive carcinoma)
Radial Scar 36 DDX Postoperative changes Fat necrosis Carcinoma; specially Tubular carcinoma (the need for immunohistochemical differentiation) Note the risk of develop subsequent carcinoma in patient with previously diagnosed radial scar is controversial (from no risk to increased risk theories)
Radial Scars 37 Management Surgical Excision Due to possible presence of associated lesions or upstage to in-situ or invasive carcinoma Upstage rate 0-32% Observation (a trend by some professionals) Completely excised microscopic scars No atypia No enhancing MRI lesions
Gynecomastia 38 Being male breast enlargement Unilateral or bilateral Painless or tender (secondary to glandular proliferation and fat deposition) Psychological impact. 3 distinct peaks High prevalence Neonatal; observed in 75% Adolescence; 4-69% Old age; 55%
Gynecomastia 39 Etiology / Pathophysiology Imbalance of estrogen and androgen levels in male breast tissue Male breast tissue has: Estrogen receptors mediate glandular proliferation Androgen receptors inhibit glandular proliferation
Gynecomastia 40 Pathophysiology Increased Estrogen Level / Effect Decreased Androgen Level / Effect Increased production (adrenals, testes) Decreased production by testes Increased peripheral aromatization Altered androgen metabolism Exposure to estrogen like substances Androgen receptor defects Medications (more release of estrogen than androgen from sex hormone binding globulin) Medications shift androgen from their receptors
Gynecomastia 41 Neonatal gynecomastia: Placental transfer of maternal estrogen into fetal circulation Transient process Resolve spontaneously Adolescent gynecomastia: Peak age 13 14 Peripheral aromatization of circulation androgen Transient process; resolves with 1-3 years 8% of cases continue into adulthood Reassurance and surveillance Impact: psychological (embarrassment) and fear of malignancy
Gynecomastia 42 Adult gynecomastia: Idiopathic Physiological Also called senile gynecomastia Due to decreased levels of circulating androgens either to decreased production or increased peripheral conversion to estrogen Medication related Chronic diseases (liver failure, renal failure, testicular tumors, adrenocortical tumors, pituitary adenoma, hypogonadism, hyperthyroidism, obesity, ectopic hormone release, etc.)
Gynecomastia 43 Clinical valuation and Workup Etiology Idiopathic Acute / persistent in puberty Medications % 25% 25% 10- 20% 8% 8% 1% 3% Clinical history and Physical exam Assessment of regional lymph nodes Distinguishing clinical feature is concentric enlargement Cirrhosis / Malnutrition Hypogonadism Renal diseases Testicular tumors Frequently bilateral Pseudogynecomastia Excess fat deposition without concomitant ductal proliferation Soft bilaterally enlarged breast
Gynecomastia 44 Mammogram in male BC Sensitivity Specificity 92% 90% Alarming features Laboratory Work up LFT KFT TSH Prolactin Beta-HCG LH Testosterone Unilateral Eccentric growth pattern Skin or nipple changes Nipple discharge lymphadenopathy Family history of breast cancer
Gynecomastia 45 Gynecomastia Stages Nodular Pattern Recent onset < 1 year Fan shaped subareolar density Appear as hypoechoic subareolar mass with fat tissue surrounding Reversible stage / no fibrosis established Dendritic Pattern In more chronic stage Flame (or cone) shaped density infiltrate deeper, surround fat Irreversible fibrosis Diffuse glandular pattern US / Mammogram similar to female breast In patient treated with high doses of estrogen
Gynecomastia 46 Pathology Florid phase (reversible) In 1st year of onset Proliferation of ductal epithelium and stromal elements Periductal inflammation and edema No fibrosis Start after 6 months Minimal ductal proliferation Hyalinized periductal tissue Non surgical treatment might be successful Only surgical treatment Fibrotic phase (irreversible)
Gynecomastia 47 Management Look for possible underlying cause. Surgery Mainstay of treatment in long standing cases Subcutaneous mastectomy Liposuction Prophylaxis strategy in high risk patients (e.g. prostate cancer) Radiotherapy Tamoxifen ?! Not yet FDA approved
48 The End



























")