Improving HER2 Targeting in NSCLC With Selective TKI
 undefined
undefined
I
m
p
r
o
v
i
n
g
H
E
R
2
T
a
r
g
e
t
i
n
g
i
n
N
S
C
L
C
W
i
t
h
S
e
l
e
c
t
i
v
e
T
K
I
Zosia Piotrowska, MD, MHS
Massachusetts General Hospital
Boston, Massachusetts, USA


•
Consulting/Honoraria:
–
Blueprint Medicines, Daiichi Sankyo, Merck, Bayer, AstraZeneca, Janssen, Takeda, Eli Lilly,
Boehringer Ingelheim
•
Research Support (To Institution):
–
Novartis, Takeda, Spectrum, AstraZeneca, Tesaro/GSK, Cullinan Oncology, Daiichi Sankyo,
AbbVie, Blueprint Medicines, Janssen
•
Travel Support:
–
Janssen, AstraZeneca
D
i
s
c
l
o
s
u
r
e
s
ESMO = European Society for Medical Oncology.

•
H
E
R
2
(
E
r
b
B
2
)
i
s
o
n
e
o
f
t
h
e
4
m
e
m
b
e
r
s
o
f
t
h
e
E
r
b
B
f
a
m
i
l
y
o
f
r
e
c
e
p
t
o
r
t
y
r
o
s
i
n
e
k
i
n
a
s
e
s
,
a
l
o
n
g
w
i
t
h
E
G
F
R
(
E
r
b
B
1
,
H
E
R
1
)
,
H
E
R
3
(
E
r
b
B
3
)
,
a
n
d
H
E
R
4
(
E
r
b
B
4
)
1
,
2
•
H
E
R
2
p
r
o
t
e
i
n
o
v
e
r
e
x
p
r
e
s
s
i
o
n
a
n
d
/
o
r
H
E
R
2
g
e
n
e
a
m
p
l
i
f
i
c
a
t
i
o
n
u
p
t
o
1
0
0
-
f
o
l
d
i
n
c
r
e
a
s
e
i
n
c
e
l
l
-
s
u
r
f
a
c
e
H
E
R
2
i
n
c
r
e
a
s
e
d
f
o
r
m
a
t
i
o
n
o
f
H
E
R
2
-
c
o
n
t
a
i
n
i
n
g
h
e
t
e
r
o
d
i
m
e
r
s
a
c
t
i
v
a
t
i
o
n
o
f
s
e
v
e
r
a
l
o
n
c
o
g
e
n
i
c
s
i
g
n
a
l
i
n
g
p
a
t
h
w
a
y
s
,
i
n
c
l
u
d
i
n
g
M
A
P
K
,
P
I
3
K
/
A
K
T
,
P
L
C
,
P
K
C
,
a
n
d
J
A
K
-
S
T
A
T
1
,
2
H
E
R
2
A
c
t
i
v
a
t
i
o
n
D
r
i
v
e
s
O
n
c
o
g
e
n
i
c
D
o
w
n
s
t
r
e
a
m
S
i
g
n
a
l
i
n
g
,
P
r
o
m
o
t
i
n
g
T
u
m
o
r
P
r
o
l
i
f
e
r
a
t
i
o
n
a
n
d
S
u
r
v
i
v
a
l

Adapted from Iqbal N, Iqbal N.
3
AKT = protein kinase B; EGFR = epidermal growth factor receptor; ErbB = erythroblastic leukemia viral oncogene;
ESMO = European Society for Medical Oncology
; HER = human epidermal growth factor receptor; JAK = Janus kinase;
MAPK = mitogen-activated protein kinase; MAPKK = mitogen-activated protein kinase leukaemia; NF
κ
B = nuclear factor kappa B; mTOR = mammalian target of rapamycin; PI3K = phosphatidylinositol 3-kinase; PKC = protein kinase C;
PLC = phospholipase-C; PTEN = phosphatase and tensin homolog; RAF = rapidly accelerated fibrosarcoma; Ras = Rat sarcoma virus; STAT = signal transducers and activators of transcription.
1. Vathiotis IA, et al.
Pharmaceuticals (Basel).
2021;14(12):1300; 2. Ni J, Zhang L.
Onco Targets Ther.
2021;14:4087–4098; 3.
Iqbal N, Iqbal N.
Mol Biol Int
. 2014;2014:852748.

H
E
R
2
M
u
t
a
t
i
o
n
s
A
l
s
o
F
e
a
t
u
r
e
a
t
V
a
r
y
i
n
g
F
r
e
q
u
e
n
c
i
e
s
A
c
r
o
s
s
T
u
m
o
r
T
y
p
e
s
ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor 2.
Subramanian J, et al.
Oncologist
. 2019;24(12):e1303
–
e1314.
H
E
R
2
M
u
t
a
t
i
o
n
s
i
n
N
S
C
L
C
•
HER2
mutations occur in 1%–4%
of NSCLC
1–3
–
Exon 20 insertions
(YVMA variant ≈85%)
–
Point mutations in the tyrosine
kinase, transmembrane, and
extracellular domain
•
HER2
mutations have little
overlap with gene amplification
or protein expression
A = alanine; D = aspartic acid; E = glutamic acid; ESMO = European Society for Medical Oncology; F = phenylalanine; G = glycine;
HER2
= human epidermal growth factor receptor 2; IHC = immunohistochemistry; L = leucine;
M = methionine; NSCLC = non
–
small cell lung cancer; P = proline; S = serine; TM = transmembrane domain; Y = tyrosine.
1. Jebbink M, et al.
Cancer Treat Rev.
2020;86:101996; 2. Yu X, et al.
Front Oncol.
2022;12:860313; 3. Arcila ME, et al.
Clin Cancer Res.
2012;18:4910
–
4918.
R
o
l
e
o
f
C
h
e
m
o
i
m
m
u
n
o
t
h
e
r
a
p
y
i
n
H
E
R
2
m
t
N
S
C
L
C
•
As of today, chemotherapy ±
immunotherapy remains the standard
1L therapy for
HER2
-mutant NSCLC
•
Chemoimmunotherapy combinations
are generally used
•
However,
HER2
-mutant NSCLC has
limited benefit from PD-1/PD-L1
inhibitors (IMMUNOTARGET)
B
e
s
t
R
e
s
p
o
n
s
e
t
o
P
D
-
1
/
P
D
-
L
1
I
n
h
i
b
i
t
o
r
s
b
y
D
r
i
v
e
r
M
u
t
a
t
i
o
n
(
I
M
M
U
N
O
T
A
R
G
E
T
R
e
g
i
s
t
r
y
)
1L = first-line; ALK = anaplastic lymphoma kinase; BRAF = v-raf murine sarcoma viral oncogene homolog B1; CR = complete response; EGFR = epidermal growth factor receptor;
ESMO = European Society for Medical Oncology;
HER2 = human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor receptor 2–mutant;
KRAS = Kirsten rat sarcoma viral oncogene homologue; MET = mesenchymal epithelial transition;
NSCLC = non–small
cell lung cancer;
PD = progressive disease;
PD-1 = programmed cell death protein 1; PD-L1 = programmed death-ligand 1
;
PR = partial response;
RET = rearranged during transfection; ROS1 = r
earrangement of c-ros oncogene 1;
SD = stable disease.
Mazieres J, et al.
Ann Oncol.
2019;30(8):1321
–
1328.
N
u
m
e
r
o
u
s
T
h
e
r
a
p
e
u
t
i
c
S
t
r
a
t
e
g
i
e
s
T
a
r
g
e
t
i
n
g
H
E
R
2
m
t
N
S
C
L
C
A
r
e
i
n
D
e
v
e
l
o
p
m
e
n
t
1
,
2
Adapted from Rolfo C, et al 2020
1
and Uy NF, et al 2022.
2
ADC = antibody-drug conjugate; EGFR = epidermal growth factor receptor;
ESMO = European Society for Medical Oncology;
HER
=
human epidermal growth factor receptor;
HER2
mt
= human epidermal growth factor receptor 2-mutant;
mAb = monoclonal antibody;
NSCLC = non–small cell lung cancer
; TKI = tyrosine kinase inhibitor; wt = wild type.
1. Rolfo C, Russo A.
Cancer Discov.
2020;10(5):643
–
645; 2. Uy NF, et al.
Cancers (Basel).
2022;14(17):4155; 3. Brazel D, et al.
BioDrugs.
2022;36(6):717
–
729.
H
E
R
2
A
D
C
s
:
A
d
o
-
t
r
a
s
t
u
z
u
m
a
b
E
m
t
a
n
s
i
n
e
(
T
-
D
M
1
)
Efficacy in
HER2
mt
lung
adenocarcinoma
•
ORR, 8/18 (44%)
•
mPFS, 5 mo
(95% CI, 3–9)
•
mDoR, 4 mo (range, 1−9
mo)
•
Responses observed in:
–
HER2
exon 20 insertions
–
TMD mutation
–
Furin-like domain mutations
ADC = antibody-drug conjugate; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor receptor 2-mutant; mDoR = median duration of response;
mPFS = median progression-free survival; ORR = objective response rate; PFS = progression-free survival; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors, version 1.1; TMD = transmembrane domain.
Li BT, et al.
J Clin Oncol.
2018;36(24):2532–2537.
B
e
s
t
R
e
s
p
o
n
s
e
P
F
S
T
-
D
X
d
I
s
a
H
E
R
2
-
t
a
r
g
e
t
i
n
g
m
A
b
L
i
n
k
e
d
t
o
a
C
h
e
m
o
t
h
e
r
a
p
y
“
P
a
y
l
o
a
d
”
1
−
3
Adapted from Nakada T, et al. 2019.
3
ESMO = European Society for Medical Oncology;
HER2 = human epidermal growth factor receptor 2; IgG1 = immunoglobulin G1; mAb = monoclonal antibody; T-DXd = trastuzumab deruxtecan.
1. Li BT, et al. ASCO 2022. Poster TPS9137; 2. Azar I, et al.
Lung Cancer (Auckl).
2021;12:103–114; 3. Nakada T, et al.
Chem Pharm Bull (Tokyo)
. 2019;67(3):173–185.
D
e
r
u
x
t
e
c
a
n
C
l
e
a
v
a
b
l
e
t
e
t
r
a
p
e
p
t
i
d
e
-
b
a
s
e
d
l
i
n
k
e
r
T
o
p
o
i
s
o
m
e
r
a
s
e
I
i
n
h
i
b
i
t
o
r
p
a
y
l
o
a
d
H
u
m
a
n
i
z
e
d
a
n
t
i
-
H
E
R
2
I
g
G
1
m
A
b
T-DXd payload: deruxtecan, a topoisomerase I inhibitor
T
-
D
X
d
H
E
R
2
L
y
s
o
s
o
m
e
C
a
t
h
e
p
s
i
n
s
T
-
D
X
d
I
s
a
H
E
R
2
-
T
a
r
g
e
t
i
n
g
m
A
b
L
i
n
k
e
d
t
o
a
C
h
e
m
o
t
h
e
r
a
p
y
“
P
a
y
l
o
a
d
”
1
–
3
P
a
y
l
o
a
d
L
i
n
k
e
r
H
u
m
a
n
i
z
e
d
a
n
t
i
-
H
E
R
2
I
g
G
1
m
A
b
Adapted from Lambert JM, Berkenblit A. 2018
3
and Nakada T, et al. 2019.
4
DNA = deoxyribonucleic acid; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; IgG1 = immunoglobulin G1; mAb = monoclonal antibody; T-DXd = trastuzumab deruxtecan.
