Evolution of Medicare and the Rise of Direct Contracting Entities

Explore the historical journey of Medicare from its inception to the introduction of Medicare Advantage and Direct Contracting Entities. Understand key acronyms, models, and initiatives shaping the current healthcare landscape, and delve into strategies to address challenges posed by the shift towards corporate involvement in healthcare delivery.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Direct Contracting Entities: Handing Traditional Medicare to Wall Street When Willie Sutton was asked why he robbed banks, he responded because that s where the money is PNHP Annual Conference, October 23-24, 2021 Ana Malinow, MD Past President, PNHP
Objectives Describe a brief history of Medicare, Medicare Advantage and the Medicare Money Machine Understand The Innovation Center and the Global and Professional Direct Contracting model Discuss a winnable strategy to stop Direct Contracting Entities
Medicare: A Tale of Many Acronyms TM Traditional (Original) Medicare CMMI Center for Medicare and Medicaid Innovation GPDC Global and Professional Direct Contracting Model DCEs Direct Contracting Entities PCPs Primary Care Practices, investor-owned primacy care practices MSOs Management service organizations that aggregate practices MA Medicare Advantage insurers SPACS Special purpose acquisition companies PE Private equity VC Venture capital firms IPO Initial public offerings
Health Care as a Human Right: American Style Congress passes Medicare to cover 65 y/o Part A (100% hospital) & Part B (80% outpatient) Medigap (supplemental private insurance to cover the 20% uncovered services) 1965 Commercial insurance introduces Medicare + Choice To give seniors a choice of HI plans To achieve the efficiencies of managed care in the private sector 1980s The Medicare Prescription Drug Improvement & Modernization Act (implemented 2006) Adds prescription drug benefit Renames & redesigns MC + Choice Medicare Advantage 2003 The Accountable Care Act establishes CMMI under CMS, gets $10 B every 10 years Test innovate payment and service delivery models to reduce program expenditures while preserving/enhancing QOC Has authority to issue regulations free of Congressional action & scale models to full Medicare program 2010 Source: Megellas, M. Medicare Modernization: The new prescription drug benefit and redesign Part B and Part C Proc (Bayl Univ Med Cent). 2006 Jan; 19(1): 21 23. McGuire TG, Newhouse JP, Sinaiko AD. An Economic History of Medicare Part C. Milbank Quarterly 2011 Jun;89(2):289-332 An Economic History of Medicare Part C (nih.gov)
The Market Explains Excessive US Health Care Costs: Unnecessary care due to financial incentives to maximize volume Physician Greed Patients Getting Too Much Care HMO ACO IDS DCE Deductibles Co-pays Co-insurance Using Market Forces to Control Prices
Medicare Beneficiaries & Spending Medicare Beneficiaries & Spending 1970-2020 926 523 $, Billion Beneficiaries, Million 222 62 47 36.8 39 34 28 111 20 7.5 1970 1980 1990 2000 2010 2020 Source: CMS Medicare Enrollment Dashboard https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics- Trends-and-Reports/CMSProgramStatistics/Dashboard CMS Medicare Enrollment National Trends 1966-2013 https://www.cms.gov/Research-Statistics-Data-and- Systems/Statistics-Trends-and-Reports/MedicareEnrpts/Downloads/SMI2013.pdf
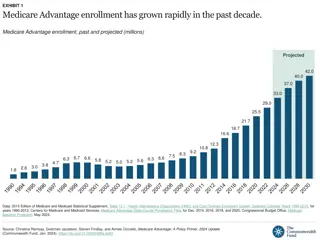
The Medicare Advantage The Medicare Advantage 271% Growth, 2000-2021 37 38 38 38 38 38 38 37 37 36 36 36 35 34 35 35 35 Traditional Medicare 34 35 35 32 33 Medicare Advantage 26 24 22 20 19 18 17 16 14 13 12 11 11 10 8 7 7 6 6 6 5 5 2000 2002 2004 2006 2008 2010 2012 2014 2016 2018 2020 Source: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Archives/MMSS and https://www.kff.org/medicare/ state-indicator/total-medicare-beneficiaries/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
Medicare Advantage Business Model For Dummies Minimal upgrades, market, repeat Insure the right population Upcode and make a profit Don t insure the wrong population Offer inexpensive premiums Sources: NBER. Differential Mortality in Medicare Advantage August 2019 Differential Mortality in Medicare Advantage | NBER GAO: Medicare Advantage: CMS Should Use Data on Disenrollment and Beneficiary Health Status to Strengthen Oversight April 2017 Medicare Advantage: CMS Should Use Data on Disenrollment and Beneficiary Health Status to Strengthen Oversight | U.S. GAO US Dept of Health & Human Services Office of Inspector General. Billions in Estimated Medicare Advantage Payments from Chart Reviews Raise Concerns. Dec 2019 https://innovation.cms.gov/innovation-models/gpdc-model DJ Myers and AW Trivedi, Private Medicare Advantage Plans Continue to Upcode for Bills in Extra Payments. Medical Care. APHA. Feb 2021 L Serna and A Johnson. MedPac. The Medicare Advantage program: Status report and a benchmark policy option http://www.medpac.gov/docs/default-source/meeting-materials/ma-status-medpac-dec-2020.pdf?sfvrsn=0 AA Markowitz et al. Medicare Advantage Plan Double Bonuses Drive Racial Disparity In Payments, Yield No Quality or Enrollment Improvements. Health Affairs, 9/21 https://www.healthaffairs.org/doi/10.1377/hlthaff.2021.00349
