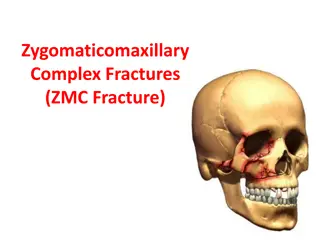
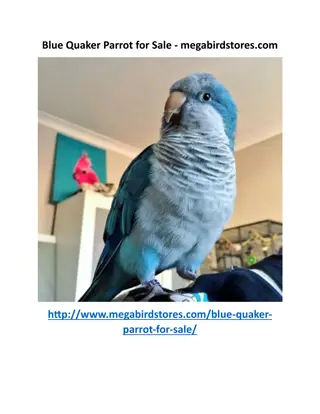
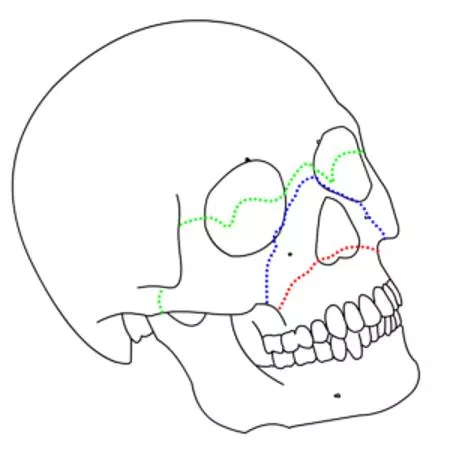
LeFort I (red), II (blue), and III (green) fractures
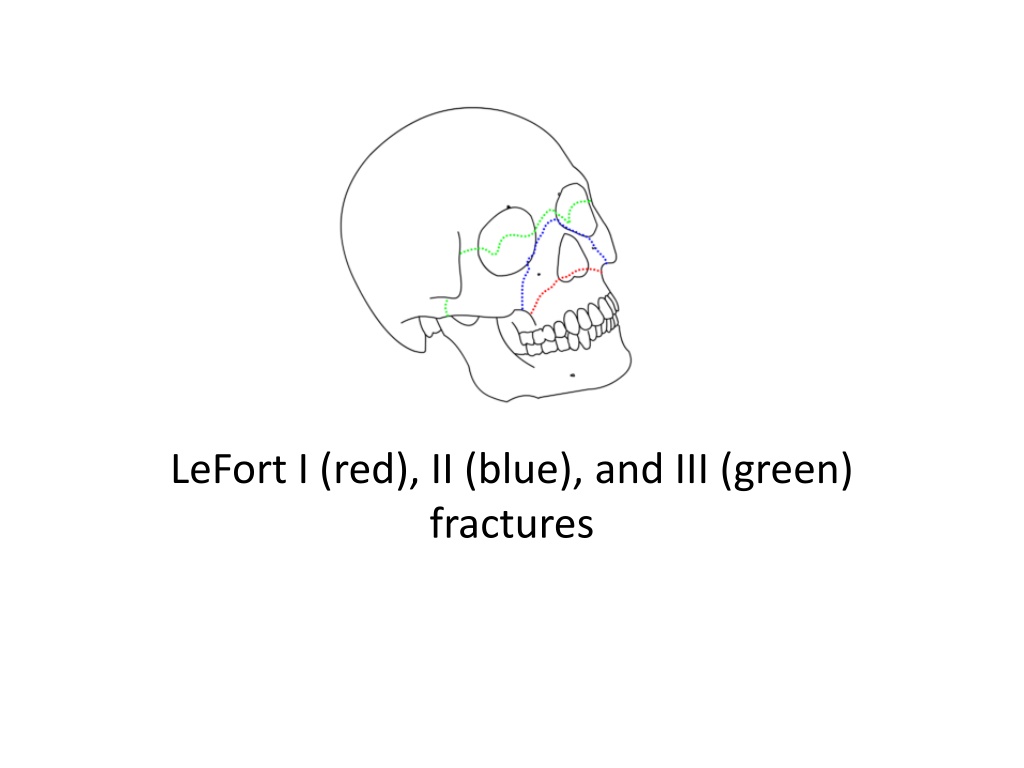

LeFort I (red), II (blue), and III (green)
fractures
Le Fort fracture of skull
•
From Wikipedia, the free encyclopedia
•
Jump to navigationJump to search
LeFort fractureLeFort I (red), II (blue),
and III (green) fracturesA
Le Fort fracture of the skull
is a classic
transfacial
fracture
of the midface, involving the
maxillary bone
and
surrounding structures in either a horizontal, pyramidal or transverse
direction. The hallmark of Lefort fractures is traumatic
pterygomaxillary
separation
, which signifies fractures between the
pterygoid plates
,
horseshoe shaped bony protuberances which extend from the inferior
margin of the
maxilla
, and the maxillary sinuses. Continuity of this
structure is a
keystone
for stability of the midface, involvement of which
impacts surgical management of trauma victims, as it requires fixation to a
horizontal bar of the
frontal bone
. The pterygoid plates lie posterior to the
upper dental row, or alveolar ridge, when viewing the face from an
anterior view. The fractures are named after French
surgeon
René Le
Fort
(1869–1951), who discovered the fracture patterns by examining
crush injuries in
cadavers
.
[1]
•
Signs and symptoms[
edit
]
•
Le Fort I
— Slight swelling of the upper lip,
ecchymosis
is present in the buccal
sulcus beneath each zygomatic arch, malocclusion, mobility of teeth. Impacted
type of fractures may be almost immobile and it is only by grasping the maxillary
teeth and applying a little firm pressure that a characteristic grate can be felt
which is diagnostic of the fracture. Percussion of upper teeth results in cracked pot
sound. Guérin's sign is present characterised by ecchymosis in the region of
greater palatine vessels.
•
Le Fort II
and
Le Fort III
(common) — Gross edema of soft tissue over the middle
