Understanding Biliary Disorders and Gallbladder Dysfunction

This informative content delves into the anatomy and function of the gallbladder, discussing its role in storing and concentrating bile. It explains the composition of bile, the process of emulsifying fats, and the consequences of bile flow obstruction. Various disorders affecting the biliary system, such as cholecystitis and gallstones, are explored in detail, highlighting symptoms and complications. Additionally, acalculous cholecystitis is discussed, shedding light on potential causes and manifestations.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Biliary Disorders Gallbladder and Pancreatic Dysfunction
Anatomy and function of gallbladder It is a pear shaped hollow organ 3-4 inches long. It lies in a shallow depression on the under surface of the liver. It can hold up to 30-50cc of bile. It is connected to the common bile duct by the cystic duct. Function: storage depot. It also concentrates bile, see page 1125. When food enters the duodenum, the gallbladder contracts and the sphincter of Oddi relaxes. This allows bile to enter the intestine. It is mediated by secretion of the cholecystokinin-pancreaozymin from the intestinal wall. Morphine sulfate causes the sphincter of Oddi to contract.
Bile Bile is composed of water and electrolytes and amts of lecithin, fatty acids, cholesterol, bilirubin, and bile salts. The salts and cholesterol assist in the emulsification of fats in the distal ileum. They are then reabsorbed into the portal blood for return to the liver and again excreted into the bile. This pathway from hepatocytes to bile to intestine and back is called enterohepatic circulation.
If the flow of bile is impeded with stones in the bile ducts then bilirubin a pigment derived from the breakdown of RBCs does not enter the intestine. As a result bilirubin in the blood increases. This results in increased renal excretion of urobiliogen, which results from conversion of bilirubin in the small intestine and decreased excretion in the stool.
Disorders of the gallbladder Several disorders affect the biliary system and interfere with normal drainage of bile into the duodenum. 1.Inflammation(cholecystitis) of biliary system, 2.cancer which obstructs the biliary tree. 3. gallstones(cholelithiasis)
A close look Cholecystitis: acute inflammation of gallbladder. S/S pain, tenderness, and rigidity in the upper right abdomen that may radiate to the midsternal area or right shoulder and is associated with nausea, and vomiting. Calculous cholecystitis: is the cause of 90% acute chole. A stone obstructs bile outflow. The bile remaining in the gallbladder initiates a chemical reaction: autolysis and edema occur, and the blood vessels are compressed, compromising the vascular system. Gangrene of gallbladder can occur and infection in 60% of pts. As well as perforation of the gallbladder.
Acalculous chole: describes acute gallbladder inflammation without gallstones. It occurs after major surgical procedures, trauma, or burns. Also torsion, cystic duct obstruction, primary bacterial infections, and multiple blood transfusions. It is speculated that this condition can come from F&E alterations and in regional blood flow in the visceral circulation. Bile stasis and increased thickness(viscosity) of bile are thought to play a role.
Risk factors The 3 Fs: fair, fat and 40 or over was usually the description of a person with gallstones or gallbladder inflammation. Adults over 40 and 50% of those over 70 and 80 will develop stones. Obesity, women with multiple pregnancies, rapid wgt loss, frequent changes in wgt, high and low dose estrogen therapy, ileal resection or disease, cystic fibrosis, and diabetes are further risk factors.
Signs and symptoms acute or chronic Epigastric distress, such as fullness, abdominal distention, vague pain in right upper quadrant of the abdomen, especially after a meal rich in fried or fatty foods. Pain-if a stone obstructs the cystic duct , the GB becomes distended, inflamed and eventually infected. They may develop fever. The patient with biliary colic can have severe upper right abd pain that radiates to the back or right shoulder, it is associated with nausea and vomiting, and can occur several hours after a heavy meal. When the bile cannot be released due to obstruction the GB distends and comes in contact with the abdominal wall in the region of the 9thand 10thcostal cartilages. This produces tenderness in the RUQ on deep inspiration and prevents full inspiratory excursion.
