Pediatric Surgical Problems Overview
A three-day-old infant presenting with not passing meconium, abdominal distension, lethargy, decreased feeding, and jaundice is evaluated for possible pediatric surgical issues. Conditions such as duodenal atresia, imperforate anus, and intussusception are discussed along with their diagnostic and management approaches. Images illustrate the anatomical variations and clinical presentations associated with these pediatric surgical problems.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Some Pediatric surgical problems Three days old NN brought to the hospital by caregiver C/O not passing meconium , but passing urine normally .The condition is associated with abdominal distension, lethargy , decreased feeding & appearance of jaundice ,the pregnancy is uneventful, apart from some polyhydramnios .on Exam. there is abdominal distension and decreased primitive reflexes , no dysmorphic features but jaundiced.
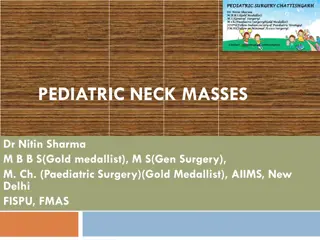
Some GIT surgical problems Duodenal atresia The incidence of duodenal atresia is 1 in 10,000, and accounts for 60% of intestinal atresias. Detected at antenatal sonography in ~ 50% of cases double bubble &polyhydramnios. .Postnatally, vomiting occurs in the first 48 hrs & is bilious if the obstruction is distal to the ampulla of Vater (two- thirds of cases), or non- bilious if the obstruction is proximal. NG decompression & IV fluid resuscitation. Surgery is usually not an emergency. SurgeryDuodeno- duodenostomy (laparoscopic or open). The proximal &distal duodenal pouches are opened and joined bypassing the atretic segment. Placement of a trans- anastomotic (nasojejunal) tube allows early enteral feeding, and avoids the need for long line/ parenteral nutrition. Long- term outcome : duodenoplasty is required if severe proximal dilatation occur
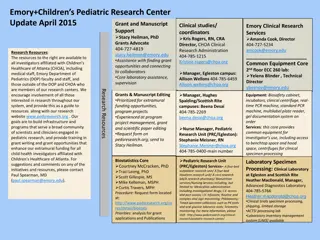
Imperforate anus in females. A, Vestibular fistula. B, Cloaca. (From Pea A: Atlas of surgical management of anorectal malformations , New York, 1989, Springer- Verlag, pp 50, 60.) Anatomy of the anal canal. (Adapted from Brunicardi FC, Anderson DK, Billar TR, et al: Schwartz's principles of surgery , ed 8, New York, 2004, McGraw-Hill.)
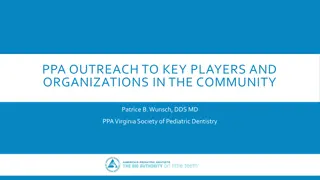
Imperforate anus in males. A, Low lesions. B, High lesions. (From Pea A: Atlas of surgical management of anorectal malformations , New York, 1989, Springer-Verlag, pp 7, 26.)
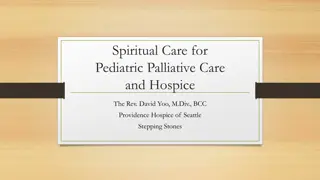
Intussusception occurs when a portion of the alimentary tract is telescoped into an adjacent segment. 5 mo & 3 yr of age ~ 90% of cases of intussusception in children are idiopathic. 2 8% of pts, recognizable lead points for the intussusception are found, such as a Meckel diverticulum, intestinal polyp, neurofibroma, intestinal duplication cysts, inverted appendix stump, leiomyomas, hamartomas, ectopic pancreatic tissue, anastomotic suture line, enterostomy tube, posttransplant lymphoproliferative disease, hemangioma, or malignant conditions such as lymphoma sudden onset, in a previously well child, of severe paroxysmal colicky pain that recurs at frequent intervals and is accompanied by straining efforts with legs and knees flexed and loud cries clinical history and physical findings suggest intussusception, an ultrasound is typically performed Intussusception in an infant. The obstruction is evident in the proximal transverse colon. Contrast material between the intussusceptum and the intussuscipiens (arrows) is responsible for the coiled-spring appearance.