third of the face, bilateral circumorbital ecchymosis, bilateral subconjunctival
hemorrhage, epistaxis, CSF rhinorrhoea, dish face deformity, diplopia,
enophthalmos, cracked pot sound.
•
Le Fort II
— Step deformity at infraorbital margin, mobile mid face, anesthesia or
paresthesia of cheek.
•
Le Fort III
— Tenderness and separation at frontozygomatic suture, lengthening of
face, depression of ocular levels (
enophthalmos
), hooding of eyes, and tilting of
occlusal plane, an imaginary curved plane between the edges of the incisors and
the tips of the posterior teeth. As a result, there is gagging on the side of injury.
[
•
Diagnosis[
edit
]
•
A 3-D CT reconstruction showing a LeFort type 1 fracture ( fracture line is marked by an arrow )
•
Diagnosis is suspected by physical exam and history, in which, classically, the
hard
and
soft palate
of the midface are mobile with respect to the
remainder of facial structures. This finding can be inconsistent due to the midfacial
bleeding
and
swelling
that typically accompany such injuries, and
so confirmation is usually needed by
radiograph
or
CT
.
[3]
•
Classification
[
edit
]
•
LeFort I fracture
•
There are three types of Le Fort fractures. As the classification increases, the anatomic level of the maxillary fracture ascends from inferior to
superior with respect to the maxilla:
•
Le Fort I fracture
(horizontal), otherwise known as a
floating palate
, may result from a force of injury directed low on the maxillary
alveolar rim
, or
upper dental row, in a downward direction. The essential component of these fractures, in addition to pterygoid plate involvement, is involvement of
the
lateral
bony margin of the nasal opening
. They also involve the medial and lateral buttresses, or walls, of the
maxillary sinus
, traveling through
the face just above the
alveolar ridge
of the upper dental row. At the midline, the inferior nasal septum is involved. Historically, it has also been
referred to as a
Guérin
fracture, although this name is less commonly used in practice.
