Comparing Health Promotion Strategies: CLTS vs. CHC Approaches in Disease Prevention
The comparison between CLTS and CHC approaches in health promotion strategies reveals contrasting implementation methods and outcomes in disease prevention. The CHC model emphasizes holistic health issues and sustained behavior change through weekly meetings and group decision-making, while the CLTS approach focuses on triggering action through community intervention. Observations in Zimbabwe indicate significant differences in sanitation and hygiene indicators between CLTS and CHC villages. Recommendations suggest integrating both approaches for optimal results.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Best Practice in Health Promotion UNC Conference 2012 Juliet Waterkeyn
Comparing Health Promotion Strategies Focus Disease # Messages % ChangeCountry Type Narrow Diarrhoea 17 5.6 % Uganda 1.PHAST 2. Social Marketing Narrow Diarrhoea 4 13 % Burkina Faso 3. CLTS Narrow Diarrhoea 1 33% triggered Nigeria 4.CHC Approach Holistic Diarrhoea 1. Palmer (WSP-World Bank) (2005) 2.Cave & Curtis, 2002. 3. WaterAid , 2010. 4. Waterkeyn & Cairncross, 2005 17 47% Zimbabwe Skin disease Eye Disease Worms ARIs HIV/AIDS Malaria / Bilharzia
CURRENT DEBATE BETWEEN TWO MAIN APPROACHES CLTS Approach Implementation strategy One Triggering day + a few follow-up visits CHC Approach: Implementation strategy 6 months Hygiene sessions 20 sessions (each week) Learning through fun participatory activities reinforce good practice (song, drama) Village walk to shock community that they are eating their own faeces Community shamed into action Leaders enforce change with fines Informed group decision making and weekly homework Voluntary household improvements Zero Open Defecation (ZOD) & 20+ other hygiene improvements Open Defecation Free (ODF ) Village free ODF zone
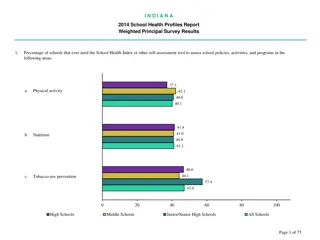
Observed Indicators of Sanitation and Hygiene between CLTS and CHC villages in Zimbabwe 100 90 80 70 60 50 40 30 20 10 0 No open faecal disposal Latrine present % built since intervention Hand washing facility present % CHC % CLTS p<0.001 2011.Whaley & Webster
CHC Model assumes Hygiene Behaviour Change is most successful when: Holistic: covers ALL local health issues and preventable diseases, not just diarrhoea Builds capacity with the same group for at least 6 months Reinforces health messages at a regular forum (weekly meetings) for problem solving Group decisions rather than individual risk taking Positive Peer Pressure to conform to group consensus
HOWEVER the best results were found in areas where there were CHCs and CLTS: Recommendations Revitalise / Evolve CLTS CHCs should be started in areas where there is already or where there will be CLTS CLTS Triggering is one of the 20 sessions in the CHC curriculum