Affinity Care Lipid Pathway Summary and Assessment
Affinity Care Lipid Pathway
Yes
Person over 16yrs has cholesterol and lipids
assessment (ensure Hba
1
c is also assessed)
A
s
s
e
s
s
i
n
g
L
i
p
i
d
/
C
h
o
l
e
s
t
e
r
o
l
b
l
o
o
d
r
e
s
u
l
t
s
Does the patient have established
diabetes or vascular disease
(CAD,PAD,TIA,CVA)
Patient
does not have
known FH
or CVD
Lifestyle advice to minimize all
CVD risk factors
Qrisk <10% at 10 years
Commence atorvastatin 40mg
(or rosuvastatin 20mg if previous
intolerant simvastatin or
atorvastatin)
Yes
Total Cholesterol > 7.5mmol/l
or
LDL Cholesterol > 4.9
Using Dutch Lipid Score assess for
Familial Hypercholeserolaemia
(FH) and refer as appropriate
Are they taking atorvastatin 40-
80mg
(or rosuvastatin 10-20mg)?
Commence atorvastatin 80mg
(or rosuvastatin 20mg if previous
intolerant simvastatin or atorvastatin)
Total Cholesterol > 4.0mmol/l
or
LDL Cholesterol > 2.6mmol/l
Recheck lipid profile at 3 months
(or later)
Add ezetimibe 10mg
Recheck lipid profile at 3 months
(or later)
Continue annual reassessment
Ensure all CVD risk factors
minimized
Refer to the Affinity Lipid Group
Qrisk assessment
Qrisk >10% at 10 years
Lifestyle advice to minimize all
CVD risk factors and reassess CVD
risk in 3 years
Continue lifestyle advice to minimize
all CVD. No need for cholesterol/lipid
assessment. LFTs do not need 3
month review
unless deranged prior
to initiation of statin
STATIN DECLINED
Continue lifestyle advice to minimize all CVD
there is no need for further cholesterol/lipid
assessment
Patient is confirmed to have FH
Total Cholesterol > 4.0mmol/l
or
LDL Cholesterol > 2.6mmol/l
Total Cholesterol > 4.0mmol/l
or
LDL Cholesterol > 2.6mmol/l
Aim to achieve at least a 50%
reduction of LDL-C (or non-fasting
non-HDL-C) from baseline in line
with secondary prevention
protocol
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
Continue annual reassessment
Ensure all CVD risk factors
minimized
Patient unable to take statins
Yes
No
Yes
CVD
FH
Affinity Care PCN December 2021
Add
Nustendi
Total Cholesterol > 4.0mmol/l
or
LDL Cholesterol > 2.6mmol/l
No
Yes
D
u
t
c
h
L
i
p
i
d
N
e
t
w
o
r
k
S
c
o
r
e
When assessment completed, if the patient is
eligible, please refer to:
Jillian Webster
Familial Hypercholesterolaemia Specialist Nurse
Huddersfield Royal Infirmary
Pathology Lab, Basement,
Acre Street , Lindley
Huddersfield
HD3 3EA
Affinity Care PCN December 2021
M
e
d
i
c
a
t
i
o
n
P
a
t
h
w
a
y
f
o
r
S
e
c
o
n
d
a
r
y
P
r
e
v
e
n
t
i
o
n
Does the patient have
established vascular disease
(CAD,PAD,TIA,CVA)
Patient unable to take statins
Are they taking atorvastatin
40-80mg
(or rosuvastatin 10-20mg)?
Total Cholesterol <4.0mmol/l or LDL Cholesterol<2.6mmol/l NICE
Patient choice to add
ezetimibe 10mg
Total Cholesterol < 4.0mmol/l
or
LDL Cholesterol < 2.6mmol/l
Commence atorvastatin 80mg
(or rosuvastatin 20mg if previous
intolerant simvastatin or atorvastatin)
Add
Nustendi
Total Cholesterol < 4.0mmol/l
or
LDL Cholesterol <2.6mmol/l
Add inclisiran
Continue annual reassessment
Ensure all CVD risk factors
minimized
Patient unable to take
Nustendi
Patient
unable to take
ezetimibe
Add inclisiran
Ezetimibe
:-Lipids and LFTs should be
checked after 8 weeks and ezetimibe
stopped if the ALT has risen to 3x
upper limit of normal
Nustendi
:-Lipids and LFTs should be
checked after 8 weeks and
Nustendi
stopped
if the ALT has risen to 3x
upper limit of normal
Inclisiran:
-
After first injection check
LDL-C and Lipids at 6 weeks.