1. Li BT, et al. ASCO 2022. Poster TPS9137; 2. Azar I, et al.
Lung Cancer (Auckl).
2021;12:103–114; 3. Lambert JM, Berkenblit A.
Annu Rev Med.
2018;69:191–207; 4. Nakada T, et al.
Chem Pharm Bull (Tokyo)
. 2019;67(3):173–185.
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
:
A
P
h
a
s
e
2
T
r
i
a
l
o
f
T
-
D
X
d
i
n
M
e
t
a
s
t
a
t
i
c
H
E
R
2
m
t
N
S
C
L
C
R
e
f
r
a
c
t
o
r
y
t
o
S
t
a
n
d
a
r
d
T
r
e
a
t
m
e
n
t
BICR = blinded independent central review; DCR = disease control rate; DoR = duration of response; ECOG PS = Eastern Cooperative Oncology Group performance status;
ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor receptor 2–mutant;
NSCLC = non–small cell lung cancer
; ORR = objective response rate; OS = overall survival;
PD-1 = programmed cell
death protein 1; PD-L1 = programmed death-ligand 1
; PFS = progression-free survival; Q3W = every 3 weeks; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors version 1.1; T-DXd = trastuzumab deruxtecan.
Jänne P, et al. WCLC 2023. Mini oral presentation MA13.10.
•
Metastatic
HER2
mutation
advanced NSCLC (ECOG
PS 0–1)
•
≥1 prior therapy
(platinum-based
chemotherapy)
•
Measurable disease per
RECIST v1.1
K
e
y
E
l
i
g
i
b
i
l
i
t
y
C
r
i
t
e
r
i
a
•
Prior anti–PD-1/PD-L1
treatment
S
t
r
a
t
i
f
i
c
a
t
i
o
n
F
a
c
t
o
r
P
r
i
m
a
r
y
E
n
d
p
o
i
n
t
•
ORR by BICR
S
e
c
o
n
d
a
r
y
E
n
d
p
o
i
n
t
s
•
Confirmed ORR by
investigator
•
DoR
•
DCR
•
PFS
•
OS
•
Safety
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
P
r
i
m
a
r
y
R
e
s
u
l
t
s
:
A
n
t
i
t
u
m
o
r
A
c
t
i
v
i
t
y
o
f
T
-
D
X
d
5
.
4
m
g
/
k
g
Q
3
W
i
n
H
E
R
2
m
t
M
e
t
a
s
t
a
t
i
c
N
S
C
L
C
B
e
s
t
P
e
r
c
e
n
t
a
g
e
C
h
a
n
g
e
F
r
o
m
B
a
s
e
l
i
n
e
a
Patients who had zero best percentage change from baseline in the sum of diameters for all target lesions.
CR = complete response; DoR = duration of response;
ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor receptor 2–mutant;
mo = months;
NE = not estimable;
NSCLC = non–small cell lung cancer;
ORR = objective response rate;
PD-(L)1 = programmed cell death-(ligand)1;
PR = partial response; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan; TKI = tyrosine kinase inhibitor.
Goto K, et al.
J Clin Oncol.
2023;JCO2301361.
a
a
a
a
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
P
r
i
m
a
r
y
R
e
s
u
l
t
s
:
A
n
t
i
t
u
m
o
r
A
c
t
i
v
i
t
y
o
f
T
-
D
X
d
6
.
4
m
g
/
k
g
Q
3
W
i
n
H
E
R
2
m
t
M
e
t
a
s
t
a
t
i
c
N
S
C
L
C
B
e
s
t
P
e
r
c
e
n
t
a
g
e
C
h
a
n
g
e
F
r
o
m
B
a
s
e
l
i
n
e
a
Patients who had zero best percentage change from baseline in the sum of diameters for all target lesions.
CR = complete response; DoR = duration of response;
ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor;
HER2
mt
= human epidermal growth factor receptor 2–mutant;
NE = not estimable;
NSCLC = non–small cell lung cancer;
ORR = objective response rate;
PD-(L)1 = programmed cell death-(ligand)1;
PR = partial response; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan; TKI = tyrosine kinase inhibitor.
Goto K, et al.
J Clin Oncol.
2023;JCO2301361.
a
a
Median OS of T-DXd 5.4 mg/kg Q3W
19.5 mo (95% CI, 13.6−NE)
T
-
D
X
d
K
a
p
l
a
n
M
e
i
e
r
C
u
r
v
e
s
f
o
r
O
S
Median OS of T-DXd 6.4 mg/kg Q3W
NE (95% CI, 12.1–NE)
ESMO = European Society for Medical Oncology;
NE = not estimable; OS = overall survival; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan.
Goto K, et al.
J Clin Oncol.
2023;JCO2301361.
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
P
r
i
m
a
r
y
R
e
s
u
l
t
s
:
O
S
H
E
R
2
A
D
C
s
:
T
-
D
X
d
a
Data cutoff: June 22, 2022.
b
Median DoR based on Kaplan-Meier estimate.
ADC = antibody-drug conjugate; CI = confidence interval; DoR = duration of response;
ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor 2; mOS = median overall survival;
mPFS = median progression-free survival; NE = not estimable; NSCLC = non–small cell lung cancer; OR = objective response; PD-(L)1 = programmed death-ligand; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan;
TKI = tyrosine kinase inhibitor.
1. Li BT, et al.
N Engl J Med
. 2022;386(3):241
–
251; 2.
Goto K, et al.
J Clin Oncol.
2023;JCO2301361.
HER2
-mutated NSCLC
•
OR, 55% (95% CI, 44%
–
65%)
•
mPFS, 8.2 mo (95% CI, 6.0
–
11.9 mo)
•
mOS, 17.8 mo (95% CI, 13.8
–
22.1 mo)
HER2
-mutated nonsquamous NSCLC with disease progression after 1 prior systemic therapy
D
E
S
T
I
N
Y
-
L
u
n
g
0
1
1
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
2
5
.
4
m
g
/
k
g
Q
3
W
•
OR, 49% (95% CI, 39.0%
–59.1
%)
•
mPFS, 9.9 mo (95% CI, 7.4
–
NE)
•
mOS,19.5 mo (95% CI, 13.6
–
NE)
6
.
4
m
g
/
k
g
Q
3
W
•
OR, 56% (95% CI, 41.3%
–70.0
%)
•
mPFS,15.4 mo (95% CI, 8.3
–
NE)
•
mOS, NE (95% CI, 12.1
–
NE)
D
E
S
T
I
N
Y
-
L
u
n
g
0
1
D
r
u
g
-
R
e
l
a
t
e
d
A
E
s
•
Adjudicated drug-related
ILD occurred in 24/91
patients (26%) at 6.4 mg/kg
a
One patient had grade 5 (ie, fatal) pneumonitis that was assessed as drug-related by the investigator (subsequently adjudicated as ILD). Another patient had grade 3 ILD, as reported by the investigator, and died; the reported ILD was
subsequently adjudicated as grade 5 by the ILD adjudication committee.
b
This category includes the preferred terms fatigue, asthenia, and malaise.
c
This category includes the preferred terms neutrophil count decreased and
neutropenia.
d
This category includes the preferred terms hemoglobin decreased, red cell count decreased, anemia, and hematocrit decreased.
e
This category includes the preferred terms white cell count decreased and leukopenia.
AE = adverse event; ESMO = European Society for Medical Oncology;
ILD = interstitial lung disease.
Li BT, et al.
N Engl J Med.
2022;386(3):241
–
251.
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
P
r
i
m
a
r
y
R
e
s
u
l
t
s
:
O
v
e
r
a
l
l
S
a
f
e
t
y
a
Includes all randomly assigned patients who received ≥1 dose of T-DXd.
ILD = interstitial lung disease;
T-DXd = trastuzumab deruxtecan; TEAE = treatment-emergent adverse event.
Jänne P, et al. WCLC 2023. Mini oral presentation MA13.10.
A
d
j
u
d
i
c
a
t
e
d
D
r
u
g
-
R
e
l
a
t
e
d
I
L
D
•
Median treatment duration was 7.7 months (range, 0.7−20.8) with T-DXd 5.4 mg/kg and 8.3 months
(range, 0.7−20.3) with T-DXd 6.4 mg/kg
•
The most common any-grade TEAEs in the T-DXd 5.4 mg/kg and 6.4 mg/kg arms included nausea
(67.3% and 82.0%), neutropenia (42.6% and 56.0%), and fatigue (44.6% and 50.0%)
•
The most common grade ≥3 TEAEs in the T-DXd 5.4 mg/kg and 6.4 mg/kg arms included neutropenia
(18.8% and 36.0%) and anemia (10.9% and 16.0%)
B
a
s
e
d
o
n
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
R
e
s
u
l
t
s
,
T
-
D
X
d
R
e
c
e
i
v
e
d
F
D
A
A
c
c
e
l
e
r
a
t
e
d
A
p
p
r
o
v
a
l
i
n
A
u
g
u
s
t
2
0
2
2
1
1L = first-line; ESMO = European Society for Medical Oncology;
FDA = US Food and Drug Administration; HER2 = human epidermal growth factor receptor 2; IV = intravenously;
NSCLC = non–small cell lung cancer
;
Q3W = every 3 weeks; SPC = summary of product characteristics; T-DXd = trastuzumab deruxtecan.
1. Enhertu Approved.
AstraZeneca
:2022.
https://www.astrazeneca.com/media-centre/press-releases/2022/enhertu-approved-in-us-for-her2-mutant-nsclc.html
. Accessed September 2023; 2. Enhertu Prescribing Information. November
2022; 3. ClinicalTrials.gov. https://www.clinicaltrials.gov/study/NCT05048797. Accessed September 2023.
•
A
p
p
r
o
v
e
d
f
o
r
a
d
u
l
t
p
a
t
i
e
n
t
s
w
i
t
h
u
n
r
e
s
e
c
t
a
b
l
e
o
r
m
e
t
a
s
t
a
t
i
c
N
S
C
L
C
w
i
t
h
H
E
R
2
m
u
t
a
t
i
o
n
s
w
h
o
h
a
v
e
r
e
c
e
i
v
e
d
p
r
i
o
r
s
y
s
t
e
m
i
c
t
h
e
r
a
p
y
2
•
This indication is approved under accelerated approval
based on improvements observed in the
DESTINY-Lung02 trial
1
•
T
h
e
a
p
p
r
o
v
e
d
r
e
c
o
m
m
e
n
d
e
d
d
o
s
e
i
s
5
.
4
m
g
/
k
g
g
i
v
e
n
I
V
Q
3
W
,
b
a
s
e
d
o
n
r
e
s
u
l
t
s
o
f
D
E
S
T
I
N
Y
-
L
u
n
g
0
2
1
,
2
T-DXd
SPC
T
-
D
X
d
i
s
c
u
r
r
e
n
t
l
y
b
e
i
n
g
e
v
a
l
u
a
t
e
d
a
s
1
L
t
h
e
r
a
p
y
i
n
H
E
R
2
-
m
u
t
a
t
e
d
N
S
C
L
C
i
n
D
E
S
T
I
N
Y
-
L
u
n
g
0
4
3
D
E
S
T
I
N
Y
-
L
u
n
g
0
4
:
A
P
h
a
s
e
3
T
r
i
a
l
o
f
T
-
D
X
d
a
s
1
L
T
r
e
a
t
m
e
n
t
i
n
M
e
t
a
s
t
a
t
i
c
H
E
R
2
m
t
N
S
C
L
C
a
HER2 mutations may be detected in tissue or ctDNA.
b
Crossover is not permitted.
c
Investigator’s choice of cisplatin or carboplatin.
