DIALOG in London Training Package


P
a
n
L
o
n
d
o
n
T
r
a
i
n
i
n
g
p
a
c
k
a
g
e
D
I
A
L
O
G






S
e
c
t
i
o
n
1
S
e
c
t
i
o
n
2
S
e
c
t
i
o
n
3
•
W
h
a
t
i
s
D
I
A
L
O
G
?
•
H
o
w
t
o
r
a
t
e
D
I
A
L
O
G
•
D
I
A
L
O
G
+
•
W
h
e
n
s
h
o
u
l
d
D
I
A
L
O
G
b
e
c
o
m
p
l
e
t
e
d
?
•
D
I
A
L
O
G
a
s
a
n
o
u
t
c
o
m
e
m
e
a
s
u
r
e
•
W
h
y
D
I
A
L
O
G
w
a
s
a
g
r
e
e
d
a
s
t
h
e
L
o
n
d
o
n
P
R
O
M
•
R
e
c
o
v
e
r
y
p
r
i
n
c
i
p
l
e
s
•
R
e
f
l
e
c
t
i
o
n
e
x
e
r
c
i
s
e
•
S
e
r
v
i
c
e
u
s
e
r
f
e
e
d
b
a
c
k
o
n
D
I
A
L
O
G
a
n
d
D
I
A
L
O
G
+
•
U
s
e
f
u
l
e
x
a
m
p
l
e
s
o
f
h
o
w
d
a
t
a
i
s
s
t
a
r
t
i
n
g
t
o
b
e
u
s
e
d
•
A
n
a
l
y
s
i
n
g
D
I
A
L
O
G
d
a
t
a
•
H
o
w
t
o
u
s
e
D
I
A
L
O
G
o
n
E
P
R
•
U
s
i
n
g
D
I
A
L
O
G
+
i
n
t
h
e
c
a
r
e
p
l
a
n



S
e
c
t
i
o
n
1
D
I
A
L
O
G
i
s
a
s
e
t
o
f
1
1
s
i
m
p
l
e
q
u
e
s
t
i
o
n
s
t
h
a
t
c
o
v
e
r
d
i
f
f
e
r
e
n
t
a
r
e
a
s
o
f
a
p
e
r
s
o
n
’
s
l
i
f
e
.
W
h
a
t
i
s
D
I
A
L
O
G
?
How satisfied are you
with….
1.
Y
our mental health?
2.
Your physical health?
3.
Your job
situation?
4.
Your
accommodation?
5.
Your leisure activities?
6.
Your relationships with your partner/family?
7.
Your friendships?
8.
Your personal safety?
9.
Your medication?
10.
he practical help you receive?
11.
Your meeting with your mental health
professionals?
S
e
c
t
i
o
n
1
How satisfied are you with your mental health?
How satisfied are you with your physical health?
How satisfied are you with your job situation?
How satisfied are you with your accommodation?
How satisfied are you with your leisure activities?
How satisfied are you with your relationships with your partner/family?
How satisfied are you with your friendships?
D
I
A
L
O
G
c
a
n
h
e
l
p
f
a
c
i
l
i
t
a
t
e
a
p
e
r
s
o
n
-
c
e
n
t
r
e
d
a
p
p
r
o
a
c
h
b
y
s
u
p
p
o
r
t
i
n
g
m
e
a
n
i
n
g
f
u
l
c
o
n
v
e
r
s
a
t
i
o
n
s
b
e
t
w
e
e
n
s
e
r
v
i
c
e
u
s
e
r
s
a
n
d
t
h
e
h
e
a
l
t
h
c
a
r
e
p
r
o
f
e
s
s
i
o
n
a
l
a
b
o
u
t
w
h
a
t
a
s
p
e
c
t
s
o
f
t
h
e
i
r
l
i
v
e
s
a
r
e
i
m
p
o
r
t
a
n
t
t
o
t
h
e
m
.
H
o
w
t
o
r
a
t
e
D
I
A
L
O
G
How satisfied are you with your personal safety?
How satisfied are you with your medication?
How satisfied are you with the practical help you receive?
How satisfied are you with your meetings with mental health professionals?
