Understanding the Rise of Gram-Negative Bloodstream Infections in Healthcare

Gram-negative bloodstream infections (GNBSI) are becoming more prevalent in healthcare settings, posing a significant challenge due to increasing antimicrobial resistance. The prevalence of GNBSI is on the rise, causing concern for healthcare professionals globally. Strategies to combat GNBSI must be implemented to address this growing threat to patient safety.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Getting to grips with healthcare- associated Gram-negative bloodstream infection? Jon Otter, PhD FRCPath Imperial College London j.otter@imperial.ac.uk @jonotter Blog: www.ReflectionsIPC.com
Background and epi Drivers of GNBSI Learning from G+ success? How to tackle GNBSI
Background and epi Drivers of GNBSI Learning from G+ success? How to tackle GNBSI
Point prevalence Around 0.5 (2016 UK PPS) to 1% (2012 European PPS) of hospital inpatients will have a BSI at any one time. Zarb et al. Eurosurvellance 2012. European Point Prevalence Survey of HCAI.
Rising threat from AMR-GNR % of all HAI caused by GNRs. % of ICU HAI caused by GNRs. Acinetobacter baumannii Pseudomonas aeruginosa Stenotrophomonas maltophilia Klebsiella pneumoniae Escherichia coli Enterobacter cloacae Non-fermenters CPO Enterobacteriaceae CPE Hidron et al. Infect Control Hosp Epidemiol 2008;29:966-1011. Peleg & Hooper. N Engl J Med 2010;362:1804-1813.
Gram-negative BSIs are getting more common 18,000 3500 C. difficile - all cases E. coli BSI - all cases MRSA BSI - all cases MSSA BSI - all cases C. difficile - Trust-apportioned E. coli BSI - Trust-apportioned MRSA BSI - Trust-apportioned MSSA BSI - Trust-apportioned Number of cases (C. difficile infection and E. coli BSI) 16,000 Number of cases (MRSA BSI, MSSA BSI) 3000 14,000 2500 12,000 2000 10,000 8,000 1500 6,000 1000 4,000 500 2,000 -00 0 Apr-Jun 2015 Oct-Dec 2007 Apr-Jun 2007 Apr-Jun 2008 Oct-Dec 2008 Apr-Jun 2009 Oct-Dec 2009 Apr-Jun 2010 Oct-Dec 2010 Apr-Jun 2011 Oct-Dec 2011 Apr-Jun 2012 Oct-Dec 2012 Apr-Jun 2013 Oct-Dec 2013 Apr-Jun 2014 Oct-Dec 2014 Jan-Mar 2015 Oct-Dec 2015 Apr-Jun 2016 Oct-Dec 2016 Apr-Jun 2017 Oct-Dec 2017 Jul-Sept 2007 Jul-Sept 2008 Jul-Sept 2009 Jul-Sept 2010 Jul-Sept 2011 Jul-Sept 2012 Jul-Sept 2013 Jul-Sept 2014 Jul-Sept 2015 Jul-Sept 2016 Jul-Sept 2017 Jan-Mar 2008 Jan-Mar 2009 Jan-Mar 2010 Jan-Mar 2011 Jan-Mar 2012 Jan-Mar 2013 Jan-Mar 2014 Jan-Mar 2016 Jan-Mar 2017 Jan-Mar 2018 Data: Public Health England.
Gram-negative BSIs are getting harder to treat Data: ESPAUR 2018.
Carbapenem-resistant organisms, Europe 24.0 Carbapenem-resistant P. aeruginosa 22.0 Carbapenem-resistant K. pneumoniae 20.0 Multidrug-resistant K. pneumoniae 18.0 16.0 14.0 % Resistant 12.0 10.0 8.0 6.0 4.0 2.0 0.0 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 EARS-Net
BSIs are expensive Cassini et al. Plos Med 2016.