1L = first-line;
ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor 2;
HER2
mt
=
human epidermal growth factor receptor 2–mutant
;
NSCLC = non–small cell lung cancer;
T-DXd = trastuzumab deruxtecan.
Li BT, et al. ASCO 2022. Poster TPS9137.
T
K
I
s
TKI = tyrosine kinase inhibitor.
O
l
d
e
r
E
G
F
R
/
H
E
R
2
T
K
I
s
i
n
H
E
R
2
m
t
N
S
C
L
C
a
3/23 patients.
b
At increasing doses of mobocertinib 5−40 mg/d, 80 mg/d total daily dose, 120 mg/d, and 160 mg/d in 70 patients with previously treated NSCLC and
EGFR
ex20ins mutations.
EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion; GI = gastrointestinal; HER2 = human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor
receptor 2–mutant;
ORR = objective response rate; mPFS = median progression-free survival; NSCLC = non–small cell lung cancer; TKI = tyrosine kinase inhibitor.
1. Dziadziuszko R, et al.
J Thorac Oncol.
2019;14:1086–1094; 2. Lai WV, et al.
Eur J
Cancer.
2019;109:28–35; 3.
Hyman DM, et al.
Nature
. 2018;554(7691):189−194
; 4. Kris MG, et al.
Ann Oncol.
2015;26:1421–1427; 5. Riely GJ, et al.
Cancer Discov
. 2021;11(7):1688−1699.
P
y
r
o
t
i
n
i
b
i
n
t
h
e
1
L
T
r
e
a
t
m
e
n
t
o
f
H
E
R
2
m
t
N
S
C
L
C
1L = first-line; AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; CF = criteria fulfilled; CU = compassionate use; ErbB
=
erythroblastic leukemia viral oncogene; ESMO = European Society for
Medical Oncology;
HER2
mt
= human epidermal growth factor receptor 2–mutant; HR = hazard ratio; NSCLC = non–small cell lung cancer; ORR = objective response rate; PFS = progression-free survival; RWS = real-world study;
TRAE = treatment-related adverse event.
Liu SM, et al.
Nat Med.
2023;29(8):2079
–
2086.
•
Pyrotinib is an oral, irreversible pan-ErbB family inhibitor
O
R
R
:
CF: 35.7%
CU: 16.7%
T
R
A
E
s
R
e
p
o
r
t
e
d
i
n
≥
1
0
%
o
f
P
a
t
i
e
n
t
s
T
u
m
o
r
R
e
s
p
o
n
s
e
P
F
S
CF
CU
Present
Absent
Brain metastases
P
o
z
i
o
t
i
n
i
b
f
o
r
H
E
R
2
m
t
N
S
C
L
C
:
T
h
e
Z
E
N
I
T
H
-
2
0
T
r
i
a
l
•
Poziotinib is an irreversible pan-ErbB family inhibitor
BID = twice daily; EGFR = epidermal growth factor receptor;
ErbB
=
erythroblastic leukemia viral oncogene;
ESMO = European Society for Medical Oncology;
HER2 = human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor receptor 2–mutant;
NSCLC = non–small cell lung cancer;
PFS = progression-free survival; QD = once daily; RECIST = Response Evaluation Criteria in Solid Tumors.
Remon J, et al.
Cancer Treat Rev.
2020;90:102105.
P
o
z
i
o
t
i
n
i
b
i
n
t
h
e
T
r
e
a
t
m
e
n
t
o
f
P
r
e
v
i
o
u
s
l
y
T
r
e
a
t
e
d
N
S
C
L
C
W
i
t
h
H
E
R
2
e
x
2
0
i
n
s
M
u
t
a
t
i
o
n
s
•
ZENITH20-2 trial, cohort 2 (n = 90), previously
treated patients; all patients treated at 16 mg QD
a
The as-treated population was the primary analysis population and included all patients who received ≥1 dose of study medication.
b
The evaluable population excluded patients from the as-treated population who did not have a target
lesion at baseline and/or did not have sufficient follow-up to evaluate tumor response.
c
CR/PR confirmation required ≥28 days after first observation of CR/PR.
d
CR/PR confirmation required ≥21 days after first observation of CR/PR.
BICR = blinded independent central reviews; CR = complete response; DCR = disease control rate; DoR = duration of response; ErbB = erythroblastic leukemia viral oncogene; ESMO = European Society for Medical Oncology;
ex20ins = exon 20 insertion;
HER2
= human epidermal growth factor 2; NSCLC = non–small cell lung cancer; NE = not estimable; ORR = objective response rate; PD = progressive disease; PFS = progression-free survival;
PR = partial response; QD = once daily; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors version 1.1; SD = stable disease.
Le X, et al.
J Clin Oncol.
2022;40(7):710
–
718.
C
l
i
n
i
c
a
l
R
e
s
p
o
n
s
e
(
R
E
C
I
S
T
v
1
.
1
b
y
B
I
C
R
)
B
e
s
t
%
C
h
a
n
g
e
F
r
o
m
B
a
s
e
l
i
n
e
B
e
s
t
C
h
a
n
g
e
F
r
o
m
B
a
s
e
l
i
n
e
i
n
S
u
m
o
f
D
i
a
m
e
t
e
r
(
%
)
P
o
z
i
o
t
i
n
i
b
i
n
t
h
e
1
L
T
r
e
a
t
m
e
n
t
o
f
N
S
C
L
C
W
i
t
h
H
E
R
2
e
x
2
0
i
n
s
M
u
t
a
t
i
o
n
s
•
ZENITH20 trial, cohort 4 (n = 80)
–
Treated at 16 mg QD and 8 mg BID
A
n
t
i
t
u
m
o
r
A
c
t
i
v
i
t
y
b
y
I
C
R
1L = first-line; BID = twice daily; CR = complete response; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion;
HER2
= human epidermal growth factor 2; ICR = independent central review; mDoR = median
duration of response; mPFS = median progression-free survival; NE = not estimable; NR = not reached; NSCLC = non–small cell lung cancer; ORR = objective response rate; PD = progressive disease; PFS = progression-free survival;
PR = partial response;
QD = once daily; SD = stable disease.
Cornelissen R, et al.
J Thorac Oncol.
2023;18(8):1031
–
1041.
B
e
s
t
%
C
h
a
n
g
e
F
r
o
m
B
a
s
e
l
i
n
e
B
e
s
t
C
h
a
n
g
e
F
r
o
m
B
a
s
e
l
i
n
e
i
n
S
u
m
o
f
D
i
a
m
e
t
e
r
(
%
)
P
F
S
a
Rash includes dermatitis acneiform, palmar-plantar erythrodysesthesia syndrome, rash, rash erythematous, rash generalized, rash maculopapular, and rash popular.
b
Stomatitis includes mucosal inflammation and stomatitis.
AE = adverse event; BID = twice daily; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion;
HER2
= human epidermal growth factor 2; NSCLC = non–small cell lung cancer; QD = once daily.
Cornelissen R, et al.
J Thorac Oncol.
2023;18(8):1031
–
1041.
P
o
z
i
o
t
i
n
i
b
:
S
a
f
e
t
y
P
r
o
f
i
l
e
i
n
P
a
t
i
e
n
t
s
W
i
t
h
T
r
e
a
t
m
e
n
t
-
N
a
ï
v
e
N
S
C
L
C
W
i
t
h
H
E
R
2
e
x
2
0
i
n
s
M
u
t
a
t
i
o
n
s
Z
o
n
g
e
r
t
i
n
i
b
(
B
I
1
8
1
0
6
3
)
–
S
e
l
e
c
t
i
v
e
H
E
R
2
T
K
I
AE = adverse event; EGFR = epidermal growth factor receptor;
ErbB = erythroblastic leukemia viral oncogene; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion; GI = gastrointestinal;
HER2 = human epidermal growth factor receptor 2; HER2
mt
= human epidermal growth factor receptor 2–mutant;
TKD
=
tyrosine kinase domain; TKI
=
tyrosine kinase inhibitor; w
t = wild type.
Heymach J, et al. ASCO 2023. Abstract 8545.
w
t
E
G
F
R
b
l
o
c
k
e
d
Z
o
n
g
e
r
t
i
n
i
b
w
t
E
G
F
R
H
E
R
2
m
t
w
t
H
E
R
2
w
t
E
G
F
R
s
p
a
r
i
n
g
M
o
r
e
A
E
s
e
x
p
e
c
t
e
d
F
e
w
e
r
A
E
s
e
x
p
e
c
t
e
d
H
E
R
2
T
K
D
m
u
t
a
t
i
o
n
s
,
i
n
c
l
u
d
i
n
g
e
x
2
0
i
n
s
w
t
H
E
R
2
H
E
R
2
m
t
w
t
E
G
F
R
H
E
R
2
T
K
D
m
u
t
a
t
i
o
n
s
,
i
n
c
l
u
d
i
n
g
e
x
2
0
i
n
s
L
i
m
i
t
e
d
a
c
t
i
v
i
t
y
a
g
a
i
n
s
t
e
x
2
0
i
n
s
P
r
e
v
i
o
u
s
E
r
b
B
T
K
I
s
A
c
t
i
v
e
a
g
a
i
n
s
t
e
x
2
0
i
n
s
S
k
i
n
G
I
B
e
a
m
i
o
n
L
U
N
G
-
1
a
Overexpression, amplification, somatic mutation, or gene rearrangement involving HER2 or
NRG1
.
b
Excluding patients treated with
ADC
s. Phase
1
a primary endpoint: MTD and DLTs (MTD evaluation period); Phase
1
b primary endpoint:
objective response, according to RECIST v1.1.
ADC = antibody-drug conjugate; BID = twice daily; DLTs = dose-limiting toxicities; ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor receptor 2–mutant;
MTD = maximum tolerated dose; NRG1 = neuregulin 1; NSCLC = non–small cell lung cancer; QD = once daily;
RECIST v1.1 = Response Evaluation Criteria in Solid Tumors, version 1.1;
TKD = tyrosine kinase domain
.
Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08.
Phase 1 study of zongertinib in patients with advanced/metastatic solid tumors with HER2 aberrations,
including
HER2
mt
NSCLC
B
e
a
m
i
o
n
L
U
N
G
-
1
:
P
a
t
i
e
n
t
C
h
a
r
a
c
t
e
r
i
s
t
i
c
s
a
4
patient (8.0%) had missing data.
b
2
patients (4.0%) had missing data.
c
1+, 2+, or 3+ on immunohistochemistry.
ECOG PS = Eastern Cooperative Oncology Group performance status; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2;
NRG1
= neuregulin 1; NSCLC = non–small cell lung cancer
.
Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08.
NSCLC
(65%)
Lung cancer,
unspecified
(8%)
Endometrial
(4%)
Colorectal
cancer
(6%)
N
=
5
0
a
Other tumors
(17%)
Data cutoff: July 17, 2023
.
a
Patients with ≥1 postbaseline tumor assessment or discontinued before first assessment for any reason.
b
Patients where mutation information was provided by the sites (which was optional in Phase
1
a).
CR = complete response; DCR = disease control rate; ESMO = European Society for Medical Oncology; insYVMA = YVMA insertion; NE = not estimable; NSCLC = non–small cell lung cancer; ORR = objective response rate;
PD = progressive disease; PR = partial response; SD = stable disease.
Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08.
Data cutoff: July 17, 2023
.