…
a
n
d
t
h
e
l
a
s
t
t
h
r
e
e
a
r
e
a
b
o
u
t
y
o
u
r
t
r
e
a
t
m
e
n
t
-
t
h
e
s
e
a
r
e
r
e
f
e
r
r
e
d
t
o
a
s
‘
t
r
e
a
t
m
e
n
t
d
o
m
a
i
n
s
’
T
h
e
f
i
r
s
t
e
i
g
h
t
q
u
e
s
t
i
o
n
s
c
o
v
e
r
d
i
f
f
e
r
e
n
t
a
r
e
a
s
o
f
a
p
e
r
s
o
n
s
l
i
f
e
-
t
h
e
s
e
a
r
e
r
e
f
e
r
r
e
d
t
o
a
s
‘
l
i
f
e
d
o
m
a
i
n
s
’
H
o
w
t
o
r
a
t
e
D
I
A
L
O
G
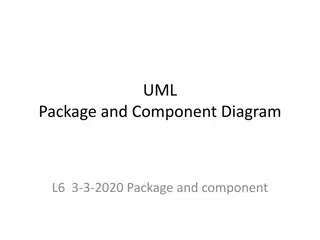
The survey is designed to
measure how a person rates
their quality of life and
experience of the care that
they receive.
Totally
satisfied
Totally
dissatisfied
Very
dissatisfied
Fairly
dissatisfied
Fairly
satisfied
Very
satisfied
In the middle
… with 1 being totally
dissatisfied and 7 being
totally satisfied.
S
c
o
r
e
s
:
1
-
3
e
x
p
l
i
c
i
t
d
i
s
s
a
t
i
s
f
a
c
t
i
o
n
,
4
n
e
u
t
r
a
l
m
i
d
d
l
e
,
5
-
7
e
x
p
l
i
c
i
t
s
a
t
i
s
f
a
c
t
i
o
n
D
I
A
L
O
G
+
1
.
U
n
d
e
r
s
t
a
n
d
i
n
g
2
.
L
o
o
k
i
n
g
f
o
r
w
a
r
d
3
.
E
x
p
l
o
r
i
n
g
o
p
t
i
o
n
s
4
.
A
g
r
e
e
i
n
g
o
n
a
c
t
i
o
n
s
D
I
A
L
O
G
+
u
s
e
s
a
4
s
t
e
p
a
p
p
r
o
a
c
h
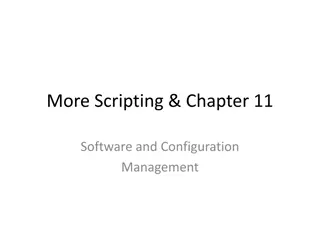
Exploring both positive and
negative aspects of the situation in
the given domain. The person is
first asked to explain the reasons
for dissatisfaction and wishes for
more help (or distress/concern in
case of MH). Then the person is
encouraged to consider existing
strengths or coping strategies.
Directing the patient from a
description of the problem to
considering desired alternative
scenarios. The patient is asked to
imagine what changes he/she
would like to see to replace the
current undesirable situation. This
can focus on long-term preferred
outcomes and more short term
small changes.
Asking the patient about what
practical actions might help
to bring about the desired
change. This covers actions
taken by the patient, the
healthcare professional or
someone else.
Agreeing on defined actions to
improve the patient’s condition
and/or social situation. This step
involves an agreement on specific
and defined actions from the
patient or the healthcare
professional or both. The agreed
actions are briefly documented.
DIALOG+ uses the scores identified by the person to
help structure a conversation between the healthcare
professional and the person to explore their identified
needs and wishes, support care planning, and help
service users take an active problem-solving
approach to promoting recovery.
To find out more information see the
Operational Manual
DIALOG+ is a specific intervention that uses the DIALOG scale and a 4- step approach based
on solution focused therapy.
W
h
e
n
s
h
o
u
l
d
D
I
A
L
O
G
b
e
c
o
m
p
l
e
t
e
d
?
At the start of a
new
treatment
episode i.e.
admission to an
inpatient treatment, home
treatment service, or other community service;
referral to new provider organisation
.)
Every
4 weeks
for
acute
treatment
–
inpatients and crisis teams.
No longer
than
6 months
for
ongoing
treatment in
community services and
outpatient clinics
.