•
LeFort II fracture
•
Le Fort II fracture
(pyramidal) may result from a blow to the lower or mid maxillary area. In addition to pterygoid plate disruption, their distinguishing
component is involvement of
inferior orbital rim
. When viewed from the front, the fracture is classically shaped like a pyramid. It extends from the
nasal bridge at or below the nasofrontal suture through the superior medial
wall
of the maxilla, inferolaterally through the
lacrimal bones
which
contain the tear ducts, and inferior orbital floor through or near the
infraorbital foramen
.
•
LeFort III fracture
•
Le Fort III fracture
(transverse), otherwise known as
craniofacial dissociation
, may follow impact to the nasal bridge or upper maxilla. The salient
feature of these fractures, beyond pterygoid plate involvement, is that they invariably involve the
zygomatic arch
, or cheek bone. These fractures
begin at the nasofrontal and frontomaxillary sutures and extend posteriorly along the medial wall of the orbit, through the nasolacrimal groove
and
ethmoid air cells
. The
sphenoid
is thickened posteriorly, limiting fracture extension into the optic canal. Instead, the fracture continues along the
orbital floor and infraorbital fissure, continuing through the lateral orbital wall to the zygomaticofrontal junction and zygomatic arch. Within the
nose, the fracture extends through the base of the perpendicular plate of the ethmoid air cells, the
vomer
, which are both part of the nasal septum.
As with the other fractures, it also involves the junction of the pterygoids with the maxillary sinuses.
CSF rhinorrhea
, or leakage of the nutrient laden
fluid that bathes the brain, is more commonly seen with these injuries due to ethmoid air cell disruption, as the air cells are located immediately
beneath the skull base.
[
•
A 3-D CT reconstruction showing a LeFort type
1 fracture ( fracture line is marked by an arrow
)
LeFort I fracture
LeFort II fracture
LeFort III fracture
•
Treatment[
edit
]
•
Treatment is surgical, and usually is able to be performed once life-
threatening injuries are stabilized, to allow the patient to survive
the general anesthesia needed for
maxillofacial surgery
. First
a
frontal bar
is used, which refers to the thickened frontal bone
above the frontonasal sutures and the superior orbital rim. The
facial bones are suspended from the bar by open reduction and
internal fixation with
titanium
plates and screws, and each fracture
is fixed, first at its superior attachment to the bar, then at the
inferior attachment to the displaced bone. For stability, the
zygomaticofrontal suture is usually replaced first, and the palate
and alveolar ridge are usually fixed last. Finally, after the horizontal
and vertical maxillary buttresses are stabilized, the orbital fractures
are fixed last.
•
Le Fort fractures
are fractures of the midface, which collectively involve
separation of all or a portion of the midface from the
skull base
. In order
to be separated from the skull base, the
pterygoid plates
of the
sphenoid
bone
need to be involved as these connect the midface to the sphenoid
bone dorsally. The Le Fort classification system attempts to distinguish
according to the plane of injury.
•
Classification
•
The commonly used classification is as follows:
•
Le Fort type I
–
horizontal
maxillary
fracture, separating the
teeth
from the upper face
–
fracture line passes through the alveolar ridge, lateral nose and
inferior wall of the
maxillary sinus
•
Le Fort type II
–
pyramidal fracture, with the teeth at the pyramid base, and
nasofrontal suture at its apex
–
fracture arch passes through the posterior alveolar ridge, lateral walls
of maxillary sinuses,
inferior orbital rim
and
nasal bones
–
uppermost fracture line can pass through the nasofrontal junction or
the frontal process of the maxilla
3
•
Le Fort type III
–
craniofacial disjunction
–
transverse fracture line passes through
nasofrontal suture
,
maxillo-
frontal suture
,
orbital wall
, and
zygomatic arch
/
zygomaticofrontal
suture
–
because of the involvement of the zygomatic arch, there is a risk of
the
temporalis
muscle impingement
•
A memory aid is:
•
Le Fort I is a floating
palate
(horizontal)
•
Le Fort II is a floating
maxilla
(pyramidal)
•
Le Fort III is a floating face (transverse)
•
Any combination is possible. For example, there may be type 2 on one side
and contralateral type 3, or there may be unilateral type 1 and 2 fractures.