•
PR: 7/11 (63.6%)
•
SD: 3/11 (27.3%)
•
PD: 1/11 (9.1%)
A775_G776
insYVMA (n = 11
b
)
B
e
s
t
P
e
r
c
e
n
t
a
g
e
C
h
a
n
g
e
F
r
o
m
B
a
s
e
l
i
n
e
B
e
s
t
O
v
e
r
a
l
l
T
r
e
a
t
m
e
n
t
R
e
s
p
o
n
s
e
B
e
a
m
i
o
n
L
U
N
G
-
1
:
A
n
t
i
t
u
m
o
r
R
e
s
p
o
n
s
e
i
n
P
h
a
s
e
1
a
62%
Patients still on treatment
as of July 17, 2023
7
.
5
(
1
–
2
4
)
Median number
of cycles (range)
ESMO = European Society for Medical Oncology; PD = progressive disease; PR = partial response; SD = stable disease.
Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08.
Z
o
n
g
e
r
t
i
n
i
b
T
r
e
a
t
m
e
n
t
R
e
s
p
o
n
s
e
O
v
e
r
T
i
m
e
B
e
a
m
i
o
n
L
U
N
G
-
1
:
T
r
e
a
t
m
e
n
t
R
e
s
p
o
n
s
e
i
n
P
h
a
s
e
1
a
B
e
a
m
i
o
n
L
U
N
G
-
1
:
P
h
a
s
e
1
a
D
o
s
e
E
s
c
a
l
a
t
i
o
n
a
n
d
S
a
f
e
t
y
a
≥8% of total patients.
b
Combined term, includes rash, rash maculopapular, and dermatitis acneiform.
ALT = alanine aminotransferase; AST = aspartate aminotransferase; BID = twice
daily
; DLTs = dose-limiting toxicities;
ESMO = European Society for Medical Oncology;
QD = once
daily
; TRAEs = treatment-related adverse event.
Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08
.
Patients
with DLTs during the
on-treatment period
Patient with TRAE leading to
treatment discontinuation (
g
rade
3
ALT increased)
M
o
s
t
T
R
A
E
s
w
e
r
e
g
r
a
d
e
1
o
r
2
Patient with serious TRAEs (
g
rade
3 ALT and AST increased)
3
1
1
B
e
a
m
i
o
n
L
U
N
G
-
1
(
P
h
a
s
e
1
b
)
:
A
n
t
i
t
u
m
o
r
A
c
t
i
v
i
t
y
i
n
P
r
e
v
i
o
u
s
l
y
T
r
e
a
t
e
d
N
S
C
L
C
W
i
t
h
H
E
R
2
T
K
D
M
u
t
a
t
i
o
n
s
7
3
.
9
%
(
5
3
.
5
%
–
8
7
.
5
%
)
O
R
R
(
9
5
%
C
I
)
:
•
Median best percentage change
from baseline in target lesions:
−41.2%
O
v
e
r
a
l
l
(
N
=
2
3
)
b
•
DCR: 91.3%
•
P
atients included had between 2
and 5 cycles of treatment at cutoff
a
Patients who
started treatment ≥7 weeks prior to the snapshot date with baseline and postbaseline tumor assessments.
b
Patients who started treatment ≥7 weeks prior to the snapshot date.
CI = confidence interval; DCR = disease control rate; ESMO = European Society for Medical Oncology;
HER2
= human epidermal growth factor receptor 2; NSCLC = non–small cell lung cancer; ORR = objective response rate;
TKD = tyrosine kinase domain.
Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08
.
E
L
V
N
-
0
0
2
:
P
r
e
c
l
i
n
i
c
a
l
A
c
t
i
v
i
t
y
•
ELVN-002 is a potent, irreversible inhibitor of HER2 with a >100-fold selectivity over EGFR
1
•
ELVN-002 showed preclinical activity in xenograft models, including an intracranial model, driven by
wt
HER2
and
HER2
mt
and was well tolerated in all models tested.
1
It is now being evaluated in a
phase 1 study in
HER2
mt
solid tumors
2
T
u
m
o
r
g
r
o
w
t
h
i
n
h
i
b
i
t
i
o
n
i
n
B
e
a
s
2
b
H
E
R
2
Y
V
M
A
x
e
n
o
g
r
a
f
t
3
C
N
S
a
n
t
i
-
t
u
m
o
r
a
c
t
i
v
i
t
y
i
n
N
C
I
-
N
8
7
H
E
R
2
w
i
l
d
t
y
p
e
i
n
t
r
a
c
r
a
n
i
a
l
m
o
d
e
l
3
E
L
V
N
-
0
0
2
A
n
t
i
t
u
m
o
r
A
c
t
i
v
i
t
y
a
n
d
A
d
d
i
t
i
v
e
A
c
t
i
v
i
t
y
W
i
t
h
T
-
D
X
d
3
a
Kp,uu is the unbound brain to plasma partition coefficient, which is used to define the unbound drug concentration in the brain relative to blood with a reference. Kp,uu = Free brain concentration (total brain concentration adjusted for brain
tissue binding)/Free plasma concentration (total plasma concentration adjusted for protein binding).
BID = twice
daily
; CNS = central nervous system; EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor;
HER2
mt
= human epidermal growth factor receptor
2–mutant;
Q3W = every 3 weeks;
QD = once
DAILY
; T-DXd
= trastuzumab deruxtecan;
TGI = tumor growth inhibition;
wt
= wild type.
1. Aujay M, et al.
Cancer Res.
2023;83(7_suppl):4019; 2. ClinicalTrials.gov. https://www.clinicaltrials.gov/study/NCT05650879. Accessed September 2023; 3. Bowyer S, et al. WCLC 2023. Poster P2.09.
12 h
(4 h Tucatinib)
16 h
(8 h Tucatinib)
K
p
,
u
u
(
f
r
e
e
b
r
a
i
n
c
o
n
c
e
n
t
r
a
t
i
o
n
)
a
E
L
V
N
-
0
0
2
:
P
h
a
s
e
1
S
t
u
d
y
i
n
S
o
l
i
d
T
u
m
o
r
s
W
i
t
h
H
E
R
2
M
u
t
a
t
i
o
n
s
,
A
m
p
l
i
f
i
c
a
t
i
o
n
,
o
r
O
v
e
r
e
x
p
r
e
s
s
i
o
n
a
Successive cohorts will receive escalating doses of QD ELVN‑002. Dose escalation decisions will follow a Bayesian design. Dosing will be continuous in 21‑day cycles until disease progression or unacceptable toxicity. Dose escalation
may continue until the maximum tolerated dose is identified. 2 RDs for phase 1b monotherapy expansion will be chosen. Evaluation of BID regimen and intermediate dose levels may occur upon approval of the Safety Review Committee.
Dose exploration may consist of up to 30 patients who may be enrolled at ≥1 dose level to further evaluate the safety, tolerability, PK, and clinical activity. A maximum of 10 patients may be enrolled at any given dose level.
b
Single-patient
cohort.
BID = twice daily; DL = dose level; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2;
HER2
mt
= human epidermal growth factor receptor 2–mutant; NSCLC = non–small cell lung cancer;
PK = pharmacokinetics;
QD = once daily;
RD = recommended dose; T-DM1 = ado-trastuzumab emtansine; T-DXd = trastuzumab deruxtecan.
Bowyer S, et al. WCLC 2023. Poster P2.09.
ELVN‑002‑001 is a first‑in‑human, Phase 1, open‑label, multicenter, dose-escalation and -expansion
study to evaluate the safety, tolerability, PK, and preliminary antitumor activity of ELVN‑002
monotherapy and in combination with T‑DXd or T‑DM1 in patients with solid tumors with HER2
alterations, including
HER2
mt
NSCLC and HER2‑overexpressed metastatic breast cancer
P
h
a
s
e
1
b
:
M
o
n
o
t
h
e
r
a
p
y
D
o
s
e
E
x
p
a
n
s
i
o
n
P
h
a
s
e
1
a
:
E
L
V
N
-
0
0
2
M
o
n
o
t
h
e
r
a
p
y
D
o
s
e
E
s
c
a
l
a
t
i
o
n
a
b
DL1
R
D
S
u
m
m
a
r
y
a
n
d
C
o
n
c
l
u
s
i
o
n
s
•
HER2
mutations occur in ≈1%–4% of NSCLC
1–3
–
ex20ins are most common, but point mutations in the tyrosine kinase, transmembrane, and
extracellular domain are also observed
1–3
•
T-DXd has accelerated FDA approval for
HER2
mt
NSCLC after prior systemic therapy
4
•
The clinical development of EGFR/HER2 TKIs for
HER2
mt
NSCLC has been limited by significant
toxicities (largely EGFR-related)
5–9
•
Novel HER2-specific TKIs (zongertinib, ELVN-002) are now in clinical development
10–13
EGFR = epidermal growth factor receptor;
ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertions;
FDA = US Food and Drug Administration;
HER2
= human epidermal growth factor receptor 2;
HER2
mt
= human
epidermal growth factor receptor 2–mutant;
NSCLC = non–small cell lung cancer; T-DXd = trastuzumab deruxtecan; TKI = tyrosine kinase inhibitor.
1.
Jebbink M, et al.
Cancer Treat Rev.
2020;86:101996;
2.
Yu X, et al.
Front Oncol.
2022;12:860313;
3. Arcila ME, et al.
Clin Cancer Res
. 2012;18:4910–4918; 4.
Enhertu Approved.
AstraZeneca
:2022. Accessed September 2023;
5.
Dziadziuszko R, et al.
J Thorac Oncol.
2019;14:1086
–
1094; 6. Lai WV, et al.
Eur J
Cancer.
2019;109:28
–
35; 7. Hyman DM, et al.
Nature.
2018;554(7691):189−194; 8. Kris MG, et al.
Ann Oncol.
2015;26:1421
–
1427
;
9
. Son J, et al.
Cancer
Res.
2022;82(8):1633
–
1645; 10.
Heymach J, et al. ASCO 2023. Abstract 8545; 11. Seymour C.
OncLive
2023.
https://www.onclive.com/view/zongertinib-proves-clinically-active-with-low-rate-of-egfr-mediated-aes-in-her2-mutant-solid-tumors
.
Accessed September 2023; 12.
ClinicalTrials.gov. https://classic.clinicaltrials.gov/ct2/show/NCT05650879. Accessed September 2023; 13. Aujay M, et al. AACR 2023, Poster 4019.