E
p
i
s
o
d
e
s
t
a
r
t
E
p
i
s
o
d
e
e
n
d
R
e
v
i
e
w
For
acute
treatment DIALOG should be
carried out within
48 hours.
F
or
community
settings it should be
obtained within the
first or second
meeting
More frequent DIALOGs maybe carried
out if embedded within Care
Programme Approach (CPA) process or
when carrying out DIALOG is clinically
indicated.
At the end of treatment episode
(discharge from a team, service or
provider organisation).
London has agreed minimum time points in which DIALOG should be completed to ensure a standardised process.
D
I
A
L
O
G
a
s
a
n
o
u
t
c
o
m
e
m
e
a
s
u
r
e
H
e
a
l
t
h
c
a
r
e
p
r
o
f
e
s
s
i
o
n
a
l
s
c
a
l
l
t
h
i
s
a
p
a
t
i
e
n
t
r
e
p
o
r
t
e
d
o
u
t
c
o
m
e
m
e
a
s
u
r
e
(
P
R
O
M
)
.
It is an assessment of
health status and health-
related quality of life that
comes directly from the
patient.
PROMs provide services
with a measure of the
subjective impact of the
services on a person’s
health and wellbeing.
In London DIALOG has been
agreed to be used for Early
Intervention in Psychosis (EIP)
and Care Programme Approach
(CPA) services. DIALOG can be
used in wider mental health
service in the future.
Why has DIALOG been chosen as the London Patient Reported Outcome Measure (PROM)?
The scale has been
shown to have good
psychometric
properties.
Service users
report
satisfaction in
using it.
It is simple to use.
The information
can be used for
planning for
individual
patients and
whole services.
It can be used to
evaluate treatment
and has the
advantage that each
item is meaningful.
The use of DIALOG +
has been shown to
improve quality of life
through a solution
focused approach.
London mental health partners came together to agree that DIALOG should be the London Patient
Reported Outcome Measure (PROM).
D
I
A
L
O
G
w
a
s
a
g
r
e
e
d
t
o
b
e
u
s
e
d
b
e
c
a
u
s
e
…
…
.
.
R
e
c
o
v
e
r
y
P
r
i
n
c
i
p
l
e
s
:
C
H
I
M
E
f
r
a
m
e
w
o
r
k
S
o
u
r
c
e
:
L
e
a
m
y
e
t
a
l
2
0
1
1
T
h
e
C
H
I
M
E
f
r
a
m
e
w
o
r
k
i
s
a
c
o
n
c
e
p
t
u
a
l
f
r
a
m
e
w
o
r
k
f
o
r
p
e
r
s
o
n
a
l
r
e
c
o
v
e
r
y
i
n
m
e
n
t
a
l
h
e
a
l
t
h
.
I
t
s
t
a
n
d
s
f
o
r
C
o
n
n
e
c
t
e
d
n
e
s
s
,
H
o
p
e
,
I
d
e
n
t
i
t
y
,
M
e
a
n
i
n
g
f
u
l
a
n
d
E
m
p
o
w
e
r
m
e
n
t
.
T
h
i
s
f
r
a
m
e
w
o
r
k
c
a
n
c
o
m
p
l
e
m
e
n
t
t
h
e
D
I
A
L
O
G
a
p
p
r
o
a
c
h
.
12
O
p
t
i
o
n
a
l
P
e
r
s
o
n
a
l
R
e
f
l
e
c
t
i
o
n
E
x
e
r
c
i
s
e
f
o
r
t
r
a
i
n
e
e
s
1
/
2
(This is not for sharing unless you wish to do so).