After second injection check LDL-C
and Lipids at 6 weeks.
Secondary Care Lipid Clinic
If the person has multiple medicine
intolerance and /or the LDL-
Cholesterol can not be reduce to
≤2.6mmol/l then consider referral for
consideration of PCSK9i
No
No
No
Yes
No
Yes
Yes
Patient declines all lipid
intervention
*NICE TA733 suggests either adding ezetimibe or inclisiran
Patient choice to add
inclisiran
Affinity Care PCN December 2021
LDL Cholesterol
<4.0mmol/l
(high CVD risk)
<3.5mmol/l (very high
r
isk)
Add evolocumab
Yes
No
Patient unable to
use
evolocumab
Healthy Lifestyle advice
Known Cardiovascular Disease
Known Occlusive
Cardiovascular
Disease
No known Occlusive Cardiovascular Disease
Qrisk2
Assessment
>10% at 10
years
Continue healthy
lifestyle and 3
yearly
assessment
Atorvastatin
80mg
Type 2 Diabetes
or
CKD 3
Hypertension
Atorvastatin
40mg
Atorvastatin
40mg
Type 2 Diabetes
With additional
CVD risk factors
*
Atorvastatin
80mg
Atorvastatin
40mg
*
C
V
D
R
i
s
k
F
a
c
t
o
r
s
:
S
t
a
t
i
n
s
U
s
e
i
n
C
a
r
d
i
o
v
a
s
c
u
l
a
r
D
i
s
e
a
s
e
If patient complains of muscle pain attributed to atovastatin
Check CPK and discontinue statin
CPK
≥
5x upper limit of
normal
CPK <5x upper limit of
normal
Recheck in 14 days
Remain off atorvastatin for
6 weeks
Recommence atorvastatin
at 50% of previous dose
Return of previous
symptoms
Continue atorvastatin at
this dose
Stop atorvastatin for 6
weeks, then commence
rosuvastatin 5mg
CPK remains
≥
5x upper
limit of normal
Consider referral to
investigate elevated CPK
Return of previous
symptoms
Up titrate rosuvastatin to:
High intensity:
Rosuvastatin 20mg
Low intensity:
Rosuvastatin 10mg
•
Albuminuria
•
CKD 3 or worse
•
Erectile
dysfunction
•
FH premature
CVD
•
Hypertension
•
LDL>2.6mmol/l
•
Psoriasis
•
Smoking
Yes
No
Yes
No
Discontinue statin and
code intolerance
Yes
No
Affinity Care PCN December 2021
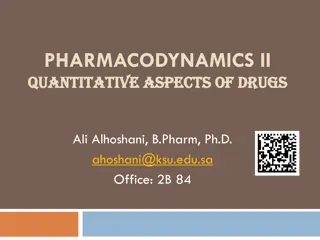
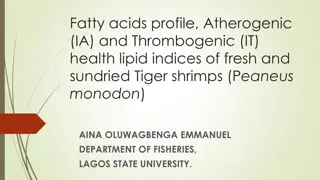
The Affinity Care Lipid Pathway outlines a systematic approach to assessing lipid/cholesterol blood results in individuals over 16 years old. It includes guidelines for managing cholesterol levels, assessing familial hypercholesterolemia, and determining appropriate medication options based on individual risk factors and existing conditions. The pathway emphasizes the importance of minimizing cardiovascular disease risk factors and provides guidance on lifestyle modifications and statin therapy for optimal lipid management. Monitoring and reassessment protocols are also detailed to ensure ongoing management and risk reduction.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Assessing Lipid/Cholesterol blood results Assessing Lipid/Cholesterol blood results Person over 16yrs has cholesterol and lipids assessment (ensure Hba1c is also assessed) Total Cholesterol > 7.5mmol/l or LDL Cholesterol > 4.9 Continue annual reassessment Ensure all CVD risk factors minimized Yes No No Using Dutch Lipid Score assess for Familial Hypercholeserolaemia (FH) and refer as appropriate Yes Does the patient have established diabetes or vascular disease (CAD,PAD,TIA,CVA) Are they taking atorvastatin 40- 80mg (or rosuvastatin 10-20mg)? Total Cholesterol > 4.0mmol/l or LDL Cholesterol > 2.6mmol/l Yes Yes Add