S/S contd Jaundice- not all patients have jaundice, only when the bilirubin is absorbed in the blood. It is also associated with itching. Changes in urine and stool color- urine is dark, and stools are clay colored
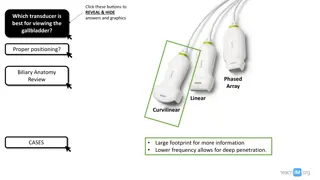
Assessment and diagnostic findings Abdominal x-ray Ultrasound Radionuclide imaging Cholecystography Endoscopic retrograde cholangiopacreatography(ERCP) Percutaneous transhepatic cholangiography
Medical management The aim is to reduce the incidence of acute episodes of pain by diet, and remove the cause by drug therapy, endoscopic or surgery methods.Most non surgical approaches including lithotripsy and dissolution of gallstones are only temporary solutions. Approx 80% of patients with acute GB inflammation achieve results with rest, I.V. fluids, nasogastric suction, analgesia, and antibiotic agents. Unless the patient s condition deteriorates, surgical intervention is delayed until the acute phase is over.
Medical management contd The diet following an exacerbation of GB inflammation is low fat liquids. Can stir protein supplement into skim milk. Cooked fruits, tapioca, mashed potatoes, non- gas forming veggies and bread, tea and coffee can be added. Food to avoid are eggs, cheese, fried foods, gas forming veggies and alcohol.
Conservative therapy There are also medications such as UDCA Ursodeoxycholic acid which can dissolve stones consisting of cholesterol over 6-12 months of therapy. There is also an infusion which can dissolve stones, not widely used, also is stone removal by ERCP as well as lithotripsy. This form uses shock wave therapy to fragment stones so that they can be passed or dissolved by the body.
Surgical management Removal of gallbladder is a cholecystectomy- this has been the approach for many years. The most recent approach is the lap chole which inserts a laproscope into the umbilicus and 3-4 other stab wounds in the abdomen and drains the GB and removes it via the tubes. The patient goes home within a day or two and can return to work in 1 week.
Surgical contd Percutaneous chole-under local anesthesia, a fine needle is inserted into the gallbladder using tomography. Bile is aspirated and then a catheter is inserted to decompress the biliary tract. Almost immediate pain is relieved and sepsis is resolved.antibiotics are also given before, during and after this procedure.
T-Tube placement If a T-Tube is placed in the common bile duct, it is inserted because of retained stones.
The Pancreas The pancreas is located in the RUQ. It has exocrine and endocrine functions. The secretion of enzymes into the GI tract through the pancreatic duct represents exocrine function. The secretion of insulin, glucagon, and somatostatin into the bloodstream represents its endocrine function.
The exocrine function The secretions of the exocrine portion of the pancreas are collected in the pancreatic duct, which joins the common bile duct and enters the duodenum at the ampulla of Vater. Surrounding the ampulla is the sphincter of Oddi, which partially controls the rate at which secretions from the pancreas and gallbladder enter the duodenum.
Exocrine contd The secretions are digestive enzymes high in protein content and electrolyte rich fluid. They are alkaline b/c they contain high concentrations of bicarbonate and are capable of neutralizing the highly gastric acid juice that enters the duodenum. Amylase- CHO Trypsin-proteins Lipase-fats
Endocrine function The islets of Langerhans have alpha, beta, and delta cells. The alpha cells secrete glucagon, the beta secrete insulin and delta secrete somatostatin. Insulin permits entry of glucose into the cell Glucagon converts glycogen to glucose in the liver. Somatostatin exerts a hypoglycemic effect by interfering with release of growth hormone from the pituitary and glucagon from pancreas to raise blood glucose.
Disorders of pancreas Pancreatitis is a serious disorder. It is described as autodigestion of the pancreas. It is believed that the pancreatic duct becomes obstructed accompanied by hypersecretion of the exocrine enzymes. They enter the bile duct where they are activated and together with bile reflux into the pancreatic duct, causing pancreatitis.