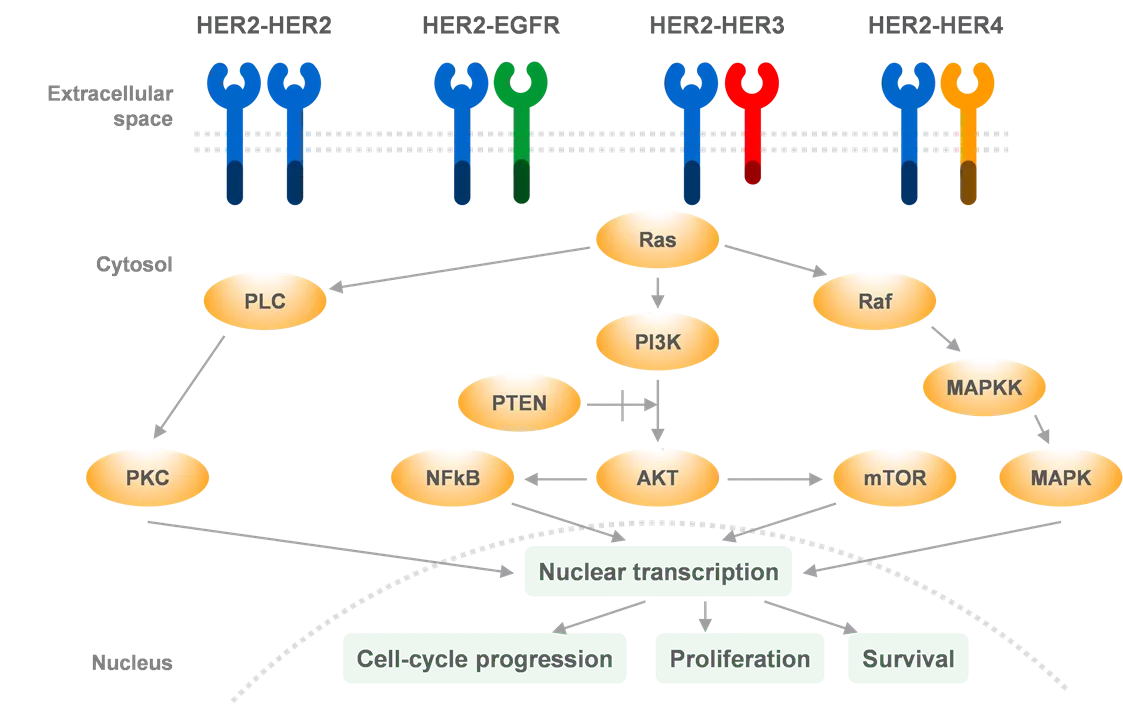
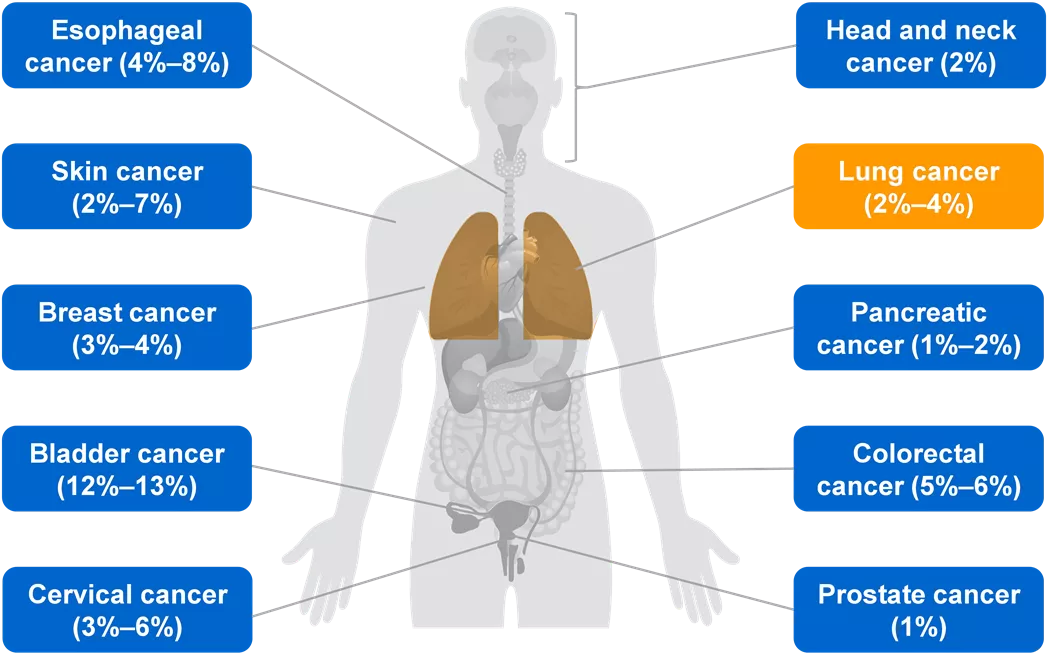
HER2 activation plays a crucial role in promoting tumor proliferation and survival in NSCLC. Driven by oncogenic downstream signaling pathways, HER2 overexpression and gene amplification lead to the formation of heterodimers and activation of key signaling cascades. Additionally, HER2 mutations are present at varying frequencies across different tumor types. These findings underscore the importance of targeting HER2 in NSCLC and highlight the potential of selective TKIs to improve treatment outcomes.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Improving HER2 Targeting in NSCLC With Selective TKI Zosia Piotrowska, MD, MHS Massachusetts General Hospital Boston, Massachusetts, USA
Disclosures Consulting/Honoraria: Blueprint Medicines, Daiichi Sankyo, Merck, Bayer, AstraZeneca, Janssen, Takeda, Eli Lilly, Boehringer Ingelheim Research Support (To Institution): Novartis, Takeda, Spectrum, AstraZeneca, Tesaro/GSK, Cullinan Oncology, Daiichi Sankyo, AbbVie, Blueprint Medicines, Janssen Travel Support: Janssen, AstraZeneca 2 ESMO = European Society for Medical Oncology. ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
HER2 Activation Drives Oncogenic Downstream Signaling, Promoting Tumor Proliferation and Survival HER2 (ErbB2) is one of the 4 members of the ErbB family of receptor tyrosine kinases, along with EGFR (ErbB1, HER1), HER3 (ErbB3), and HER4 (ErbB4)1,2 HER2-HER2 HER2-EGFR HER2-HER3 HER2-HER4 Extracellular space Ras Cytosol HER2 protein overexpression and/or HER2 gene amplification up to 100-fold increase in cell-surface HER2 increased formation of HER2- containing heterodimers activation of several oncogenic signaling pathways, including MAPK, PI3K/AKT, PLC, PKC, and JAK-STAT1,2 PLC Raf PI3K MAPKK PTEN PKC NFkB AKT mTOR MAPK Nuclear transcription Cell-cycle progression Proliferation Survival Nucleus Adapted from Iqbal N, Iqbal N.3 AKT = protein kinase B; EGFR = epidermal growth factor receptor; ErbB = erythroblastic leukemia viral oncogene; ESMO = European Society for Medical Oncology; HER = human epidermal growth factor receptor; JAK = Janus kinase; MAPK = mitogen-activated protein kinase; MAPKK = mitogen-activated protein kinase leukaemia; NF B = nuclear factor kappa B; mTOR = mammalian target of rapamycin; PI3K = phosphatidylinositol 3-kinase; PKC = protein kinase C; PLC = phospholipase-C; PTEN = phosphatase and tensin homolog; RAF = rapidly accelerated fibrosarcoma; Ras = Rat sarcoma virus; STAT = signal transducers and activators of transcription. 1. Vathiotis IA, et al. Pharmaceuticals (Basel). 2021;14(12):1300; 2. Ni J, Zhang L. Onco Targets Ther. 2021;14:4087 4098; 3. Iqbal N, Iqbal N. Mol Biol Int. 2014;2014:852748. 3 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
HER2 Mutations Also Feature at Varying Frequencies Across Tumor Types Esophageal cancer (4% 8%) Head and neck cancer (2%) Skin cancer (2% 7%) Lung cancer (2% 4%) Breast cancer (3% 4%) Pancreatic cancer (1% 2%) Bladder cancer (12% 13%) Colorectal cancer (5% 6%) Cervical cancer (3% 6%) Prostate cancer (1%) ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2. Subramanian J, et al. Oncologist. 2019;24(12):e1303 e1314. 4 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
HER2 Mutations in NSCLC HER2 mutations occur in 1% 4% of NSCLC1 3 Exon 20 insertions (YVMA variant 85%) Point mutations in the tyrosine kinase, transmembrane, and extracellular domain cohort A 2% 4% HER2 mutations have little overlap with gene amplification or protein expression HER2 mutation HER2 amplification cohort B 2% 4% HER2 IHC 2+ HER2 IHC 3z+ cohort C 2.5% 34% A = alanine; D = aspartic acid; E = glutamic acid; ESMO = European Society for Medical Oncology; F = phenylalanine; G = glycine; HER2 = human epidermal growth factor receptor 2; IHC = immunohistochemistry; L = leucine; M = methionine; NSCLC = non small cell lung cancer; P = proline; S = serine; TM = transmembrane domain; Y = tyrosine. 1. Jebbink M, et al. Cancer Treat Rev. 2020;86:101996; 2. Yu X, et al. Front Oncol. 2022;12:860313; 3. Arcila ME, et al. Clin Cancer Res. 2012;18:4910 4918. 5 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Role of Chemoimmunotherapy in HER2mt NSCLC As of today, chemotherapy immunotherapy remains the standard 1L therapy for HER2-mutant NSCLC Best Response to PD-1/PD-L1 Inhibitors by Driver Mutation (IMMUNOTARGET Registry) Chemoimmunotherapy combinations are generally used (n=37) BRAF (n=32) MET (n=246) KRAS However, HER2-mutant NSCLC has limited benefit from PD-1/PD-L1 inhibitors (IMMUNOTARGET) (n=27) HER2 (n=115) EGFR (n=19) ALK (n=16) RET (n=6) ROS1 1L = first-line; ALK = anaplastic lymphoma kinase; BRAF = v-raf murine sarcoma viral oncogene homolog B1; CR = complete response; EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; KRAS = Kirsten rat sarcoma viral oncogene homologue; MET = mesenchymal epithelial transition; NSCLC = non small cell lung cancer; PD = progressive disease; PD-1 = programmed cell death protein 1; PD-L1 = programmed death-ligand 1; PR = partial response; RET = rearranged during transfection; ROS1 = rearrangement of c-ros oncogene 1; SD = stable disease. Mazieres J, et al. Ann Oncol. 2019;30(8):1321 1328. 6 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Numerous Therapeutic Strategies Targeting HER2mt NSCLC Are in Development1,2 mAbs Bind to the extracellular domain of HER2 to block homodimerization and heterodimerization2 ADCs Utilize a mAb linked to a cytotoxic agent payload to direct the payload to cancer cells2 TKIs Non EGFRwt-sparing3 Block phosphorylation of the tyrosine kinase residues, inhibiting cell proliferation2 Novel HER2 TKls EGFRwt-sparing3 Pan-HER inhibitors Adapted from Rolfo C, et al 20201and Uy NF, et al 2022.2 ADC = antibody-drug conjugate; EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; HER = human epidermal growth factor receptor; HER2mt = human epidermal growth factor receptor 2-mutant; mAb = monoclonal antibody; NSCLC = non small cell lung cancer; TKI = tyrosine kinase inhibitor; wt = wild type. 1. Rolfo C, Russo A. Cancer Discov. 2020;10(5):643 645; 2. Uy NF, et al. Cancers (Basel). 2022;14(17):4155; 3. Brazel D, et al. BioDrugs. 2022;36(6):717 729. 7 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
HER2 ADCs: Ado-trastuzumab Emtansine (T-DM1) Efficacy in HER2mt lung adenocarcinoma Best Response PFS ORR, 8/18 (44%) mPFS, 5 mo (95% CI, 3 9) mDoR, 4 mo (range, 1 9 mo) Responses observed in: HER2 exon 20 insertions TMD mutation Furin-like domain mutations ADC = antibody-drug conjugate; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2-mutant; mDoR = median duration of response; mPFS = median progression-free survival; ORR = objective response rate; PFS = progression-free survival; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors, version 1.1; TMD = transmembrane domain. Li BT, et al. J Clin Oncol. 2018;36(24):2532 2537. 8 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
T-DXd Is a HER2-targeting mAb Linked to a Chemotherapy Payload 1 3 T-DXd payload: deruxtecan, a topoisomerase I inhibitor Humanized anti-HER2 IgG1 mAb Deruxtecan Cleavable tetrapeptide-based linker Topoisomerase I inhibitor payload Adapted from Nakada T, et al. 2019.3 ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; IgG1 = immunoglobulin G1; mAb = monoclonal antibody; T-DXd = trastuzumab deruxtecan. 1. Li BT, et al. ASCO 2022. Poster TPS9137; 2. Azar I, et al. Lung Cancer (Auckl). 2021;12:103 114; 3. Nakada T, et al. Chem Pharm Bull (Tokyo). 2019;67(3):173 185. 9 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
T-DXd Is a HER2-Targeting mAb Linked to a Chemotherapy Payload 1 3 T-DXd 1. T-DXd binds to HER2 Humanized anti-HER2 IgG1 mAb HER2 Linker 2. Endocytosis Payload Cathepsins Lysosome 6. Bystander killing effect 4. DNA replication disruption 3. Cleavage of linker and payload release 5. Induction of apoptosis Adapted from Lambert JM, Berkenblit A. 20183and Nakada T, et al. 2019.4 DNA = deoxyribonucleic acid; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; IgG1 = immunoglobulin G1; mAb = monoclonal antibody; T-DXd = trastuzumab deruxtecan. 1. Li BT, et al. ASCO 2022. Poster TPS9137; 2. Azar I, et al. Lung Cancer (Auckl). 2021;12:103 114; 3. Lambert JM, Berkenblit A. Annu Rev Med. 2018;69:191 207; 4. Nakada T, et al. Chem Pharm Bull (Tokyo). 2019;67(3):173 185. 10 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