It should be noted that Le Fort fractures are often associated with other
facial fractures, neuromuscular injury and dental avulsions.
•
History and etymology
•
They are named after
René Le Fort
,
French surgeon (1869-1951). Le Fort
conducted experiments on 35 cadavers inflicting varying facial trauma by
dropping cannon balls and striking them with a bat. He would then boil
the heads to remove soft tissue and record the results
4,5
.
•
Practical points
•
fracture of the
pterygoid plates
is mandatory to diagnose Le Fort fractures
•
if the anterolateral margins of the nasal fossa are intact it excludes a type I
fracture
•
if the zygomatic arch is intact it excludes a type III fracture
•
if the infraorbital rims are intact it excludes a type III fracture
•
if the nasofrontal suture is involved, then it is either a type II or III fracture
•
e Fort Fractures
•
BACKGROUND
•
Definition
•
Term applied to transverse fractures of the midface.
The fractures involve three bones of the midface
–
Maxilla
–
Orbital rims
–
Zygoma
•
All involve the pterygoid processes of the sphenoid
bones, which make up intrinsic support of the midface
–
Results in discontinuity of the midface
•
Fun fact: These fractures were named by Rene Le Fort, a French surgeon in 1901
who took intact cadavers and caused forceful blunt trauma to the skulls.
•
Epidemiology
•
Low-velocity mechanism (fall from standing, blunt trauma) resulted in the majority
of Le Fort I fractures (56%)
•
High-velocity mechanism
(fall >1 story, high-speed MVC) were associated with
higher grade
Le Fort fractures (e.g. II, III)
(
Phillips 2017
)
•
Associated head and neck injuries
with higher grade Le Fort fractures: (ibid.)
–
Skull fracture (40.7%)
–
Closed head injury (5.4%)
–
Cervical spine injury (5.4%)
•
Classification
•
Three types, dependent on the plane of injury
•
Le Fort Type I: “Floating palate”
–
Involves a transverse fracture through the maxilla. Occurs above the roots of the teeth and
may result in mobility of the maxilla and hard palate from the midface
–
Can be associated with malocclusion and dental fractures
•
Le Fort Type II: “Floating maxilla”
This fracture
involves extension of the fracture superiorally.
Includes fractures of the nasal bridge, maxilla,
lacrimal bones, and orbital floors and rims
•
Typically bilateral and triangular in shape
•
Le Fort Type III: “Floating face”
–
Rare but are considered “craniofacial dysjunction”
–
They involve the bridge of the nose, the medial
walls of the orbit (ethmoids), the lateral orbital
walls, the maxilla and the zygomatic arch
–
The entire face can shift
•
•
EVALUATION
•
Findings on presentation
•
Severe facial ecchymosis (balloon face)
•
Severe nasal or oral hemorrhaging
•
Conjunctival hemorrhage.
•
CSF Rhinorrhea
•
Hemotympanum
•
Anosmia
•
Paresthesias of the face
•
Elongation of the face
•
Nasal disfiguration
•
Emphysema of the face
•
Exophthalmos
•
Racoon eyes
•
Auricular hematoma
•
Pupil asymmetry
•
Dental injuries
•
Sinking over the anterior face (dish face)
•
Knoop, Atlast of Emergency Medicine, 3rd Ed.
•
Diagnostics
•
Primary survey (ABCs) and then secondary survey (where your facial and ocular exam occur)
•
Physical exam
•
Palpation of the entire face will detect most fractures
•
Mobility in the hard palate (intraoral palpation) or maxilla when teeth are grasped and evaluated while stabilizing the forehead with the other hand
•
Pertinent questions to ask if the patient is awake and alert:
–
How is your vision? (
document visual acuity
)
–
Does your bite feel normal?
–
Does anything feel numb?