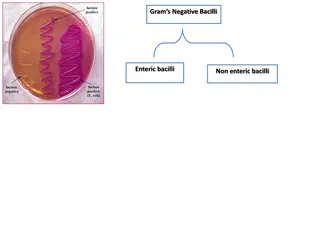
Enterobacteriaceae vs. non-fermenters Share Gram stain reaction Concerning AMR Differ Risk factors & at-risk population Potential for epidemic spread Infection profile & mortality Prevalence Colonisation site & duration Transmission routes Resistance profile & mechanisms
Whats the problem? Poor clinical outcome Enterobacteriaceae Non fermenters Organism AmpC / ESBL CPE A. baumannii Attributable mortality Moderate Massive (>50%) Minimal Shorr et al. Crit Care Med 2009;37:1463-1469. Patel et al. Iinfect Control Hosp Epidemiol 2008;29:1099-1106.
The emerging threat of AMR GNR! C. difficile +/- n/a Single HA Old + +++ Pathogen Resistance Resistance genes Species HA vs CA At-risk pts Virulence Environment GNR +++ Multiple Multiple HA & CA All +++ +/- MRSA + Single Single HA Unwell ++ + VRE + Single Single HA Unwell +/- ++
Background and epi Drivers of GNBSI Learning from G+ success? How to tackle GNBSI
Drivers of Gram-negative BSI Patient sampling Seasonal variation Lab testing Deprivation Humans Animals Devices Sources Food Hydration & UTI Acquisition Soil AMR Patient factors Hands Transmission routes Environment Surgery & wounds High risk patients
Trends in classification of E. coli BSIs Classification and trends of E. coli BSIs in Oxfordshire, England. Vihta et al. Lancet Infectious Dis 2018.
Getting to grips with the source of E. coli BSIs Comparing the source of 250 healthcare-associated E. coli BSIs with the national picture, 2015-2017. Otter et al. J Hosp Infect 2018.
Seasonal variation in E. coli BSIs The monthly rate of 2810 E. coli BSIs in a region of Israel plotted against ambient temperature. Chazan et al. Clinical Microbiol Infect 2011.
Social and material deprivation We performed a risk factor analysis, which included both individual-level variables (such as overseas travel, antibiotic exposure, and age) and were also able to include community-level variables (such as markers of household overcrowding, deprivation, immigration, and ethnicity). We found that risk factors for ESBL were travel to Asia (OR 4.4, CI 2.5-7.6), or Africa (OR 2.4, CI 1.2-4.8) in the 12 months prior to admission, two or more courses of antibiotics in the 6 months prior to admission (OR 2.0, CI 1.3-3.0), and residence in a district with a higher than average prevalence of overcrowded households (OR 1.5, CI 1.05-2.2). The global prevalence of ESBL in the community, from Woerther et al. Otter et al. Clinical Microbiol Infect 2019.
Background and epi Drivers of GNBSI Learning from G+ success? How to tackle GNBSI
MRSA bacteraemia, England 2001-2013 2,500 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Revised national guidelines, 2006 11. Deep clean, 2007 12. Screening elective admissions, 2008 13. Universal screening, 2010 Mandatory reporting, 2001 Getting ahead of the curve , 2002 Winning ways , 2003 Towards cleaner hospitals , 2004 Cleanyourhands , 2004 Targets introduced, 2004 Cleanliness improvement, 2005 Going further faster , 2006 Root cause analysis, 2006 4 5 6 8 9 10 3 7 1 2 2,000 Number of MRSA bacteraemias 11 1,500 12 1,000 13 All cases 500 Trust apportioned 0 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
CDI cases, 2004-2013 C. difficile infection (CDI), England 2004-2013 3 18,000 1. National Antimicrobial Stewardship Group (ASG) formed in England, 2003 Mandatory reporting, 2004 Targets, 2007 Revised national guidelines, 2009 Start Smart Then Focus lauchned ESPAUR formed 2. 3. 4. 5. 6. 16,000 14,000 C. difficile infection (CDI)I cases 1 2 12,000 10,000 4 8,000 5 6,000 All cases 6 Trust apportioned 4,000 2,000 0 Q2 Q1 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Does hand hygiene explain the reductions? The Cleanyourhands campaign was associated with sustained increases in hospital procurement of alcohol rub and soap, which the results suggest has an important role in reducing rates of some healthcare associated infections. Stone et al. BMJ 2012;344:e3005.
Does antimicrobial stewardship explain the reduction? Dingle et al. Lancet Infect Dis 2017 in press.