DESTINY-Lung02: A Phase 2 Trial of T-DXd in Metastatic HER2mt NSCLC Refractory to Standard Treatment Key Eligibility Criteria Study Design Primary Endpoint Metastatic HER2 mutation advanced NSCLC (ECOG PS 0 1) Randomization ORR by BICR T-DXd 5.4 mg/kg Q3W n=102 1 prior therapy (platinum-based chemotherapy) Secondary Endpoints Ratio 2:1 Confirmed ORR by investigator Measurable disease per RECIST v1.1 T-DXd DoR 6.4 mg/kg Q3W n = 50 N=152 DCR PFS Stratification Factor OS Prior anti PD-1/PD-L1 treatment Safety BICR = blinded independent central review; DCR = disease control rate; DoR = duration of response; ECOG PS = Eastern Cooperative Oncology Group performance status; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; NSCLC = non small cell lung cancer; ORR = objective response rate; OS = overall survival; PD-1 = programmed cell death protein 1; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; Q3W = every 3 weeks; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors version 1.1; T-DXd = trastuzumab deruxtecan. J nne P, et al. WCLC 2023. Mini oral presentation MA13.10. 11 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
DESTINY-Lung02 Primary Results: Antitumor Activity of T- DXd 5.4 mg/kg Q3W in HER2mt Metastatic NSCLC Best Percentage Change From Baseline T-DXd 5.4 mg/kg Q3W (n = 102) DESTINY-Lung02 (n = 152) aa a a Confirmed ORR, n (%) (95% CI) 50 (49.0) (39.0 59.1) CR 1 (1.0) PR 49 (48.0) Median DoR, mo (95% CI) 16.8 (6.4 NE) Median follow-up, mo (range) 11.5 (1.1 20.6) aPatients who had zero best percentage change from baseline in the sum of diameters for all target lesions. CR = complete response; DoR = duration of response; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; mo = months; NE = not estimable; NSCLC = non small cell lung cancer; ORR = objective response rate; PD-(L)1 = programmed cell death-(ligand)1; PR = partial response; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan; TKI = tyrosine kinase inhibitor. Goto K, et al. J Clin Oncol. 2023;JCO2301361. 12 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
DESTINY-Lung02 Primary Results: Antitumor Activity of T-DXd 6.4 mg/kg Q3W in HER2mt Metastatic NSCLC Best Percentage Change From Baseline T-DXd 6.4 mg/kg Q3W (n = 50) DESTINY-Lung02 (n = 152) Confirmed ORR, n (%) (95% CI) 28, 56.0 (41.3 70.0) a a CR, n (%) 2 (4.0) PR, n (%) 26 (52.0) Median DoR, mo (95% CI) NE (8.3 NE) Median follow-up, mo (range) 11.8 (0.6 21.0) aPatients who had zero best percentage change from baseline in the sum of diameters for all target lesions. CR = complete response; DoR = duration of response; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor; HER2mt = human epidermal growth factor receptor 2 mutant; NE = not estimable; NSCLC = non small cell lung cancer; ORR = objective response rate; PD-(L)1 = programmed cell death-(ligand)1; PR = partial response; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan; TKI = tyrosine kinase inhibitor. Goto K, et al. J Clin Oncol. 2023;JCO2301361. 13 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
DESTINY-Lung02 Primary Results: OS T-DXd Kaplan Meier Curves for OS Median OS of T-DXd 5.4 mg/kg Q3W 19.5 mo (95% CI, 13.6 NE) Median OS of T-DXd 6.4 mg/kg Q3W NE (95% CI, 12.1 NE) ESMO = European Society for Medical Oncology; NE = not estimable; OS = overall survival; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan. Goto K, et al. J Clin Oncol. 2023;JCO2301361. 14 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
HER2 ADCs: T-DXd DESTINY-Lung011 DESTINY-Lung022 HER2-mutated nonsquamous NSCLC with disease progression after 1 prior systemic therapy HER2-mutated NSCLC OR, 55% (95% CI, 44% 65%) mPFS, 8.2 mo (95% CI, 6.0 11.9 mo) mOS, 17.8 mo (95% CI, 13.8 22.1 mo) 5.4 mg/kg Q3W OR, 49% (95% CI, 39.0% 59.1%) mPFS, 9.9 mo (95% CI, 7.4 NE) mOS,19.5 mo (95% CI, 13.6 NE) 6.4 mg/kg Q3W OR, 56% (95% CI, 41.3% 70.0%) mPFS,15.4 mo (95% CI, 8.3 NE) mOS, NE (95% CI, 12.1 NE) aData cutoff: June 22, 2022. bMedian DoR based on Kaplan-Meier estimate. ADC = antibody-drug conjugate; CI = confidence interval; DoR = duration of response; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; mOS = median overall survival; mPFS = median progression-free survival; NE = not estimable; NSCLC = non small cell lung cancer; OR = objective response; PD-(L)1 = programmed death-ligand; Q3W = every 3 weeks; T-DXd = trastuzumab deruxtecan; TKI = tyrosine kinase inhibitor. 1. Li BT, et al. N Engl J Med. 2022;386(3):241 251; 2. Goto K, et al. J Clin Oncol. 2023;JCO2301361. 15 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
DESTINY-Lung01 Drug-Related AEs Event Grade 3 Grade 4 Grade 5 Overall Grades 1 2 Number of patients (%) Drug-related AE 46 (51) 37 (41) 4 (4) 1 (1)a 88 (97) Drug-related AEs with 20% incidence Nausea 58 (64) 8 (9) 0 0 66 (73) Adjudicated drug-related ILD occurred in 24/91 patients (26%) at 6.4 mg/kg Fatigueb 42 (46) 6 (7) 0 0 48 (53) Alopecia 42 (46) 0 0 0 42 (46) Vomiting 33 (36) 3 (3) 0 0 36 (40) Neutropeniac 15 (16) 14 (15) 3 (3) 0 32 (35) Anemiad 21 (23) 9 (10) 0 0 30 (33) Diarrhea 26 (29) 2 (2) 1 (1) 0 29 (32) Decreased appetite 27 (30) 0 0 0 27 (30) Leukopeniae 17 (19) 4 (4) 0 0 21 (23) Constipation 20 (22) 0 0 0 20 (22) aOne patient had grade 5 (ie, fatal) pneumonitis that was assessed as drug-related by the investigator (subsequently adjudicated as ILD). Another patient had grade 3 ILD, as reported by the investigator, and died; the reported ILD was subsequently adjudicated as grade 5 by the ILD adjudication committee. bThis category includes the preferred terms fatigue, asthenia, and malaise. cThis category includes the preferred terms neutrophil count decreased and neutropenia. dThis category includes the preferred terms hemoglobin decreased, red cell count decreased, anemia, and hematocrit decreased. eThis category includes the preferred terms white cell count decreased and leukopenia. AE = adverse event; ESMO = European Society for Medical Oncology; ILD = interstitial lung disease. Li BT, et al. N Engl J Med. 2022;386(3):241 251. 16 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
DESTINY-Lung02 Primary Results: Overall Safety Adjudicated Drug-Related ILD Adjudicated as drug- related ILD (n = 101)a T-DXd 5.4 mg/kg T-DXd 6.4 mg/kg (n = 50)a Overall Safety Drug-related TEAE, % Any grade, n% 13 (12.9) 14 (28.0) Grade 1 4 (4.0) 4 (8.0) Grade 2 7 (6.9) 9 (18.0) Grade 3 1 (1.0) 0 Grade 4 0 0 Grade 5 1 (1.0) 1 (2.0) Median treatment duration was 7.7 months (range, 0.7 20.8) with T-DXd 5.4 mg/kg and 8.3 months (range, 0.7 20.3) with T-DXd 6.4 mg/kg The most common any-grade TEAEs in the T-DXd 5.4 mg/kg and 6.4 mg/kg arms included nausea (67.3% and 82.0%), neutropenia (42.6% and 56.0%), and fatigue (44.6% and 50.0%) The most common grade 3 TEAEs in the T-DXd 5.4 mg/kg and 6.4 mg/kg arms included neutropenia (18.8% and 36.0%) and anemia (10.9% and 16.0%) aIncludes all randomly assigned patients who received 1 dose of T-DXd. ILD = interstitial lung disease; T-DXd = trastuzumab deruxtecan; TEAE = treatment-emergent adverse event. J nne P, et al. WCLC 2023. Mini oral presentation MA13.10. 17 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Based on DESTINY-Lung02 Results, T-DXd Received FDA Accelerated Approval in August 20221 Approved for adult patients with unresectable or metastatic NSCLC with HER2 mutations who have received prior systemic therapy2 This indication is approved under accelerated approval based on improvements observed in the DESTINY-Lung02 trial1 The approved recommended dose is 5.4 mg/kg given IV Q3W, based on results of DESTINY-Lung021,2 T-DXd SPC T-DXd is currently being evaluated as 1L therapy in HER2-mutated NSCLC in DESTINY-Lung043 1L = first-line; ESMO = European Society for Medical Oncology; FDA = US Food and Drug Administration; HER2 = human epidermal growth factor receptor 2; IV = intravenously; NSCLC = non small cell lung cancer; Q3W = every 3 weeks; SPC = summary of product characteristics; T-DXd = trastuzumab deruxtecan. 1. Enhertu Approved. AstraZeneca:2022. https://www.astrazeneca.com/media-centre/press-releases/2022/enhertu-approved-in-us-for-her2-mutant-nsclc.html. Accessed September 2023; 2. Enhertu Prescribing Information. November 2022; 3. ClinicalTrials.gov. https://www.clinicaltrials.gov/study/NCT05048797. Accessed September 2023. 18 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
DESTINY-Lung04: A Phase 3 Trial of T-DXd as 1L Treatment in Metastatic HER2mt NSCLC aHER2 mutations may be detected in tissue or ctDNA. bCrossover is not permitted. cInvestigator s choice of cisplatin or carboplatin. 1L = first-line; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt= human epidermal growth factor receptor 2 mutant; NSCLC = non small cell lung cancer; T-DXd = trastuzumab deruxtecan. Li BT, et al. ASCO 2022. Poster TPS9137. 19 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
TKIs TKI = tyrosine kinase inhibitor.
