Health Systems Assessment: Understanding Control Knobs and Policy Levers
Health Systems Assessment webinar series explores the importance of evaluating health systems to achieve social goals. Topics include Control Knob Framework, Ultimate & Intermediate Outcomes, and Financing options. Learn how policy levers impact system performance through metaphorical control knobs in health sector reforms.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Introduction to Health Systems Assessment Prof. Winnie Yip Webinar Series on Health Systems Assessment July 28, 20201
Why health system assessment? Why health system assessment? A health system is a means to achieve some social end goals. Thus, how good a health system is, is judged by how well the end goals are met.
The Control Knob Framework The Control Knob Framework A health system is a means to an end The Policy Reform Cycle The Control Knob Framework
Ultimate Ultimate & Intermediate Outcomes & Intermediate Outcomes of Health Systems of Health Systems Final Outcomes Intermediate Outcomes Level (Average) Distribution Health Status 1. Access Financial Risk Protection 2. Quality 3. Efficiency Citizen Satisfaction The future webinars in this series will delve into each of these topics in detail
The Control Knobs/Levers The Control Knobs/Levers Financing Payment Organization Regulation Persuasion (Behavior)
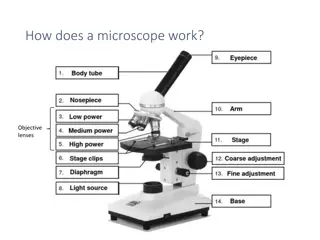
To understand why a health system performs well or not, we trace back to 5 policy levers
What is a What is a Control Knob ? Control Knob ? A metaphor about how health system reform can be understood Each knob is a set of features of the health sector that can be changed by public policy; that someone can control Changing the setting is likely to change the performance of the health sector Using more than one control knob is normally required to change system performance
Financing Financing Resource mobilization Risk pooling Resource allocation Typical financing options General revenue Social insurance (mandatory) Private insurance (voluntary) Out-of-pocket payment Community financing International aid Most real systems depart from any one ideal type and use a mix of financing options
The Importance of Financing Choices The Importance of Financing Choices Methods chosen affect the amount of available funds Methods chosen affect burden of who pays Different approaches change who has authority over the system Different approaches change what services are available and to whom
Provider Payment Provider Payment Each provider payment method creates different incentives for the providers The impact of provider payment depends on both the method and the level of payment Payment options: Doctors Fee for service Salary Salary plus bonus Capitation Capitation plus bonus Hospitals Patient day Admission/DRG Global budget Line item budget Fee for service
Organization Organization Macro level Market structure: e.g. competition, monopoly, share of private sector Centralized vs decentralized Meso level Ownership Governance Internal management Internal incentives Structure of delivery organizations Policymakers have a limited capacity to make changes inside delivery organizations not in the public sector
Regulation Regulation The use of the coercive power of the State to influence actors in the health sector to change their behaviour Examples: Price regulation Entry and exit of providers through licensing Approval of drugs This power may be delegated to non-state actors Health care regulation has many purposes: Establish markets Protect consumers from their inability to judge quality and quantity Counteract market failures and external effects Achieve non-market goals
Persuasion Persuasion Both patient and provider behavior are relevant targets of persuasion Information alone does not change behavior Environments can influence behavior powerfully Messages need to be carefully designed to appeal to the goals and values of the target population There are many possible communication channels: free media, paid media, individual contact, groups, big events, etc.
