Understanding Heterogeneity in Hypophosphatasia: A Case Study in Phenotypic Variability

This case study explores the diverse expression of hypophosphatasia in a Caucasian female patient, highlighting the challenges in diagnosis and treatment. The patient presented with chronic pain, fractures, myopathy, and dental issues, underscoring the complexity of genotype-phenotype correlations in this rare genetic disorder. Genetic mutations, enzyme activity, and environmental factors all play crucial roles in shaping the clinical manifestation of the disease.
- Hypophosphatasia
- Phenotypic Variability
- Genotype-Phenotype Correlations
- Rare Genetic Disorder
- Case Study

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Firenze 10-12 Dicembre 2015 L IPOFOSFATASIA: ETEROGENEITA NELL ESPRESSIONE DI MALATTIA Francesco Conti
Disclosures Speaker and/or consultant fees and/or research support from : Alexion, Amgen 2
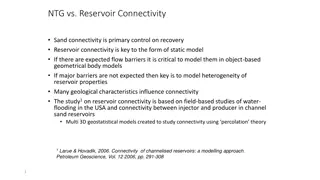
Possible explanation for phenotypic variability allelic heterogeneity in the TNSALP gene with 300 different mutations described (http://www.sesep.uvsq.fr/03_hypo_mutations.php) inheritance mechanism and age of onset mutation effect on the protein structure: 3D structure modeling and in vitro mutagenesis experiments to study the residual enzymatic activity good correlation between severity of the disease and genotype not always reported possible in vivo interference from other factors: modifier genes of alkaline phosphatase activity or phosphate metabolism epigenetic and environmental factors Studying the biochemical and clinical impact of ALPL gene mutations in large kindred might help to better understand genotype-phenotype correlations in hypophosphatasia.
Proposita - index patient Medical history: Caucasian, female, 47 yrs at presentation Patient complained of pelvic and ankle pain in the previous 2-3 years, resistant to analgesic and anti-inflammatory drugs
Proposita - index patient Medical history: At age of 47, on further radiographic examination, the pseudofracture of the lateral cortex of the right proximal femur was diagnosed (which likely occurred 1 year before) Patient was started on clodronate Low levels of ALP were unnoticed
Proposita - index patient Medical history: Patient was referred to our bone clinic in January 2008, because the femoral fracture did not heal Was still taking clodronate upon referral Persistent pain in the pelvis and femurs Other clinical features: Dental problems : early deciduous and permanent tooth loss Metatarsal stress fractures at age 35-40 Myopathy (pain and reduced strength and endurance) Recurrent acute inflammation of tendons with fluid retention (enthesopathy)
Proposita - index patient IV and V left metatarsal bone fractures bilateral proximal femoral pseudofractures of lateral cortical bone
Twin sister of the index patient Medical history: Caucasian, female, 48 yrs at presentation, referred from the sister Patient complained of pelvic and ankle pain in the previous 2-3 years, resistant to analgesic and anti-inflammatory drugs Other clinical features: Dental problems: early deciduous and permanent tooth loss Metatarsal stress fractures at age 35-40 Myopathy (pain and reduced strength and endurance) Recurrent acute inflammation of tendons with fluid retention (enthesopathy) Not aware of any other fractures Never on bisphosphonates
Twin sister of the index patient bilateral proximal femoral pseudofractures of lateral cortical bone at presentation the AP X-ray of pelvis showing calcific enthesitis (4 years later)
Brother of the index patient Medical history: Caucasian, male, 43 yrs at presentation, referred from the sister At approximately age 35, the patient suffered a left femoral fracture following minimal trauma, treated with intramedullary rod insertion for delayed healing He had also suffered from pain in the right ankle and femur in the last two years. Other clinical features: Dental problems: early deciduous and permanent tooth loss Metatarsal stress fractures at age 30-35 Myopathy (pain and reduced strength and endurance) Recurrent acute inflammation of tendons with fluid retention (enthesopathy) Never on bisphosphonates
Brother of the index patient A B bilateral proximal femoral pseudofractures of lateral cortical bone at presentation fracture of the left ulna following a minimal trauma (A after rod insertion; B at 6 mo) 11