Spurious correlation? Correlation between national chocolate consumption and rate of Nobel prize winners. Messerli FH. New Engl J Med 2012;367:1562-4.
Spurious correlations http://www.tylervigen.com/spurious-correlations
Spurious correlations http://www.tylervigen.com/spurious-correlations
Spurious correlations http://www.tylervigen.com/spurious-correlations
Whats driving increases in MSSA and E. coli BSI? 18,000 3500 C. difficile - all cases E. coli BSI - all cases MRSA BSI - all cases MSSA BSI - all cases C. difficile - Trust-apportioned E. coli BSI - Trust-apportioned MRSA BSI - Trust-apportioned MSSA BSI - Trust-apportioned Number of cases (C. difficile infection and E. coli BSI) 16,000 Number of cases (MRSA BSI, MSSA BSI) 3000 14,000 2500 12,000 2000 10,000 8,000 1500 6,000 1000 4,000 500 2,000 -00 0 Apr-Jun 2015 Oct-Dec 2007 Apr-Jun 2007 Apr-Jun 2008 Oct-Dec 2008 Apr-Jun 2009 Oct-Dec 2009 Apr-Jun 2010 Oct-Dec 2010 Apr-Jun 2011 Oct-Dec 2011 Apr-Jun 2012 Oct-Dec 2012 Apr-Jun 2013 Oct-Dec 2013 Apr-Jun 2014 Oct-Dec 2014 Jan-Mar 2015 Oct-Dec 2015 Apr-Jun 2016 Oct-Dec 2016 Apr-Jun 2017 Oct-Dec 2017 Jul-Sept 2007 Jul-Sept 2008 Jul-Sept 2009 Jul-Sept 2010 Jul-Sept 2011 Jul-Sept 2012 Jul-Sept 2013 Jul-Sept 2014 Jul-Sept 2015 Jul-Sept 2016 Jul-Sept 2017 Jan-Mar 2008 Jan-Mar 2009 Jan-Mar 2010 Jan-Mar 2011 Jan-Mar 2012 Jan-Mar 2013 Jan-Mar 2014 Jan-Mar 2016 Jan-Mar 2017 Jan-Mar 2018
Why antibiotic susceptible bacteria are resistant to hospital- based IPC intervention Mathematical model to investigate transmission in hospitals and their surrounding catchment area. Included a competitive advantage for resistant bacteria in hospitals and sensitive bacteria in the community. Modelling the impact of improving hand hygiene by 10%. Antibiotic-resistant bacteria were disproportionately affected in hospitals! van Kleef et al. BMC Infect Dis 2013;13:294.
Why antibiotic susceptible bacteria are resistant to hospital- based IPC intervention 3500 MRSA BSI - all cases MRSA BSI - Trust-apportioned MSSA BSI - all cases MSSA BSI - Trust-apportioned 3000 Number of cases 2500 2000 1500 1000 500 0 Oct-Dec 2007 Oct-Dec 2008 Oct-Dec 2009 Oct-Dec 2010 Oct-Dec 2011 Oct-Dec 2012 Oct-Dec 2013 Oct-Dec 2014 Oct-Dec 2015 Oct-Dec 2016 Oct-Dec 2017 Jul-Sept 2007 Jan-Mar 2008 Jul-Sept 2008 Jan-Mar 2009 Jul-Sept 2009 Jan-Mar 2010 Jul-Sept 2010 Jan-Mar 2011 Jul-Sept 2011 Jan-Mar 2012 Jul-Sept 2012 Jan-Mar 2013 Jul-Sept 2013 Jan-Mar 2014 Jul-Sept 2014 Jan-Mar 2015 Jul-Sept 2015 Jan-Mar 2016 Jul-Sept 2016 Jan-Mar 2017 Jul-Sept 2017 Jan-Mar 2018 Apr-Jun 2007 Apr-Jun 2008 Apr-Jun 2009 Apr-Jun 2010 Apr-Jun 2011 Apr-Jun 2012 Apr-Jun 2013 Apr-Jun 2014 Apr-Jun 2015 Apr-Jun 2016 Apr-Jun 2017 van Kleef et al. BMC Infect Dis 2013;13:294.