Health System Diagnosis - an illustration from Odisha
A snapshot of the health system in Odisha Hybrid system with public and private providers. Fragmented delivery without linkages between different levels of care. Majority seek care at public facilities for both IP and OP. Delivery System No formal referral linkages, no gate-keeping. Lower level facilities are bypassed due to poor quality More providers in urban areas, coastal/central districts. Fewer in northern, southern districts Government spends only 0.9% of its GSDP on health. Majority of THE is borne by individuals through OOPE (76%). GHE (%THE): 21.6%. Minimal pooling Most of the government money is spent on hospitals and curative care. Most of the OOPE is spent on drugs GHIS: BSKY eligibility based on poverty and other vulnerability criteria (SC/ST, disability, etc.). CGHS for civil servants, ESI for formal sector workers Fragmented Risk Pools: Multiple risk pools and payment rates Multiple purchasers BSKY (earlier BKKY, RSBY), CGHS; ESI; most purchasing is by individuals (reflected in high OOPE) Benefit Package: Wide-ranging coverage across different schemes. BSKY only hospitalization, no OP care/drugs Cost-sharing: No cost-sharing with beneficiaries. BSKY is entirely tax-financed. SHI not feasible due to large informal sector & low payroll tax contribution Providers: BSKY & CGHS automatically empanels all public hospitals. Private hospitals need to fulfil certain simple criteria. ESI has their own network of providers. Health Financing Physicians in public system paid by salaries earn as per pay-grades (not performance). Private providers are paid through OOPE-POS. Provider Payment Mechanisms (PPM) Public hospitals paid with line item budgets + reimbursement for BSKY & other GHIS. Private hospitals paid by OOPE. Private hospitals empanelled under BSKY/GHIS get reimbursements as per set package rates. Cost Control No clear cost-control mechanisms, except wait times, limited timings in the public system Regulatory mechanisms exist but are not strictly enforced Regulation
Diagnosis possible underlying causes of poor performance Health System Goal CHE rates for hospitalization, by public/private & with/without insurance Figure 1.5: CHE rates for hospitalization, by public/private, and with/without insurance Figure 1.4: CHE rates for hospitalization, by public/private facility Inadequate Insurance Coverage 1 Population coverage too low: No universal GHIS. ~85% popn qualify for BSKY, but only 15% households reported having insurance Low Financial Risk Protection (FRP) Insufficient benefit package: BSKY covers only secondary/tertiary care (not the main causes of OOPE) Both insured & uninsured HHs incur OOPE/CHE High OOPE = 76% of THE CHE = 24% IHE = 10% OOPE/CHE incurred both at public & private sector hospitals Type of care and provider Share of patients with CHE (using monthly consumption expenditure) Mean spend per visit (Rupees) Drug share of OOP Mean drug OOP (Rupees) Share purchasing drugs from private sector chemist 2 High OOPE in public + private sector Outpatient 790 68% of OOPE on drugs Public (46%) Private hospital outpatient departments and solo providers (24%) Private Chemists and other providers (30%) 25% 59% 428 72% Majority of OP care from private sector (54%), including ~15% to chemist shops. Even those who seek care from public sector buy medicines from pvt chemists 38% 1404 67% 754 100% Majority IP care from public sector - supposed to be free, Niramaya for free essential drugs 25% 735 73% 512 98% Inpatient Public (75%) Private (25%) n/a 19% 10,407 41% 3,287 n/a 52% 33,886 37% 10,380
Health System Goal Diagnosis possible underlying causes of poor performance 1.1 Inadequate Insurance Coverage 1 Why is popn coverage low? - Implementation gaps - low awareness among the insured Population coverage too low: No universal GHIS. ~85% popn qualify for BSKY, but only 15% households reported having insurance Low Financial Risk Protection (FRP) Insufficient benefit package: BSKY covers only secondary/tertiary care (not the main causes of OOPE) 1.2 High OOPE = 76% of THE CHE = 24% IHE = 10% Why is benefit package thin? - Lack of funds - BSKY design; How to empanel/pay OP care providers, private providers -Moral hazard, overuse Both insured & uninsured HHs incur OOPE/CHE 68% of OOPE on drugs
Health System Goal Diagnosis possible underlying causes of poor performance 2 High OOPE in public + private sector 2.1 Majority of OP care from private sector (54%), including ~15% to chemist shops. Even those who seek care from public sector buy medicines from pvt chemists Why is there OOPE in public? Poor supply of drugs, frequent stock-outs at public facilities: Availability of medicines vary by level of care, with very low availability at primary levels: - 73% essential medicines in stock at public hospitals, 59% at private hospitals, 66% at CHCs. - 38% at PHCs, 18% at Sub-centers and HWCs, 48% at private chemist shops. Low Financial Risk Protection (FRP) Majority IP care from public sector - supposed to be free, Niramaya for free essential drugs High OOPE = 76% of THE CHE = 24% IHE = 10% OOPE/CHE incurred both at public & private sector hospitals 68% of OOPE on drugs
Health System Goal Diagnosis possible underlying causes of poor performance Geographical co-location of private chemist shops around public facilities 2.2 High OOPE in public + private sector 2 Why seek private care? People s preference of providers based on convenience, quality - - Common reasons reported by users: better stock & variety of drugs, more convenient hours. Chemists are open 11.5 hrs/day. Majority of OP care from private sector (54%), including ~15% to chemist shops. Even those who seek care from public sector buy medicines from pvt chemists Low Financial Risk Protection (FRP) Majority IP care from public sector - supposed to be free, Niramaya for free essential drugs High OOPE = 76% of THE CHE = 24% IHE = 10% Public providers may refer patients to private chemists (financial interests, ownership, commissions, etc.) - 15% were referred to chemists by public providers - Providers may prescribe drugs that they know are not stocked in the public facility but available at pvt chemists OOPE/CHE incurred both at public & private sector hospitals 68% of OOPE on drugs Providers & chemist shops may collaborate through geographical co-location. 93% public hospitals have ~8 chemist shops & 58% public primary facilities have ~2 shops within 3 km radius.