ezetimibe 10mg No No CVD No Yes Commence atorvastatin 80mg (or rosuvastatin 20mg if previous intolerant simvastatin or atorvastatin) Patient does not have known FH or CVD Recheck lipid profile at 3 months (or later) Recheck lipid profile at 3 months (or later) Patient is confirmed to have FH Yes Yes Yes FH Lifestyle advice to minimize all CVD risk factors Aim to achieve at least a 50% reduction of LDL-C (or non-fasting non-HDL-C) from baseline in line with secondary prevention protocol Patient unable to take statins Total Cholesterol > 4.0mmol/l or LDL Cholesterol > 2.6mmol/l Total Cholesterol > 4.0mmol/l or LDL Cholesterol > 2.6mmol/l Add Nustendi No Yes Qrisk assessment Total Cholesterol > 4.0mmol/l or LDL Cholesterol > 2.6mmol/l Continue annual reassessment Ensure all CVD risk factors minimized No Refer to the Affinity Lipid Group Yes Qrisk <10% at 10 years Qrisk >10% at 10 years Equivalence Dose Dose Considerations Commence atorvastatin 40mg (or rosuvastatin 20mg if previous intolerant simvastatin or atorvastatin) Atorvastatin 40mg 80mg No renal considerations Reduced interaction profile Rosuvasatin 20mg 40mg Avoid if eGFR <30. Max dose 20mg if eGFR 30-60 Reduced interaction profile Pravastatin 40mg Start 10mg reduced renal function Reduced interaction profile Continue lifestyle advice to minimize all CVD. No need for cholesterol/lipid assessment. LFTs do not need 3 month review unless deranged prior to initiation of statin STATIN DECLINED Lifestyle advice to minimize all CVD risk factors and reassess CVD risk in 3 years Continue lifestyle advice to minimize all CVD there is no need for further cholesterol/lipid assessment Simvastatin 40mg Max dose 10mg if eGFR <10 High interaction profile Affinity Care PCN December 2021
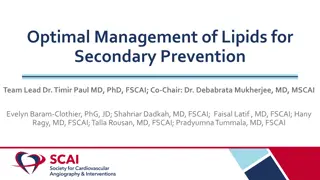
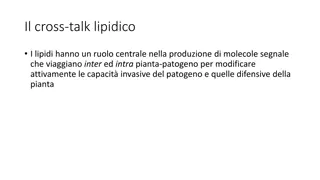
Dutch Lipid Network Score Dutch Lipid Network Score Genotype Scoring Criteria for Patients with a clinical diagnosis of Familial Hypercholesterolemia Please note these criteria only apply for index case, not family members of a known genotype positive patients Points 1st or 2nd Degree relatives Known with premature (<60yrs) CHD Known with premature (<45yrs) CHD Known with LDL-C >4.9mmol/l (or total cholesterol >7.5mmol/l) Known with LDL-C >4.0mmol/l (or total cholesterol >6.7mmol/l) Please specify relation to index case Tendon xanthomata (in 1st/2nd degree relatives) Premature corneal arcus (no score arcus senilis) 1 2 1 Family History When assessment completed, if the patient is eligible, please refer to: 2 Jillian Webster Familial Hypercholesterolaemia Specialist Nurse Huddersfield Royal Infirmary Pathology Lab, Basement, Acre Street , Lindley Huddersfield HD3 3EA 6 4 Physical Examination Patient has premature CHD (<45 yrs) Patient has premature CHD (<50 yrs) Patient has premature CHD (<60 yrs) Patient has premature Stroke/TIA or PVD (<60 yrs) 4 3 2 1 Clinical History LDL-Cholesterol 8.5 LDL-Cholesterol 6.5-8.4 LDL-Cholesterol 5.0-6.4 LDL-Cholesterol 4.0-4.9 Triglyceride 2.5-3.4 Triglyceride 3.5-4.9 Triglyceride 5.0 8 5 3 1 Untreated or Corrected LDL- cholesterol Minus 2 Minus 3 Minus 4 Fasting Triglycerides Please record in referral any secondary issue that may predispose to raised TG s such as diabetes TOTAL SCORE 6 or above eligible for genotyping 5 or less usually not eligible except in exceptional circumstances Eligibility for FH genotyping Affinity Care PCN December 2021