Diagnosis of HPP DIAGNOSIS OF HPP AND/OR 1. Whyte, M. (2012); 2. Beck, C. (2011); 3. Barvencik, F. (2011); 4. Whyte, M. (2012, May); 5. Coe, J. (1986); 6. Whyte, M. (2012); 7. Chuck, A. J. (1989); 8. Sutton, R. (2012); 9. Collmann, H. (2009); 10. Rockman-Greenberg, C. (2013); 11. Whyte, M. (1982); 12. Reibel A. (2009); 13. Seshia, S. (1990); 14. Mohn, A. (2011); 15. Fallon, M. (1985); 16. Baumgartner-Sigl S. (2007); 17. Balasubramaniam, S. (2010); 18. Silver, M. (1988); 19. Mornet, E. (1993); 20. Whyte, M. (2001); 21. Whyte, M. (1985)
ALP Activity by age and gender Low End of Normal Range by age and gender ALP Activity U/L
To confirm the diagnosis of HPP Low ALP activity bone ALP has a less important role (differs only by post-translational modifications) Elevated substrate levels Inorganic pyrophosphate (PPi) in urine and plasma Phosphoethanolamine (PEA) in urine Pyridoxal 5 -phosphate (PLP) in plasma [Vit. B6] Mutation analysis of TNSALP 300 mutations described 14
Biochemical findings in the three patients # 6 # 7 # 8 ALP (U/L) (n.r. 35-128) 17.3 23.4 14.2 Bone ALP ( g/L) (n.r. 6-26) 2.3 2.9 1.7 PLP ( g/L) (n.r. 8.7-27.2) 77.1 129.8 109.7 Calcium (mg/dl) (n.r. 8.4-10.2) 10.3 9.9 9.4 Phosphate (mg/dl) (n.r. 2.7-4.5) 4.68 5.46 5.33 Creatinine (mg/dl) (n.r. 0.7-1.25) 1.21 0.97 0.81 25-OH-Vit.D (ng/ml) (n.r. 30) 27.5 25.2 19.1 . Biochemical values are the average of 6-8 different determinations.
Bone Mineral Density (DXA Tscore) # 6 # 7 # 8 43 48 48 Age (yrs) BMD was measured at diagnosis. +2.9 +1.0 +3.3 Lumbar (L1-L4) Ts Subjects #7 and #8 : premenopausal. -1.1 -0.9 -0.4 Femoral neck Ts -1.0 -0.2 -0.7 Total hip Ts
Family pedigree based on ALP levels and skelatal phenotype 2# 2 # 1 1 9 7 # 7 8 # 8 # 4 # 3 # 6 # 9 3 # 3 4 5 6 20 21 22 23 24 25 26 14 15 16 # 16 17 # 17 10 11 12 13 # 18 # 19 Key table = normal ALP , = low ALP without HPP clinical phenotype , = low ALP with HPP clinical phenotype , 17
Family pedigree based on ALP levels and mutational analysis of TNSALP # 2 # 1 1 2 9 7 # 7 8 # 8 # 4 # 3 # 6 # 9 3 # 3 4 5 6 20 21 22 23 24 25 26 14 15 16 # 16 10 11 12 13 # 17 # 18 # 19 Key table = normal ALP , = low ALP without HPP clinical phenotype , = low ALP with HPP clinical phenotype , = single base mutation of TNSALP exon 12 18
Family pedigree based on ALP levels and mutational analysis of TNSALP # 2 # 1 1 2 9 7 # 7 8 # 8 # 4 # 3 # 6 # 9 3 # 3 4 5 6 20 21 22 23 24 25 26 14 15 16 # 16 10 11 12 13 # 17 # 18 # 19 Key table = normal ALP , = low ALP without HPP clinical phenotype , = low ALP with HPP clinical phenotype , = single base mutation of TNSALP exon 12 = single base mutation of TNSALP intron 8 19
Clinical characteristcs and biochemical values (serum ALP, plasma PLP) # 2 # 4 # 5 # 6 # 7 # 8 # 9 # 16 # 17 # 18 # 19 NO Mutation Age (diagn/scree) 78 56 34 43 48 48 52 20 25 20 15 Premature teeth loss No No No Yes Yes Yes No No No No No Metatarsal fractures No No No Yes Yes Yes No No No No No Femoral fractures Yes bilateral Yes bilateral Yes bilateral No No No No No No No No Other fractures Ulna Left Ulna Left No No No No No No No No No Nephro- calcinosis No No No No No No No No No No No Acute peri- articular pain + No No ++ +++ ++ No No No No No Muscle pain/ weakness No No No Yes Yes Yes No No No ** ** ALP (U/L) (n.r. 35-128) 30 34 53 17.3 23.4 14.2 44 42 30.3 26 25 PLP ( g/L) (n.r. 8,7-27,2) 28 18 19 77.1 129.8 109.7 21 19 19 26 23 20
Asfotase alfa Asfotase alfa is a bone-targeted, human recombinant TNSALP fusion protein Designed to replace enzyme activity at site of deficiency TNSALP Structure of asfotase alfa IgG1 Fc Deca-aspartate 21 1. Mill n JL et al, J Bone Miner Res 2008;23:777 787; 2. Data on file
Summary A classic form of adult HPP was diagnosed in three individuals of the same family. Unnoticed low ALP activity and lack of knowledge of the disease contributed to the late diagnosis Normal to high mineral densitometry was found in these patients The clinical phenotype in the three subjects was considerably homogeneous (skeletal, reumatologic and dental manifestations) and the natural history of disease appeared to be similar 5 subjects of the same family, showed ALP activity in the low range although did not show clinical manifestations of HPP Genetic analysis revealed the presence of two TNSALP mutations that co-segregated in the individuals presenting the clinical phenotype The patient showing the most severe phenotype has started asfotase alfa therapy 22
Acknowledgements M.P. Whyte, S Mumm (Shriners Hospital, Washington University, St.Louis, USA) F. Turturro, G. Argento, G. Gentile, L. Lionetto, G. Pugliese (Sant Andrea Hospital, Sapienza University, Rome, Italy) ML Brandi (Metabolic Bone Diseases Unit, Department of Surgery and Translational Medicine, University of Florence, Italy) 23















")