Health System Goal Diagnosis possible underlying causes of poor performance 2.3 2 Are they given too many drugs (irrational care)? - All providers prescribed ~3 drugs for different conditions. Public providers prescribed more than private (on average) - ~40% of all cases were prescribed unnecessary drugs - Majority of prescriptions were for branded drugs, not generics High OOPE in public + private sector Majority of OP care from private sector (54%), including ~15% to chemist shops. Even those who seek care from public sector buy medicines from pvt chemists Low Financial Risk Protection (FRP) Majority IP care from public sector - supposed to be free, Niramaya for free essential drugs High OOPE = 76% of THE CHE = 24% IHE = 10% OOPE/CHE incurred both at public & private sector hospitals 68% of OOPE on drugs
Health System Goal Diagnosis possible underlying causes of poor performance 2.4 2 High OOPE in public + private sector Are current provider payment mechanisms leading to high OOPE? -Line item budgets - GHIS Reimbursement minimal for public, rates lower than private charges + significant delays. Not motivating - FFS - perverse incentives for supply-induced demand -Turning away GHIS patients, charging OOPE, balance- billing -Cost-shifting in case of fragmented schemes, different payment rates Majority of OP care from private sector (54%), including ~15% to chemist shops. Even those who seek care from public sector buy medicines from pvt chemists Low Financial Risk Protection (FRP) Majority IP care from public sector - supposed to be free, Niramaya for free essential drugs High OOPE = 76% of THE CHE = 24% IHE = 10% OOPE/CHE incurred both at public & private sector hospitals 68% of OOPE on drugs
Examples of survey questions/analysis for assessments Research question Survey instruments 1 3 4 1 2 Supplies not available, leakages? Examine scenarios of CHE with/without OOP on private sector drugs for public sector visit to assess whether a major driver of CHE Compare drug stocks in public and private sectors (facilities and chemist shops) to see if stocks differ by drug and sector Compare drug stocks by sector to the disease areas people spending the most money on Compare and contrast ordering, supplier and financing questions by sector to examine whether private sector has better processes Household Survey 1 2 3 4 Out-patient Exit interviews 2 People s preferences of drugs/providers? Assess revealed preference Examine perceptions of drug quality from public/private Examine relationship between patient satisfaction and drugs Examine perceptions of providers/quality & reasons behind preferences 1 2 3 4 Why is there OOPE in the public sector? In-patient Exit interviews 1 3 Facility surveys Supply-induced demand? Doctors prescribe more drugs, costlier drugs, unnecessary drugs? Examine prescription behavior of providers for common illnesses Assess provider knowledge about correct treatment (necessary drugs) Compare the number of unnecessary drugs prescribed with the costs of those drugs Public& private providers refer to specific private chemists (profit motive?) examine referral patterns Is there dual practice or ownership of chemist shops by public doctors? 1 3 Public providers, private solo providers, chemist shops 3 4 Clinical vignettes Informal payments? Examine how common reports of paying other fees/gifts in public sector Examine the average monetary amount of these payments
Health system design is not just a technical problem. Politics and Ethics matter. Reform is a process.
Thank you Thank you