•
Imaging
•
Dedicated facial CT
–
Allows for imaging of orbits and fine fracture lines as well
•
Consider CT C-spine given high incidence of concomitant cervical spine injury
–
1.4% of patients with concomitant c-spine fracture / dislocation
(
Hasler 2012
)
•
No role in plain films due to the complexity of the facial bones
•
MANAGEMENT
•
Airway should always be managed first, protection from bleeding or mechanical disruption is key
–
Severe bleeding may occur from the nose or oropharynx and these can be managed with anterior packing
–
Posterior packing should be avoided if possible
unless the skull base is known to be intact.
–
In one series, 43.5% of patients with Le Fort III required tracheostomy (
Bagheri 2005
)
•
After the primary stabilization is achieved, other management can occur
–
Elevate the head of the bed to 40-60 degrees for anyone with a possible CSF leak (if not in spinal precautions)
–
Administering IV
antibiotics
, especially if CSF leak known orsuspected (though this is
not well supported by literature
) (
Soong 2014
)
•
First generation cephalosporins or Augmentin when sinus fractures are involved
–
Perform secondary exam
•
Disposition
–
There is an association between
Injury Severity Score
(ISS) and grade of Le Fort fracture (
Bagheri 2005
)
–
Majority of patient require admission; in one series:
•
52.2% placed in ICU
•
20.9% taken directly to OR (
ibid.
)
–
Goal is to restore the facial skeleton and proper masticatory function
–
Consult oral maxillofacial surgery (or whoever may be on call for facial trauma at your institution)
–
Consider neurosurgery consult if CSF leak noted
•
These patients commonly do not need intervention though
–
Consider ophthalmology consult within 24 hours depending on any ocular damage or involvement
•
https://vimeo.com/visualscience/lefort-
fractures-visualscience
Le Fort fractures are classic traumatic injuries affecting the midface, specifically the maxillary bone and surrounding structures. They are characterized by specific signs and symptoms, such as swelling, malocclusion, and mobility of teeth. Diagnosis typically involves physical examination and imaging techniques. These fractures are classified into three types based on the anatomic level of the maxillary fracture. French surgeon René Le Fort discovered these fracture patterns in the late 19th century.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Le Fort fracture of skull From Wikipedia, the free encyclopedia Jump to navigationJump to searchLeFort fractureLeFort I (red), II (blue), and III (green) fracturesA Le Fort fracture of the skull is a classic transfacial fracture of the midface, involving the maxillary bone and surrounding structures in either a horizontal, pyramidal or transverse direction. The hallmark of Lefort fractures is traumatic pterygomaxillary separation, which signifies fractures between the pterygoid plates, horseshoe shaped bony protuberances which extend from the inferior margin of the maxilla, and the maxillary sinuses. Continuity of this structure is a keystone for stability of the midface, involvement of which impacts surgical management of trauma victims, as it requires fixation to a horizontal bar of the frontal bone. The pterygoid plates lie posterior to the upper dental row, or alveolar ridge, when viewing the face from an anterior view. The fractures are named after French surgeon Ren Le Fort (1869 1951), who discovered the fracture patterns by examining crush injuries in cadavers.[1]
Signs and symptoms[edit] Le Fort I Slight swelling of the upper lip, ecchymosis is present in the buccal sulcus beneath each zygomatic arch, malocclusion, mobility of teeth. Impacted type of fractures may be almost immobile and it is only by grasping the maxillary teeth and applying a little firm pressure that a characteristic grate can be felt which is diagnostic of the fracture. Percussion of upper teeth results in cracked pot sound. Gu rin's sign is present characterised by ecchymosis in the region of greater palatine vessels. Le Fort II and Le Fort III (common) Gross edema of soft tissue over the middle third of the face, bilateral circumorbital ecchymosis, bilateral subconjunctival hemorrhage, epistaxis, CSF rhinorrhoea, dish face deformity, diplopia, enophthalmos, cracked pot sound. Le Fort II Step deformity at infraorbital margin, mobile mid face, anesthesia or paresthesia of cheek. Le Fort III Tenderness and separation at frontozygomatic suture, lengthening of face, depression of ocular levels (enophthalmos), hooding of eyes, and tilting of occlusal plane, an imaginary curved plane between the edges of the incisors and the tips of the posterior teeth. As a result, there is gagging on the side of injury.[