Fold a piece of paper in 4
On each quarter put aspects of your life that represent
how you and others see you i.e. mother, friend etc
S
t
e
p
1
W
e
a
r
e
n
o
w
g
o
i
n
g
t
o
u
n
d
e
r
t
a
k
e
a
s
h
o
r
t
e
x
e
r
c
i
s
e
t
h
a
t
h
e
l
p
s
p
u
t
t
h
e
r
e
c
o
v
e
r
y
p
r
i
n
c
i
p
l
e
s
i
n
t
o
c
o
n
t
e
x
t
Group reflection
S
t
e
p
2
S
t
e
p
3
T
r
a
i
n
e
r
s
:
p
l
e
a
s
e
s
e
e
f
a
c
i
l
i
t
a
t
i
o
n
p
r
o
m
p
t
s
w
i
t
h
i
n
t
h
e
n
o
t
e
s
s
e
c
t
i
o
n
o
f
t
h
e
s
l
i
d
e
s
S
e
c
t
i
o
n
2
S
e
r
v
i
c
e
u
s
e
r
f
e
e
d
b
a
c
k
o
n
D
I
A
L
O
G
a
n
d
D
I
A
L
O
G
+
S
e
r
v
i
c
e
u
s
e
r
s
h
a
v
e
d
e
s
c
r
i
b
e
d
t
h
e
b
e
n
e
f
i
t
s
o
f
u
s
i
n
g
D
I
A
L
O
G
a
n
d
D
I
A
L
O
G
+
[
P
l
a
c
e
h
o
l
d
e
r
]
We recommend that Trusts co-deliver the training with service users, with
service users reflecting on their own experience of how DIALOG/DIALOG+
has supported them. In the initial delivery of training Trusts may not be able
have a pool of service users to co deliver sessions. They may wish to play
the service user vignette video or the
Pat Deegan video
Watch this
short video
to hear
what service users who have
used DIALOG think
S
e
c
t
i
o
n
3
U
s
e
f
u
l
e
x
a
m
p
l
e
s
o
f
h
o
w
D
I
A
L
O
G
d
a
t
a
i
s
s
t
a
r
t
i
n
g
t
o
b
e
u
s
e
d
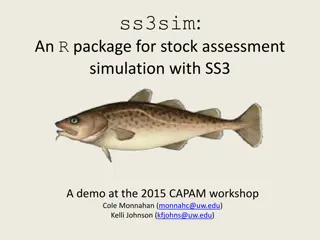
The data can be understood at an individual
level.
These charts shows how individual
DIALOG question categories can be viewed
to explore trends over time. The example is
over a 10-month period.
The data can be used to better understand team needs. The data
s
hows other aspects of people’s lives that they are dissatisfied with,
beyond their mental health, such as physical health,
job situation and
leisure activities. This can be used to direct focus around patients’
needs or for example staff skills and expertise.
T
h
e
r
e
a
r
e
d
i
f
f
e
r
e
n
t
w
a
y
s
t
h
a
t
D
I
A
L
O
G
d
a
t
a
c
a
n
b
e
u
n
d
e
r
s
t
o
o
d
a
n
d
u
s
e
d
t
o
s
u
p
p
o
r
t
a
p
e
r
s
o
n
’
s
m
e
n
t
a
l
h
e
a
l
t
h
a
n
d
i
m
p
r
o
v
e
t
h
e
q
u
a
l
i
t
y
o
f
t
h
e
s
e
r
v
i
c
e
.
S
o
u
r
c
e
:
T
h
i
s
d
a
t
a
i
s
a
n
o
n
y
m
i
s
e
d
d
a
t
a
t
a
k
e
n
f
r
o
m
E
a
s
t
L
o
n
d
o
n
N
H
S
F
o
u
n
d
a
t
i
o
n
T
r
u
s
t
A
n
a
l
y
s
i
n
g
D
I
A
L
O
G
d
a
t
a
Each of the DIALOG questions are rated using a Likert scale
from 1 (totally dissatisfied) 7 (totally satisfied).
*
T
r
e
a
t
m
e
n
t
e
p
i
s
o
d
e
-
r
e
f
e
r
s
t
o
t
h
e
p
e
r
i
o
d
o
f
t
i
m
e
a
p
e
r
s
o
n
i
s
r
e
c
e
i
v
i
n
g
t
r
e
a
t
m
e
n
t
(
f
r
o
m
t
h
e
i
n
i
t
i
a
l
D
I
A
L
O
G
s
c
o
r
e
t
o
t
h
e
l
a
s
t
D
I
A
L
O
G
s
c
o
r
e
)
.
When evaluating treatment episode
satisfaction the change score should be
considered to understand if subjective
quality of life has improved. Either mean
scores across the eight rated life
domains or ratings of single life domains
can be selected. This may depend on
the focus, and context of care, the
situation of the patients and the purpose
of the evaluation.