Hirschsprung disease HD is congenital aganglionosis of the distal colon, extending proximally from the rectum. HD usually affects the recto- sigmoid only (short- segment). In 25% of cases, aganglionosis extends more proximally, total colonic aganglionosis occurs in 10%. Classic triad is of neonatal bilious vomiting, abdominal distension, & delayed passage of meconium (>48 hours). Diagnosis Suction rectal biopsy can be performed in the neonate without general an-aesthesia (GA); open biopsy under GA is required in older infants/ children. Dx is confirmed by histological confirmation of absent ganglion cells (H&E stain) and hypertrophic nerve trunks on acetylcholinesterase staining. Calretinin staining (absent in HD) may be supportive. Contrast enema may demonstrate a transition zone, Surgical treatment is excision of the aganglionic segment and colo- anal anastomosis (pull- through) of proximal normally innervated colon. Initial management is directed at nasogastric decompression, rectal washouts (up to three times per day, retained volume should be <20mL/ kg saline)
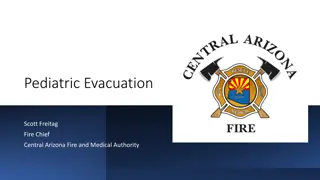
Non-bilious vomiting is the initial symptom of pyloric stenosis starts after 3 wk of age, but symptoms can develop as early as the first wk of life and as late as the 5th mo Hypochloremic metabolic alkalosis . Unconjugated hyperbilirubinemia is more common than conjugated and usually resolves with surgical correction Dx by palpating the pyloric mass. firm, movable, approximately 2 cm in length, olive shaped, hard, best palpated from the left side, and located above and to the right of the umbilicus in the mid epigastrium beneath the liver's edge. Ultrasound examination confirms the Dx Treatment 1-Supportive 2-Surgery Gastric peristaltic wave in an infant with PS
Esophageal atresia usually associated with a tracheoesophageal fistula
Learning objectives: *Select patients with abdominal pain who require emergency Select patients with abdominal pain who require emergency Tx Tx. . *Show clinical findings which are key to instituting the most likely source of the *Show clinical findings which are key to instituting the most likely source of the pain pain. *Distinguish acute from chronic pain & organic from functional *Distinguish acute from chronic pain & organic from functional *Understand the abdominal x *Understand the abdominal x- -rays rays *Perform an effective plan of *Perform an effective plan of Mx Mx for a pt with AP for a pt with AP *Define which pts have significant liver dysfunction & its cause *Define which pts have significant liver dysfunction & its cause *Distinguish between the causes of jaundice . *Distinguish between the causes of jaundice . *immunization status, past & *immunization status, past & FHx FHx. . *Discuss abnormal LFT in the setting of the clinical presentation, & choice pts *Discuss abnormal LFT in the setting of the clinical presentation, & choice pts needing medical needing medical Mx Mx. . *Outline the epidemiology & natural *Outline the epidemiology & natural Hx Hx of viral hepatitis * *Select & interpret an appropriate investigations for pts with jaundice (e.g., liver enzymes Select & interpret an appropriate investigations for pts with jaundice (e.g., liver enzymes. *List the indications for an abdominal U *List the indications for an abdominal U\ \S, spiral CT, MRI, ERCP& PTC S, spiral CT, MRI, ERCP& PTC. *Outline a *Outline a Mx Mx plan for pts with acute hepatic failure plan for pts with acute hepatic failure. of viral hepatitis
References: References: 1.Nelson textbook of Pediatrics last edition 1.Nelson textbook of Pediatrics last edition 2.Illustrated textbook of 2.Illustrated textbook of Paediatrics 3.Internet educational websites 3.Internet educational websites Paediatrics Last edition Last edition THANKS THANKS