Diagnosis[edit] A 3-D CT reconstruction showing a LeFort type 1 fracture ( fracture line is marked by an arrow ) Diagnosis is suspected by physical exam and history, in which, classically, the hard and soft palate of the midface are mobile with respect to the remainder of facial structures. This finding can be inconsistent due to the midfacial bleeding and swelling that typically accompany such injuries, and so confirmation is usually needed by radiograph or CT.[3] Classification[edit] LeFort I fracture There are three types of Le Fort fractures. As the classification increases, the anatomic level of the maxillary fracture ascends from inferior to superior with respect to the maxilla: Le Fort I fracture (horizontal), otherwise known as a floating palate, may result from a force of injury directed low on the maxillary alveolar rim, or upper dental row, in a downward direction. The essential component of these fractures, in addition to pterygoid plate involvement, is involvement of the lateral bony margin of the nasal opening. They also involve the medial and lateral buttresses, or walls, of the maxillary sinus, traveling through the face just above the alveolar ridge of the upper dental row. At the midline, the inferior nasal septum is involved. Historically, it has also been referred to as a Gu rin fracture, although this name is less commonly used in practice. LeFort II fracture Le Fort II fracture(pyramidal) may result from a blow to the lower or mid maxillary area. In addition to pterygoid plate disruption, their distinguishing component is involvement of inferior orbital rim. When viewed from the front, the fracture is classically shaped like a pyramid. It extends from the nasal bridge at or below the nasofrontal suture through the superior medial wall of the maxilla, inferolaterally through the lacrimal bones which contain the tear ducts, and inferior orbital floor through or near the infraorbital foramen. LeFort III fracture Le Fort III fracture(transverse), otherwise known as craniofacial dissociation, may follow impact to the nasal bridge or upper maxilla. The salient feature of these fractures, beyond pterygoid plate involvement, is that they invariably involve the zygomatic arch, or cheek bone. These fractures begin at the nasofrontal and frontomaxillary sutures and extend posteriorly along the medial wall of the orbit, through the nasolacrimal groove and ethmoid air cells. The sphenoid is thickened posteriorly, limiting fracture extension into the optic canal. Instead, the fracture continues along the orbital floor and infraorbitalfissure, continuing through the lateral orbital wall to the zygomaticofrontal junction and zygomatic arch. Within the nose, the fracture extends through the base of the perpendicular plate of the ethmoid air cells, the vomer, which are both part of the nasal septum. As with the other fractures, it also involves the junction of the pterygoids with the maxillary sinuses. CSF rhinorrhea, or leakage of the nutrient laden fluid that bathes the brain, is more commonly seen with these injuries due to ethmoid air cell disruption, as the air cells are located immediately beneath the skull base.[
A 3-D CT reconstruction showing a LeFort type 1 fracture ( fracture line is marked by an arrow )
Treatment[edit] Treatment is surgical, and usually is able to be performed once life- threatening injuries are stabilized, to allow the patient to survive the general anesthesia needed for maxillofacial surgery. First a frontal bar is used, which refers to the thickened frontal bone above the frontonasal sutures and the superior orbital rim. The facial bones are suspended from the bar by open reduction and internal fixation with titanium plates and screws, and each fracture is fixed, first at its superior attachment to the bar, then at the inferior attachment to the displaced bone. For stability, the zygomaticofrontal suture is usually replaced first, and the palate and alveolar ridge are usually fixed last. Finally, after the horizontal and vertical maxillary buttresses are stabilized, the orbital fractures are fixed last.