A
h
i
g
h
i
n
i
t
i
a
l
s
c
o
r
e
=
l
e
s
s
r
o
o
m
f
o
r
i
m
p
r
o
v
e
m
e
n
t
A
l
o
w
s
c
o
r
e
=
i
m
p
r
o
v
e
m
e
n
t
i
s
m
o
r
e
l
i
k
e
l
y
When evaluating satisfaction of
the treatment episode the most
recent score given during the
current treatment period is most
relevant than changes over time.
When analysing the
difference between
scores over two
timepoints it is important
to acknowledge the initial
score to understand the
overall scope for
improvement in
satisfaction.
The first eight DIALOG questions rate the satisfaction levels within different areas of life e.g accommodation.
The mean score of all eight questions gives an overall score of subjective quality of life as a Patient Rated
Outcome Measure (PROM).
S
u
b
j
e
c
t
i
v
e
q
u
a
l
i
t
y
o
f
l
i
f
e
The final three items ask to rate different aspects of treatment. The mean score of the last three question
gives an overall score for treatment satisfaction as a Patient Reported Experience Measure (PREM).
T
r
e
a
t
m
e
n
t
d
o
m
a
i
n
s
DIALOG data can be analysed at an individual item level or represented as mean scores for the team,
service or organisation. The below information should be read in conjunction with the
analytical framework
.
A
n
a
l
y
s
i
n
g
D
I
A
L
O
G
d
a
t
a
•
Used for an assessment
of personal problems
and areas of strength.
•
For
subjective quality of
life scores below 4
(explicit dissatisfaction)
require particular
attention.
•
When evaluating
treatment episode, any
improvement in
subjective quality of life
is a meaningful
increase.
•
For service users
receiving long term care
it is unrealistic to expect
consistent and ongoing
improvements;
understanding personal
context is important.
•
The data can be viewed in different ways- Scores of
single domains
(DIALOG
questions) of people in a service
can be shown as means
(average satisfaction scores) or as a % of patients who have explicit
dissatisfaction/satisfaction.
Mean team scores allow for review of data
across every item.
•
When considering changes over time, global mean scores
as well as
single
can be used depending on the purpose For example if one evaluates full
services with variable treatment tasks for a range of patients, it is
reasonable to explore first the global scores before considering the ratings
of single
life
domains. This applies to most services in most situations.
However, there may also be specific questions, e.g. on how services affect
the wide spread dissatisfaction of patients with their physical health.
•
Analysing the global score provides a general evaluation, whilst the
analysis of single
domains
provides more specific information about what
exactly services do and do not achieve.
W
h
e
n
i
n
t
e
r
p
r
e
t
i
n
g
s
c
o
r
e
s
:
•
The average subjective quality of life score of ALL patients in a service
should not improve as patients with better quality of life will be discharged
and new patients with lower quality of life be admitted, yet when you look at
individual scores improvements should be expected.
•
A change of overall mean scores of >0.125 reflects an average
improvement of at least one scale point in at least one life domain
(question) and may be a guide for overall meaningful improvement.
•
Ideally treatment satisfaction scores should consistently stay above 4 and
the % of patients with dissatisfaction <4 kept to a minimum
•
Follows same principles
as the interpretation for
all patients in a service.
•
When evaluating data at
an organisation level the
patient groups become
very large, this means
that the differences
between the mean
scores tend to become
smaller therefore
percentages of explicit
dissatisfaction or very
satisfied become more
informative than mean
scores.
O
r
g
a
n
i
s
a
t
i
o
n
I
n
d
i
v
i
d
u
a
l
S
e
r
v
i
c
e
D
o
m
a
i
n
-
r
e
f
e
r
s
t
o
t
h
e
i
n
d
i
v
i
d
u
a
l
D
I
A
L
O
G
q
u
e
s
t
i
o
n
e
.
g
H
o
w
s
a
t
i
s
f
i
e
d
a
r
e
y
o
u
w
i
t
h
y
o
u
r
j
o
b
s
i
t
u
a
t
i
o
n
?