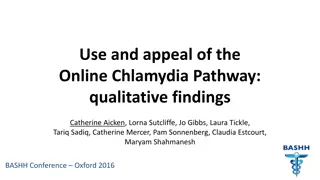
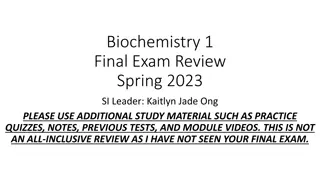
Medication Pathway for Secondary Prevention Medication Pathway for Secondary Prevention Does the patient have established vascular disease (CAD,PAD,TIA,CVA) Ezetimibe:-Lipids and LFTs should be checked after 8 weeks and ezetimibe stopped if the ALT has risen to 3x upper limit of normal Are they taking atorvastatin 40-80mg (or rosuvastatin 10-20mg)? Patient declines all lipid intervention Patient unable to take statins Yes No Commence atorvastatin 80mg (or rosuvastatin 20mg if previous intolerant simvastatin or atorvastatin) Patient unable to take Nustendi Add Nustendi Nustendi:-Lipids and LFTs should be checked after 8 weeks and Nustendi stopped if the ALT has risen to 3x upper limit of normal No LDL Cholesterol <4.0mmol/l(high CVD risk) <3.5mmol/l (very high risk) Total Cholesterol <4.0mmol/l or LDL Cholesterol<2.6mmol/l NICE Patient choice to add inclisiran Patient choice to add ezetimibe 10mg No Yes Inclisiran:-After first injection check LDL-C and Lipids at 6 weeks. Add evolocumab After second injection check LDL-C and Lipids at 6 weeks. Total Cholesterol < 4.0mmol/l or LDL Cholesterol < 2.6mmol/l Total Cholesterol < 4.0mmol/l or LDL Cholesterol <2.6mmol/l Yes Yes Patient unable to use evolocumab Patient unable to take ezetimibe Secondary Care Lipid Clinic If the person has multiple medicine intolerance and /or the LDL- Cholesterol can not be reduce to 2.6mmol/l then consider referral for consideration of PCSK9i No No Add inclisiran Add inclisiran Continue annual reassessment Ensure all CVD risk factors minimized Affinity Care PCN December 2021 *NICE TA733 suggests either adding ezetimibe or inclisiran
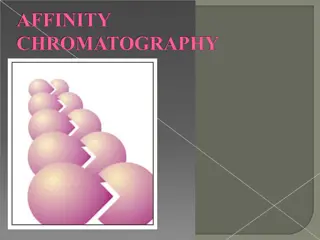
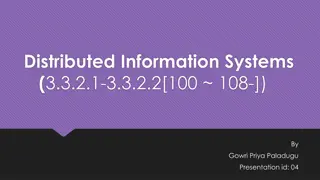
Statins Use in Cardiovascular Disease Statins Use in Cardiovascular Disease Healthy Lifestyle advice If patient complains of muscle pain attributed to atovastatin Check CPK and discontinue statin Known Cardiovascular Disease CPK 5x upper limit of normal CPK <5x upper limit of normal Remain off atorvastatin for 6 weeks Recheck in 14 days Known Occlusive Cardiovascular Disease No known Occlusive Cardiovascular Disease No CPK remains 5x upper limit of normal Recommence atorvastatin at 50% of previous dose Yes Qrisk2 Assessment >10% at 10 years Return of previous symptoms Consider referral to investigate elevated CPK Type 2 Diabetes With additional CVD risk factors* Type 2 Diabetes or CKD 3 Hypertension No Yes Stop atorvastatin for 6 weeks, then commence rosuvastatin 5mg Continue atorvastatin at this dose Continue healthy lifestyle and 3 yearly assessment Atorvastatin 80mg Atorvastatin 40mg Atorvastatin 40mg Atorvastatin 80mg Atorvastatin 40mg Return of previous symptoms No Yes Discontinue statin and code intolerance *CVD Risk Factors: Up titrate rosuvastatin to: Albuminuria CKD 3 or worse Erectile dysfunction FH premature CVD Hypertension LDL>2.6mmol/l Psoriasis Smoking Low intensity: Rosuvastatin 10mg High intensity: Rosuvastatin 20mg Affinity Care PCN December 2021