Le Fort fractures are fractures of the midface, which collectively involve separation of all or a portion of the midface from the skull base. In order to be separated from the skull base, the pterygoid plates of the sphenoid bone need to be involved as these connect the midface to the sphenoid bone dorsally. The Le Fort classification system attempts to distinguish according to the plane of injury. Classification The commonly used classification is as follows: Le Fort type I horizontal maxillary fracture, separating the teeth from the upper face fracture line passes through the alveolar ridge, lateral nose and inferior wall of the maxillary sinus Le Fort type II pyramidal fracture, with the teeth at the pyramid base, and nasofrontal suture at its apex fracture arch passes through the posterior alveolar ridge, lateral walls
e Fort Fractures BACKGROUND Definition Term applied to transverse fractures of the midface. The fractures involve three bones of the midface Maxilla Orbital rims Zygoma All involve the pterygoid processes of the sphenoid bones, which make up intrinsic support of the midface Results in discontinuity of the midface
Fun fact: These fractures were named by Rene Le Fort, a French surgeon in 1901 who took intact cadavers and caused forceful blunt trauma to the skulls. Epidemiology Low-velocity mechanism (fall from standing, blunt trauma) resulted in the majority of Le Fort I fractures (56%) High-velocity mechanism (fall >1 story, high-speed MVC) were associated with higher grade Le Fort fractures (e.g. II, III) (Phillips 2017) Associated head and neck injuries with higher grade Le Fort fractures: (ibid.) Skull fracture (40.7%) Closed head injury (5.4%) Cervical spine injury (5.4%) Classification Three types, dependent on the plane of injury Le Fort Type I: Floating palate Involves a transverse fracture through the maxilla. Occurs above the roots of the teeth and may result in mobility of the maxilla and hard palate from the midface Can be associated with malocclusion and dental fractures
Le Fort Type II: Floating maxillaThis fracture involves extension of the fracture superiorally. Includes fractures of the nasal bridge, maxilla, lacrimal bones, and orbital floors and rims Typically bilateral and triangular in shape
Le Fort Type III: Floating face Rare but are considered craniofacial dysjunction They involve the bridge of the nose, the medial walls of the orbit (ethmoids), the lateral orbital walls, the maxilla and the zygomatic arch The entire face can shift
EVALUATION Findings on presentation Severe facial ecchymosis (balloon face) Severe nasal or oral hemorrhaging Conjunctival hemorrhage. CSF Rhinorrhea Hemotympanum Anosmia Paresthesias of the face Elongation of the face Nasal disfiguration Emphysema of the face Exophthalmos Racoon eyes Auricular hematoma Pupil asymmetry Dental injuries Sinking over the anterior face (dish face) Knoop, Atlast of Emergency Medicine, 3rd Ed. Diagnostics Primary survey (ABCs) and then secondary survey (where your facial and ocular exam occur) Physical exam Palpation of the entire face will detect most fractures Mobility in the hard palate (intraoral palpation) or maxilla when teeth are grasped and evaluated while stabilizing the forehead with the other hand Pertinent questions to ask if the patient is awake and alert: How is your vision? (document visual acuity) Does your bite feel normal? Does anything feel numb? Imaging Dedicated facial CT Allows for imaging of orbits and fine fracture lines as well Consider CT C-spine given high incidence of concomitant cervical spine injury 1.4% of patients with concomitant c-spine fracture / dislocation(Hasler 2012) No role in plain films due to the complexity of the facial bones MANAGEMENT Airway should always be managed first, protection from bleeding or mechanical disruption is key Severe bleeding may occur from the nose or oropharynx and these can be managed with anterior packing Posterior packing should be avoided if possible unless the skull base is known to be intact. In one series, 43.5% of patients with Le Fort III required tracheostomy (Bagheri 2005) After the primary stabilization is achieved, other management can occur Elevate the head of the bed to 40-60 degrees for anyone with a possible CSF leak (if not in spinal precautions) Administering IV antibiotics, especially if CSF leak known orsuspected (though this is not well supported by literature) (Soong 2014) First generation cephalosporins or Augmentin when sinus fractures are involved Perform secondary exam Disposition
https://vimeo.com/visualscience/lefort- fractures-visualscience
, II (blue), and III (green)")