Older EGFR/HER2 TKIs in HER2mt NSCLC Target population Drug N ORR mPFS Toxicities Afatinib1 HER2mt 13 8% 16 weeks Diarrhea, vomiting, abdominal pain, skin rash, paronychia, fatigue, mucositis, dyspnea Afatinib2 HER2mt 27 13%a 3 mo Diarrhea/GI toxicity, skin rash Neratinib3 HER2mt 26 4% 5.5 mo Diarrhea (74%), nausea (43%), vomiting (41%) Dacomitinib4 HER2mt 26 12% 3 mo Diarrhea (90%), rash (73%) Mobocertinib5 HER2mt 136 0%, 22% 19%, 43%b 10.2 mo Diarrhea (83%), nausea (43%), rash (33%), vomiting (26%) a3/23 patients. bAt increasing doses of mobocertinib 5 40 mg/d, 80 mg/d total daily dose, 120 mg/d, and 160 mg/d in 70 patients with previously treated NSCLC and EGFR ex20ins mutations. EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion; GI = gastrointestinal; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant;ORR = objective response rate; mPFS = median progression-free survival; NSCLC = non small cell lung cancer; TKI = tyrosine kinase inhibitor. 1. Dziadziuszko R, et al. J Thorac Oncol. 2019;14:1086 1094; 2. Lai WV, et al. Eur JCancer. 2019;109:28 35; 3. Hyman DM, et al. Nature. 2018;554(7691):189 194; 4. Kris MG, et al. Ann Oncol. 2015;26:1421 1427; 5. Riely GJ, et al. Cancer Discov. 2021;11(7):1688 1699. 21 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Pyrotinib in the 1L Treatment of HER2mt NSCLC Pyrotinib is an oral, irreversible pan-ErbB family inhibitor TRAEs Reported in 10% of Patients Tumor Response TRAEs, n (%) CF Cohort (n = 28) CU Cohort (n = 12) ORR: CF: 35.7% CU: 16.7% All Grades 3/4 All Grades 3/4 Grades Grades Any AEs 27 (96.4) 3 (10.7) 11 (91.7) 4 (33.3) Diarrhea 24 (85.7) 0 (0) 11 (91.7) 2 (16.7) CF CU Rash 9 (32.1) 0 (0) 5 (41.7) 0 (0) Brain metastases AST increased 7 (25.0) 1 (3.6) 1 (8.3) 0 (0) Present Absent Creatinine increased 6 (21.4) 0 (0) 2 (16.7) 0 (0) Conjugated bilirubin increased 5 (17.9) 0 (0) 3 (25.0) 0 (0) PFS ALT increased 5 (17.9) 1 (3.6) 1 (8.3) 0 (0) Mouth ulcer 4 (14.3) 0 (0) 2 (16.7) 0 (0) Lymphocyte count decreased 4 (14.3) 0 (0) 2 (16.7) 0 (0) Bilirubin increased 3 (10.7) 0 (0) 1 (8.3) 0 (0) Serum uric acid increased 3 (10.7) 0 (0) 0 (0) 0 (0) Pruritus 3 (10.7) 0 (0) 0 (0) 0 (0) 1L = first-line; AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; CF = criteria fulfilled; CU = compassionate use; ErbB = erythroblastic leukemia viral oncogene; ESMO = European Society for Medical Oncology; HER2mt = human epidermal growth factor receptor 2 mutant; HR = hazard ratio; NSCLC = non small cell lung cancer; ORR = objective response rate; PFS = progression-free survival; RWS = real-world study; TRAE = treatment-related adverse event. Liu SM, et al. Nat Med. 2023;29(8):2079 2086. 22 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Poziotinib for HER2mt NSCLC: The ZENITH-20 Trial Poziotinib is an irreversible pan-ErbB family inhibitor BID = twice daily; EGFR = epidermal growth factor receptor; ErbB = erythroblastic leukemia viral oncogene; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; NSCLC = non small cell lung cancer; PFS = progression-free survival; QD = once daily; RECIST = Response Evaluation Criteria in Solid Tumors. Remon J, et al. Cancer Treat Rev. 2020;90:102105. 23 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Poziotinib in the Treatment of Previously Treated NSCLC With HER2 ex20ins Mutations ZENITH20-2 trial, cohort 2 (n = 90), previously treated patients; all patients treated at 16 mg QD Clinical Response (RECIST v1.1 by BICR) As-treateda (n = 90) Evaluableb (n = 74) Parameter Best % Change From Baseline ORR, n (%) 95% CI 25 (27.8)c 18.9 38.2 26 (35.1)d 24.4 47.1 Best Change From Baseline in Sum of Diameter (%) Best overall response, no. (%) CR 0 (0) 0 (0) PR 25 (27.8)c 26 (35.1)d SD 38 (42.2) 35 (47.3) PD 13 (14.4) 13 (17.6) NE 14 (15.6) 0 (0) DCR, n (%) 95% CI 63 (70.0) 59.4 79.2 61 (82.4) 71.8 90.3 DoR, mo, median (range) 95% CI 5.1 (1 14.1) 4.2 5.5 5.1 (0.9 14.1) 4.2 5.5 PFS, mo, median (range) 95% CI 5.5 (0.0 17.6) 3.9 5.8 5.5 (0.6 17.6) 3.9 6.2 aThe as-treated population was the primary analysis population and included all patients who received 1 dose of study medication. bThe evaluable population excluded patients from the as-treated population who did not have a target lesion at baseline and/or did not have sufficient follow-up to evaluate tumor response. cCR/PR confirmation required 28 days after first observation of CR/PR. dCR/PR confirmation required 21 days after first observation of CR/PR. BICR = blinded independent central reviews; CR = complete response; DCR = disease control rate; DoR = duration of response; ErbB = erythroblastic leukemia viral oncogene; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion; HER2 = human epidermal growth factor 2; NSCLC = non small cell lung cancer; NE = not estimable; ORR = objective response rate; PD = progressive disease; PFS = progression-free survival; PR = partial response; QD = once daily; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors version 1.1; SD = stable disease. Le X, et al. J Clin Oncol. 2022;40(7):710 718. 24 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Poziotinib in the 1L Treatment of NSCLC With HER2 ex20ins Mutations Antitumor Activity by ICR ZENITH20 trial, cohort 4 (n = 80) Treated at 16 mg QD and 8 mg BID Parameter As-treated population Evaluable population Total (N = 80) 16 mg QD (n = 47) 8 mg BID (n = 33) Total (N = 63) 16 mg QD (n = 41) 8 mg BID (n = 22) Outcomes ORR, n (%) 95% CI 31 (39) 28 50 21 (45) 30 60 10 (30) 16 49 31 (49) 36 62 21 (51) 35 67 10 (46) 24 68 Best % Change From Baseline mDoR (mo) 95% CI 5.7 4.6 11.9 5.7 4.6 11.9 5.7 4.6 11.9 5.7 4.6 11.9 NR NR Best Change From Baseline in Sum of Diameter (%) mPFS (mo) 95% CI 5.6 5.4 7.3 5.6 4.3 9.1 5.6 5.5 NR 5.6 5.3 7.2 5.6 4.1 7.3 5.6 5.5 NR PFS + censored 16 mg QD 8 mg QD PFS Best Overall Response CR PR SD PD NE Treatment Ongoing * 16 mg QD 8 mg QD 47 33 32 19 15 5 8 3 6 1 3 0 3 1 0 1L = first-line; BID = twice daily; CR = complete response; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion; HER2 = human epidermal growth factor 2; ICR = independent central review; mDoR = median duration of response; mPFS = median progression-free survival; NE = not estimable; NR = not reached; NSCLC = non small cell lung cancer; ORR = objective response rate; PD = progressive disease; PFS = progression-free survival; PR = partial response; QD = once daily; SD = stable disease. Cornelissen R, et al. J Thorac Oncol. 2023;18(8):1031 1041. 25 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Poziotinib: Safety Profile in Patients With Treatment-Nave NSCLC With HER2 ex20ins Mutations Poziotinib 16 mg QD, n (%) (n = 47) Grade 3 Poziotinib 8 mg BID, n (%) (n = 33) Grade 3 AEs (preferred term) Any Grade Grade 4/5 Any Grade Grade 4/5 47 (100) 33 (70) 0/1 (2) 32 (97) 24 (73) 2 (6)/0 Patients with 1 event Rash (multiple terms)a 46 (98) 21 (45) 0 27 (82) 13 (39) 0 Diarrhea 39 (83) 7 (15) 0 28 (85) 7 (21) 0 Stomatitis (multiple terms)b 38 (81) 10 (21) 0 24 (73) 5 (15) 0 Paronychia 23 (49) 5 (11) 0 18 (55) 4 (12) 0 Alopecia 16 (34) 0 0 13 (39) 0 0 Dry skin 16 (34) 1 (2) 0 10 (30) 1 (3) 0 Decreased appetite 15 (32) 0 0 13 (39) 1 (3) 0 Nausea 13 (28) 0 0 10 (30) 0 0 Weight decreased 12 (26) 1 (2) 0 8 (24) 0 0 Dysgeusia 9 (19) 0 0 10 (30) 1 (3) 0 Pruritus 9 (19) 3 (6) 0 9 (27) 0 0 Skin fissures 9 (19) 1 (2) 0 8 (24) 1 (3) 0 Fatigue 8 (17) 2 (4) 0 11 (33) 1 (3) 0 Vomiting 7 (15) 1 (2) 0 7 (21) 1 (3) 0 Dry mouth 7 (15) 0 0 6 (18) 0 0 Hypokalemia 6 (13) 3 (6) 0 6 (18) 2 (6) 2 (6)/0 Dizziness 5 (11) 0 0 2 (6) 0 0 Pneumonitis 2 (4) 0 0/1 (2) 1 (3) 1 (3) 0 aRash includes dermatitis acneiform, palmar-plantar erythrodysesthesia syndrome, rash, rash erythematous, rash generalized, rash maculopapular, and rash popular. bStomatitis includes mucosal inflammation and stomatitis. AE = adverse event; BID = twice daily; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion; HER2 = human epidermal growth factor 2; NSCLC = non small cell lung cancer; QD = once daily. Cornelissen R, et al. J Thorac Oncol. 2023;18(8):1031 1041. 26 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Zongertinib (BI 181063) Selective HER2 TKI Previous ErbB TKIs Zongertinib HER2 TKD mutations, including ex20ins HER2 TKD mutations, including ex20ins Tumor cell wt HER2 HER2mt wt EGFR wt EGFR wt HER2 HER2mt Limited activity against ex20ins Active against ex20ins wt EGFR sparing wt EGFR blocked More AEs expected Fewer AEs expected Common AEs caused by blocking EGFR GI Skin AE = adverse event; EGFR = epidermal growth factor receptor; ErbB = erythroblastic leukemia viral oncogene; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertion; GI = gastrointestinal; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; TKD = tyrosine kinase domain; TKI = tyrosine kinase inhibitor; wt = wild type. Heymach J, et al. ASCO 2023. Abstract 8545. 27 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Beamion LUNG-1 Phase 1 study of zongertinib in patients with advanced/metastatic solid tumors with HER2 aberrations, including HER2mt NSCLC Phase 1a: Dose Escalation Phase 1b: Dose Expansion (in Patients With HER2mt NSCLC) (in Patients With Advanced Solid Tumors With HER2 Aberrationsa) Cohort 1 Cohort 1 1 oral dose, BID, 3-week cycles Interim futility analyses Cohort 2 Cohort 2 Cohort 5 n 36 patients Cohort 5 150 mg Cohort 3 (experimental) Cohort 4 (experimental) 100 mg 60 mg 30 mg 360 mg Ongoing 15 mg Cohort 1: Pretreated NSCLCb with a HER2 TKD mutation 300 mg Planned 240 mg Cohort 2: Treatment-na ve NSCLC with a HER2 TKD mutation 180 mg 120 mg Cohort 3: NSCLC with a non-TKD HER2 mutation n 30 patients 60 mg NSCLC with a HER2 TKD mutation active brain metastases Cohort 4: 1 oral dose, QD, 3-week cycles Cohort 5: NSCLC with a HER2 TKD mutation and prior treatment with HER2 directed ADCs aOverexpression, amplification, somatic mutation, or gene rearrangement involving HER2 or NRG1. bExcluding patients treated with ADCs. Phase 1a primary endpoint: MTD and DLTs (MTD evaluation period); Phase 1b primary endpoint: objective response, according to RECIST v1.1. ADC = antibody-drug conjugate; BID = twice daily; DLTs = dose-limiting toxicities; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; MTD = maximum tolerated dose; NRG1 = neuregulin 1; NSCLC = non small cell lung cancer; QD = once daily; RECIST v1.1 = Response Evaluation Criteria in Solid Tumors, version 1.1; TKD = tyrosine kinase domain. Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08. 28 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Beamion LUNG-1: Patient Characteristics Total (N = 50) 60.5 (31 79) Baseline Characteristics Median age, y (range) Gender, n (%) Male Race, n (%) White Asian ECOG PS, n (%) 0 1 Prior lines of therapy, n (%)a 2 >2 HER2 aberration, n/N tested (%)b Mutation Amplification Overexpressionc Rearrangement involving HER2 or NRG1 Lung cancer, unspecified (8%) 26 (52.0) 17 (34.0) 32 (64.0) Colorectal cancer (6%) NSCLC (65%) N=50a 17 (34.0) 33 (66.0) 15 (34.9) 20 (40.0) 26 (52.0) Endometrial (4%) Other tumors (17%) 28/48 (58.3) 4/5 (80.0) 9/12 (75.0) 10/48 (21.0) Data cutoff: July 17, 2023. a4 patient (8.0%) had missing data. b2 patients (4.0%) had missing data. c1+, 2+, or 3+ on immunohistochemistry. ECOG PS = Eastern Cooperative Oncology Group performance status; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; NRG1 = neuregulin 1; NSCLC = non small cell lung cancer. Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08. 29 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Beamion LUNG-1: Antitumor Response in Phase 1a Best Percentage Change From Baseline Best Overall Treatment Response 100 Overall (N = 46)a ORR: 41.3% DCR: 91.3% NSCLC (n = 34)a ORR: 50.0% DCR: 97.1% Best Change From Baseline in Target Lesions (%)a NSCLC Overall (N = 46)a NSCLC (n = 34)a 80 n (%) Other 60 ORR 19 (41.3) 0 (0) 19 (41.3) 23 (50.0) 17 (50.0) 0 (0) 17 (50.0) 16 (47.1) CR PR SD 40 20 0 20 40 PR: 7/11 (63.6%) 60 SD: 3/11 (27.3%) Esophagus 80 Biliary tract A775_G776 insYVMA (n = 11b) PD: 1/11 (9.1%) 100 Data cutoff: July 17, 2023. aPatients with 1 postbaseline tumor assessment or discontinued before first assessment for any reason. bPatients where mutation information was provided by the sites (which was optional in Phase 1a). CR = complete response; DCR = disease control rate; ESMO = European Society for Medical Oncology; insYVMA = YVMA insertion; NE = not estimable; NSCLC = non small cell lung cancer; ORR = objective response rate; PD = progressive disease; PR = partial response; SD = stable disease. Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08. 30 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Beamion LUNG-1: Treatment Response in Phase 1a Zongertinib Treatment Response Over Time 62% Patients still on treatment as of July 17, 2023 Patients 7.5 (1 24) Median number of cycles (range) PR SD PD Ongoing 500 0 50 100 150 200 250 300 350 400 450 TimeSince Treatment Start (days) ESMO = European Society for Medical Oncology; PD = progressive disease; PR = partial response; SD = stable disease. Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08. 31 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Beamion LUNG-1: Phase 1a Dose Escalation and Safety Zongertinib BID (n = 17) Zongertinib QD (n = 33) Total (N = 50) Phase 1a TRAEs (%)a Grade 3 5.9 Grade 3 12.1 Grade 3 10.0 Any 76.5 Any 84.8 Any 82.0 Most TRAEs were grade 1 or 2 3 1 1 Any TRAE Patients with DLTs during the on-treatment period Diarrhea 47.1 36.4 40.0 AST increased 5.9 18.2 3.0 14.0 2.0 Rashb 11.8 15.2 14.0 Patient with TRAE leading to treatment discontinuation (grade 3 ALT increased) ALT increased 5.9 5.9 15.2 6.1 12.0 6.0 Paronychia 5.9 12.1 10.0 Patient with serious TRAEs (grade 3 ALT and AST increased) Dry skin 11.8 6.1 8.0 Anemia 11.8 6.1 8.0 a 8% of total patients. bCombined term, includes rash, rash maculopapular, and dermatitis acneiform. ALT = alanine aminotransferase; AST = aspartate aminotransferase; BID = twice daily; DLTs = dose-limiting toxicities; ESMO = European Society for Medical Oncology; QD = once daily; TRAEs = treatment-related adverse event. Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08. 32 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Beamion LUNG-1 (Phase 1b): Antitumor Activity in Previously Treated NSCLC With HER2 TKD Mutations 100 Best Change From Baseline in Target Lesions (%)a 73.9% (53.5% 87.5%) ORR (95% CI): 80 60 Overall (N = 23)b 40 Patients included had between 2 and 5 cycles of treatment at cutoff 20 0 DCR: 91.3% 20 Median best percentage change from baseline in target lesions: 41.2% 40 60 80 100 aPatients who started treatment 7 weeks prior to the snapshot date with baseline and postbaseline tumor assessments.bPatients who started treatment 7 weeks prior to the snapshot date. CI = confidence interval; DCR = disease control rate; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; NSCLC = non small cell lung cancer; ORR = objective response rate; TKD = tyrosine kinase domain. Yamamoto N, et al. WCLC 2023. Mini Oral Presentation MA13.08. 33 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
ELVN-002: Preclinical Activity ELVN-002 is a potent, irreversible inhibitor of HER2 with a >100-fold selectivity over EGFR1 ELVN-002 showed preclinical activity in xenograft models, including an intracranial model, driven by wt HER2 and HER2mt and was well tolerated in all models tested.1 It is now being evaluated in a phase 1 study in HER2mt solid tumors2 ELVN-002 Antitumor Activity and Additive Activity With T-DXd3 CNS anti-tumor activity in NCI-N87 HER2 wild type intracranial model3 Tumor growth inhibition in Beas2b HER2 YVMA xenograft3 Kp,uu (free brain concentration)a 12 h 16 h (4 h Tucatinib) (8 h Tucatinib) aKp,uu is the unbound brain to plasma partition coefficient, which is used to define the unbound drug concentration in the brain relative to blood with a reference. Kp,uu = Free brain concentration (total brain concentration adjusted for brain tissue binding)/Free plasma concentration (total plasma concentration adjusted for protein binding). BID = twice daily; CNS = central nervous system; EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor; HER2mt = human epidermal growth factor receptor 2 mutant; Q3W = every 3 weeks; QD = once DAILY; T-DXd = trastuzumab deruxtecan; TGI = tumor growth inhibition; wt = wild type. 1. Aujay M, et al. Cancer Res. 2023;83(7_suppl):4019; 2. ClinicalTrials.gov. https://www.clinicaltrials.gov/study/NCT05650879. Accessed September 2023; 3. Bowyer S, et al. WCLC 2023. Poster P2.09. 34 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
ELVN-002: Phase 1 Study in Solid Tumors With HER2 Mutations, Amplification, or Overexpression ELVN-002-001 is a first-in-human, Phase 1, open-label, multicenter, dose-escalation and -expansion study to evaluate the safety, tolerability, PK, and preliminary antitumor activity of ELVN-002 monotherapy and in combination with T-DXd or T-DM1 in patients with solid tumors with HER2 alterations, including HER2mt NSCLC and HER2-overexpressed metastatic breast cancer Phase 1b: Monotherapy Dose Expansion Phase 1a: ELVN-002 Monotherapy Dose Escalationa RD b DL1 aSuccessive cohorts will receive escalating doses of QD ELVN-002. Dose escalation decisions will follow a Bayesian design. Dosing will be continuous in 21-day cycles until disease progression or unacceptable toxicity. Dose escalation may continue until the maximum tolerated dose is identified. 2 RDs for phase 1b monotherapy expansion will be chosen. Evaluation of BID regimen and intermediate dose levels may occur upon approval of the Safety Review Committee. Dose exploration may consist of up to 30 patients who may be enrolled at 1 dose level to further evaluate the safety, tolerability, PK, and clinical activity. A maximum of 10 patients may be enrolled at any given dose level. bSingle-patient cohort. BID = twice daily; DL = dose level; ESMO = European Society for Medical Oncology; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; NSCLC = non small cell lung cancer; PK = pharmacokinetics; QD = once daily; RD = recommended dose; T-DM1 = ado-trastuzumab emtansine; T-DXd = trastuzumab deruxtecan. Bowyer S, et al. WCLC 2023. Poster P2.09. 35 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain
Summary and Conclusions HER2mutations occur in 1% 4% of NSCLC1 3 ex20ins are most common, but point mutations in the tyrosine kinase, transmembrane, and extracellular domain are also observed1 3 T-DXd has accelerated FDA approval for HER2mt NSCLC after prior systemic therapy4 The clinical development of EGFR/HER2 TKIs for HER2mt NSCLC has been limited by significant toxicities (largely EGFR-related)5 9 Novel HER2-specific TKIs (zongertinib, ELVN-002) are now in clinical development10 13 EGFR = epidermal growth factor receptor; ESMO = European Society for Medical Oncology; ex20ins = exon 20 insertions; FDA = US Food and Drug Administration; HER2 = human epidermal growth factor receptor 2; HER2mt = human epidermal growth factor receptor 2 mutant; NSCLC = non small cell lung cancer; T-DXd = trastuzumab deruxtecan; TKI = tyrosine kinase inhibitor. 1. Jebbink M, et al. Cancer Treat Rev. 2020;86:101996; 2. Yu X, et al. Front Oncol. 2022;12:860313; 3. Arcila ME, et al. Clin Cancer Res. 2012;18:4910 4918; 4. Enhertu Approved. AstraZeneca:2022. Accessed September 2023; 5. Dziadziuszko R, et al. J Thorac Oncol. 2019;14:1086 1094; 6. Lai WV, et al. Eur JCancer. 2019;109:28 35; 7. Hyman DM, et al. Nature.2018;554(7691):189 194; 8. Kris MG, et al. Ann Oncol. 2015;26:1421 1427; 9. Son J, et al. Cancer Res. 2022;82(8):1633 1645; 10. Heymach J, et al. ASCO 2023. Abstract 8545; 11. Seymour C. OncLive 2023. https://www.onclive.com/view/zongertinib-proves-clinically-active-with-low-rate-of-egfr-mediated-aes-in-her2-mutant-solid-tumors. Accessed September 2023; 12. ClinicalTrials.gov. https://classic.clinicaltrials.gov/ct2/show/NCT05650879. Accessed September 2023; 13. Aujay M, et al. AACR 2023, Poster 4019. 36 ESMO Annual Meeting, 20 24 October 2023, Madrid, Spain







")


















 – Selective HER2 TKI")





: Antitumor Activity in")