Acute pancreatitis This can range from mild and self limiting to a fatal disease that does not respond to any treatment. Mild is characterized by edema confined to the pancreas, minimal organ dysfunction is present and return to normal in 6 months. The pt is still at risk for hypovolemic shock, f&e disturbances and sepsis. A more widespread type is where the tissue becomes necrotic, and the damage extends to the retroperitoneal tissues. Systemic complications such as acute respiratory distress syndrome, shock, DIC, and pleural effusion can increase mortality rate to 50%.
Etiology 80% of patients have biliary disease, however only 5% of patients have gallstones. If anything obstructs the flow of pancreatic enzymes or causes reflux of bile into the pancreatic duct, it activates powerful enzymes. This activation can lead to necrosis, vasodilation, increased vascular permeability, erosion, and hemorrhage.
Etiology contd Long term use of alcohol is commonly associated with acute pancreatitis, however, the patient usually has had undiagnosed chronic pancreatitis before the first episode of acute occurs. Other less common causes are viral, bacterial, mumps. Spasm and edema of ampulla of Vater, resulting from duodenitis, blunt trauma, peptic ulcer disease, ischemic vascular disease, hyperlipidemia, hypercalcemia, use of steroids, thiazide diuretics, and oral contraceptives. Also after some surgeries and a small incidence of hereditary.
Signs and Symptoms The patient is severely ill with severe abdominal pain and back pain. Pain may be accompanied by abdominal distention, a poorly defined palpable mass and decreased peristalsis. This pain is also accompanied by vomiting that does not relieve the pain or nausea.
Signs and Symptoms contd Acutely ill Rigid abdomen if peritonitis or soft in the absence of peritonitis Bruising or ecchymosis in the flank or umbilicus Nausea, vomiting, fever, jaundice, mental confusion or agitation may occur.
More severe s/s Hypotension due to hypovolemia and shock, tachycardia, cyanosis and cold clammy skin due to large amts of protein rich fluids into the peritoneal cavity and tissues. Respiratory distress and hypoxia are common, pulmonary infiltrates, dyspnea, tachypnea and abn gas values also. Myocardial depression, hypocalcemia, hyperglycemia and DIC may occur.
Medical management NPO Nasogastric tube, I.V. therapy,(TPN) Histamine 2 antagonists, pain management with Demerol not Morphine( which may cause spasms of the sphincter of Oddi) Anitemetic agents such as Phenergan Correction of fluid and blood loss and low albumin levels is necessary to maintain fluid volume and prevent renal failure. Antibiotics Insulin
Surgical management Usually is not done while the patient is acutely ill and if the patient recovers from medical management. The only reasons for surgery are: diagnostic lap, to establish pancreatic drainage, or to resect or debride a necrotic pancreas.
Creative Commons License This work is licensed under a Creative Commons Attribution 4.0 International License. Except where otherwise noted, this content by Southern Regional Technical College is licensed under the Creative Commons Attribution 4.0 International License. To view a copy of this license, click https://creativecommons.org/licenses/by/4.0/ Healthcare Careers Work!(HCW) is sponsored by a $2.3 million grant from the U.S. Department of Labor, Employment & Training Administration. TAACCCT Grant #TC- 26488-14-60-A-13. Southern Regional Technical College is an equal opportunity employer and will make adaptive equipment available to persons with disabilities upon request. This workforce product was funded by a grant awarded by the U.S. Department of Labor s Employment and Training Administration. The product was created by the grantee and does not necessarily reflect the official position of the U.S. Department of Labor. The U.S. Department of Labor makes no guarantees, warranties, or assurances of any kind, express or implied, with respect to such information, including any information on linked sites and including, but not limited to, accuracy of the information or its completeness, timeliness, usefulness, adequacy, continued availability, or ownership.