T
r
e
a
t
m
e
n
t
e
p
i
s
o
d
e
-
r
e
f
e
r
s
t
o
t
h
e
p
e
r
i
o
d
o
f
t
i
m
e
a
p
e
r
s
o
n
i
s
r
e
c
e
i
v
i
n
g
t
r
e
a
t
m
e
n
t
(
f
r
o
m
t
h
e
i
n
i
t
i
a
l
D
I
A
L
O
G
s
c
o
r
e
t
o
t
h
e
l
a
s
t
D
I
A
L
O
G
s
c
o
r
e
)
.
G
l
o
b
a
l
s
c
o
r
e
-
r
e
f
e
r
s
t
o
t
h
e
t
o
t
a
l
D
I
A
L
O
G
s
c
o
r
e
s
r
a
t
h
e
r
t
h
a
n
s
i
n
g
l
e
i
t
e
m
s
H
o
w
t
o
u
s
e
D
I
A
L
O
G
o
n
E
l
e
c
t
r
o
n
i
c
P
a
t
i
e
n
t
R
e
c
o
r
d
s
(
E
P
R
)
s
y
s
t
e
m
s
[
P
l
a
c
e
h
o
l
d
e
r
]
Trusts to add in EPR information e.g.
screenshots and instructions of how to
navigate your EPR system in relation to
DIALOG
U
s
i
n
g
D
I
A
L
O
G
+
i
n
t
h
e
c
a
r
e
p
l
a
n
[
P
l
a
c
e
h
o
l
d
e
r
]
Trust might want to add examples of their
care plans.
•
DIALOG can improve the care
planning process.
•
Where Trusts move towards DIALOG+
there may be an opportunity to
streamline this process.
DIALOG is a valuable tool encompassing 11 questions covering various life areas, aiming to enhance person-centered care. Users rate their satisfaction levels across different domains, facilitating meaningful conversations with healthcare professionals. DIALOG+ further enhances interventions through a solution-focused therapy approach. The package emphasizes user feedback, outcome measurement, care planning, and recovery principles, promoting holistic recovery and well-being in London's healthcare context.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
DIALOG Pan London Training package
Section 3 Section 1 Section 2 What is DIALOG? Useful examples of how data is starting to be used Service user feedback on DIALOG and DIALOG+ How to rate DIALOG DIALOG+ Analysing DIALOG data When should DIALOG be completed? How to use DIALOG on EPR DIALOG as an outcome measure Using DIALOG+ in the care plan Why DIALOG was agreed as the London PROM Recovery principles Reflection exercise
What is DIALOG? DIALOG is a set of 11 simple questions that cover different areas of a person s life. Relationships with friends and family Meeting with your mental health professional Practical help you receive Accommodation Medication Mental health Physical health Leisure activities Personal safety Job Friendships situation
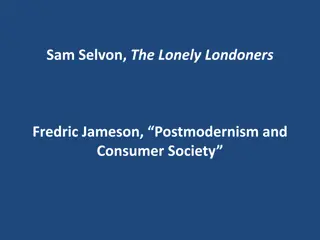
Section 1 How to rate DIALOG How satisfied are you with . 1. Your mental health? 2. Your physical health? 3. Your job situation? 4. Your accommodation? 5. Your leisure activities? 6. Your relationships with your partner/family? 7. Your friendships? 8. Your personal safety? 9. Your medication? 10.he practical help you receive? 11.Your meeting with your mental health professionals? How satisfied are you with your mental health? How satisfied are you with your physical health? The first eight questions cover different areas of a persons life- these are referred to as life domains How satisfied are you with your job situation? How satisfied are you with your accommodation? How satisfied are you with your leisure activities? How satisfied are you with your relationships with your partner/family? How satisfied are you with your friendships? How satisfied are you with your personal safety? and the last three are about your treatment- these are referred to as treatment domains How satisfied are you with your medication? How satisfied are you with the practical help you receive? How satisfied are you with your meetings with mental health professionals? DIALOG can help facilitate a person-centred approach by supporting meaningful conversations between service users and the healthcare professional about what aspects of their lives are important to them.