Risk Scores Drive MA Reimbursements Physician coding drives Risk Scores Typical Coding Baseline for age Obesity Type 2 Diabetes Major Depression CHF Asthma Ulcer, unspecified CHF*DM Risk Score = 1.03 CMS pays MA $9,000 HCC .45 0 .104 0 .323 0 0 .154 Maximized Coding Baseline for age Morbid Obesity DM w/ retinopathy MD, Sing Ep, Mild CHF, Class 3 COPD Ulcer, stage 3 CHF*DM,COPD Risk Score = 3.63 CMS pays MA $32,000 HCC .45 .273 .318 .395 .323 .328 1.204 .154, .19 For every 0.1 increase in risk score at current enrollment levels: $15 B overpayments ($13 B CMS + $2 B Part B beneficiaries) $3.5 B additional MA profits Sources: https://www.healthcatalyst.com/insights/5-ways-improve-hcc-coding-accuracy-risk-adjustment/ R Gilfillan, DM Berwick Medicare Advantage, Direct Contracting, And The Medicare Money Machine, Part 1: The Risk-Score Game. Health Affairs Blog Sept 29, 2021 9
The 2021 Medicare Pie The 2021 Medicare Pie Total 2021:$926 Billion Traditional Medicare 58%* Medicare Advantage 42% $537 Billion $389 Billion *63% have supplemental coverage through Medigap (34%) or ESHI retiree plan (29%) Source: Kaiser Family Foundation Medicare Advantage in 2021: Enrollment Update and Key Trends https://www.kff.org/medicare/issue- brief/medicare-advantage-in-2021-enrollment-update-and-key-trends/ and ttps://www.kff.org/medicare/issue-brief/a-snapshot-of-sources- of-coverage-among-medicare-beneficiaries-in-2018/ and https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends- and-Reports/NationalHealthExpendData/NHE-Fact-Sheet
R Gilfillan & D Berwick: The Medicare Gold Rush The Perverse Marketplace and Business Model of Medicare Advantage Wall Street Speculators Increase Average Valuation of Medicare Advantage Beneficiaries 1. Expected doubling of Medicare spending from $800B to $1.6T in 2028 as Baby Boomers age 2. CMS consistently overpays MA plans despite lack of clinical benefit 3. Distorted market dynamics from CMS overpayments 4. Direct Contracting Model to privatize part of the $1.6T spend $87,000 $7,000 Historical Current Source: R Gilfillan, DM Berwick Medicare Advantage, Direct Contracting and the Medicare Money Machine, Part 1: The Risk-Score Game. Health Affairs Blog Sept 29, 2021
Meanwhile, Back at the CMMI Farm Trump Administration vows to de-risk CMS Pass entire FFS to MA-like full-risk capitated arrangements 2017 GEO model: Involuntary assignment of all TM beneficiaries in 10 cities Inability to opt out of DCE 2019 Biden halts GEO but greenlights GLO-PRO 53 Direct Contracting Entities Defined provider network (although maintain access to all Medicare providers) Complex constraints on Risk Scoring, unclear enforcement, MLR ~60% Auto-alignment of potentially 30 M beneficiaries (claims-based or voluntary through PCP) 2021 Source: Centers for Medicare and Medicaid Services. Global and Professional Direct Contracting (GPDC) Model https://innovation.cms.gov/innovation-models/gpdc-model
Of the 53 GLO PRO DCEs on April 2021 Most Are Investor Owned Remember the 1980s? Give seniors a choice of HI plans to achieve the efficiencies of managed care in the private sector ? A mix of ACOs, some for-profit PCP groups, MSOs, and specialty providers 22 are either publicly traded or publicly backed by Private Equity and Venture Capital firms Provider -based DCEs 25 Investor- owned DCEs 28 Only 6 are owned by insurers, but they have the greatest potential Source: Ed Weisbart R. Gilfillan & D Berwick Medicare Advantage, Direct Contracting, And The Medicare Money Machine, Part 2: Building On The ACO Model. Health Affairs Blog. 9/30/2021 Data sources include April 8, 2021 CMS report https://innovation.cms.gov/media/document/gpdc-model-participant-announcement, accessed Sept. 19, 2021 13
UnitedHealth Group Inc Anthem Inc Humana Inc April 2010 August 2021 These 5 Insurers Entire S&P 500 Stock increased 280% Market cap increased Stock increased 825% Average market cap increased 497% Cigna Inc CVS Health Corp 245% Speculation on Speculation on Wall Street: Wall Street: Medicare Medicare Advantage/DCEs Advantage/DCEs is the place to be is the place to be Source: https://www.google.com/finance/ https://www.yardeni.com/
Take Action: Sign the Petition! Go to www.pnhp.org
Take Action Stop DCEs Now! Call or write your member of Congress, tell them to stop the DCE program and protect Medicare. Find a sample letter HERE Write a letter to the editor of your local news outlet. For writing and publishing tips, visit PNHP's guide Physicians: Collect letters that your patients receive from DCEs, send to anamalinow@gmail.com Seniors: If you receive a letter asking you to join a DCE, keep it and send to anamalinow@gmail.com Educate yourself and colleagues! Watch and share this webinar on DCEs featuring physicians, journalists and Rep. Katie Porter Collaborate with orgs & organize for NSP/MFA: it couldn t be more obvious Thank you Dr. Ed Weisbart for designing the slide deck