MRSA bacteraemia, England 2001-2013 2,500 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Revised national guidelines, 2006 11. Deep clean, 2007 12. Screening elective admissions, 2008 13. Universal screening, 2010 Mandatory reporting, 2001 Getting ahead of the curve , 2002 Winning ways , 2003 Towards cleaner hospitals , 2004 Cleanyourhands , 2004 Targets introduced, 2004 Cleanliness improvement, 2005 Going further faster , 2006 Root cause analysis, 2006 4 5 6 8 9 10 3 7 1 2 2,000 Number of MRSA bacteraemias 11 1,500 12 1,000 13 All cases 500 Trust apportioned 0 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Targeted approach to MRSA infection prevention Reduction targets introduced in 2004 and reinforced in 2006 High impact interventions launched in 2006 Root cause analysis launched in 2006 Revised national guidelines launched in 2006 (including screening, isolation, and suppression for carriers)
Going further faster (2006) Key challenge Specific Focus Challenge 1 Engage the board and use performance management at every level Challenge 2 Challenge 3 Challenge 4 Challenge 5 Ensure clinical ownership across organisation Screen and/or decontaminate according to risk assessment Use HIIs* to monitor and increase compliance Integrate with risk and clinical governance framework Challenge 6 Ensure infection control is part of induction and ongoing training Challenge 7 Effectively coordinate bed management with infection control input Challenge 8 Clean and decontaminate Proactively manage your reputation, engage all staff and local community Challenge 9 * HII = high impact interventions: Central venous catheter care bundle; Peripheral intravenous cannula care bundle; Renal catheter care bundle; Care bundle to prevent surgical site infection; Care bundle for ventilated patients; Urinary catheter care bundle; Care bundle to reduce the risk from Clostridium difficile. From Going further faster
Background and epi Drivers of GNBSI Learning from G+ success? How to tackle GNBSI
Drivers of Gram-negative BSI Patient sampling Seasonal variation Lab testing Deprivation Humans Animals Devices Sources Food Hydration & UTI Acquisition Soil AMR Patient factors Hands Transmission routes Environment Surgery & wounds High risk patients
Getting to grips with the source of E. coli BSIs Comparing the source of 250 healthcare-associated E. coli BSIs with the national picture, 2015-2017. Otter et al. J Hosp Infect 2018.
Youre givin me good hydration Simple interventions (e.g. offering people a drink and giving them a choice of fluids) made a big impact on hydration levels (Wilson, Clin Nutr, 2019)
Prevent preventable SSIs % patients with SSI following cardiothoracic surgery. Chiwera et al. J Hosp Infect 2018.
Transmission modes of Gram-negative bacteria Otter et al. Infect Control Hosp Epidemiol 2011;32:687-699.
Contaminated sinks / drains CPE (K. pneumoniae) acquisition and clinical infection halved through improved management of sinks (OR = 0.51 for acquisions, and 0.29 for clinical cultures) (n=~7,500 pts). Mathers et al. Clin Infect Dis 2018 in press.
Transmissibility / fitness Klebsiella species 3.7x more transmissible than E. coli in the ICU.1 K. pneumoniae seems to be more environmental than E. coli.2,3 Conclusion Surface contamination on five standardized sites surrounding patients infected or colonized with ESBL-producing Klebsiella spp. (n=48) or ESBL-producing E. coli (n=46).2 35 p<0.001 30 % contaminated 25 Klebsiella spp. E. coli 20 15 p<0.001 10 5 0 Rooms contaminated Sites contaminated 1. Gurieva et al. Clin Infect Dis 2018;66:489-93. 2. Guet-Revillet et al. Am J Infect Control 2012;40:845-8. 3. Gbaguidi-Haore. Am J Infect Cont 2013;41:664-5.
Background and epi Drivers of GNBSI Learning from G+ success? How to tackle GNBSI
Getting to grips with healthcare- associated Gram-negative bloodstream infection? Jon Otter, PhD FRCPath Imperial College London j.otter@imperial.ac.uk @jonotter Blog: www.ReflectionsIPC.com

































")