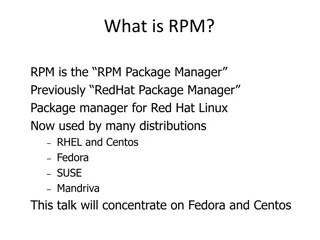
How to rate DIALOG with 1 being totally dissatisfied and 7 being totally satisfied. The survey is designed to measure how a person rates their quality of life and experience of the care that they receive. Fairly satisfied Totally satisfied Totally dissatisfied Fairly dissatisfied 2 Very 6 Very satisfied 1 7 3 4 5 In the middle dissatisfied Scores: 1-3 explicit dissatisfaction, 4 neutral middle, 5-7 explicit satisfaction
DIALOG + DIALOG+ is a specific intervention that uses the DIALOG scale and a 4- step approach based on solution focused therapy. DIALOG+ uses the scores identified by the person to help structure a conversation between the healthcare professional and the person to explore their identified needs and wishes, support care planning, and help service users take an active problem-solving approach to promoting recovery. DIALOG+ uses a 4 step approach 4. Agreeing on actions Agreeing on defined actions to improve the patient s condition and/or social situation. This step involves an agreement on specific and defined actions from the patient or the healthcare professional or both. The agreed actions are briefly documented. 3. Exploring options 2. Looking forward Asking the patient about what practical actions might help to bring about the desired change. This covers actions taken by the patient, the healthcare professional or someone else. Directing the patient from a description of the problem to considering desired alternative scenarios. The patient is asked to imagine what changes he/she would like to see to replace the current undesirable situation. This can focus on long-term preferred outcomes and more short term small changes. 1. Understanding Exploring both positive and negative aspects of the situation in the given domain. The person is first asked to explain the reasons for dissatisfaction and wishes for more help (or distress/concern in case of MH). Then the person is encouraged to consider existing strengths or coping strategies. To find out more information see the Operational Manual
When should DIALOG be completed? London has agreed minimum time points in which DIALOG should be completed to ensure a standardised process. Every 4 weeks for acutetreatment inpatients and crisis teams. No longer than 6 months for ongoing treatment in community services and outpatient clinics. At the start of a new treatment episode i.e. admission to an inpatient treatment, home treatment service, or other community service; referral to new provider organisation.) Review For acute treatment DIALOG should be carried out within 48 hours. For community settings it should be obtained within the first or second meeting Episode start More frequent DIALOGs maybe carried out if embedded within Care Programme Approach (CPA) process or when carrying out DIALOG is clinically indicated. At the end of treatment episode (discharge from a team, service or provider organisation). Episode end
DIALOG as an outcome measure PROMs provide services with a measure of the subjective impact of the services on a person s health and wellbeing. Healthcare professionals call this a patient reported outcome measure (PROM). It is an assessment of health status and health- related quality of life that comes directly from the patient. In London DIALOG has been agreed to be used for Early Intervention in Psychosis (EIP) and Care Programme Approach (CPA) services. DIALOG can be used in wider mental health service in the future.
Why has DIALOG been chosen as the London Patient Reported Outcome Measure (PROM)? London mental health partners came together to agree that DIALOG should be the London Patient Reported Outcome Measure (PROM). DIALOG was agreed to be used because .. The information can be used for planning for individual patients and whole services. The scale has been shown to have good psychometric properties. It is simple to use. It can be used to evaluate treatment and has the advantage that each item is meaningful. The use of DIALOG + has been shown to improve quality of life through a solution focused approach. Service users report satisfaction in using it.
Recovery Principles: CHIME framework The CHIME framework is a conceptual framework for personal recovery in mental health. It stands for Connectedness, Hope, Identity, Meaningful and Empowerment. This framework can complement the DIALOG approach. Connectedness Hope & Optimism Having good relationships and being connected to other people in positive ways. Characterised by: peer support and support groups; support from others; community. Having hope and optimism that recovery is possible and relationships that support this. Characterised by: motivation to change; positive thinking and valuing success; having dreams and aspirations Empowerment Identity Having control over life, focusing on strengths, and taking personal responsibility. Regaining a positive sense of self and identity and overcoming stigma. Meaningful Living a meaningful and purposeful life, as defined by the person (not others). Characterised by: meaning in mental illness experience ; spirituality; meaningful life and social goals. Source: Leamy et al 2011
Optional Personal Reflection Exercise for trainees 1/2 We are now going to undertake a short exercise that helps put the recovery principles into context Step 1 Fold a piece of paper in 4 Step 2 On each quarter put aspects of your life that represent how you and others see you i.e. mother, friend etc (This is not for sharing unless you wish to do so). Step 3 Group reflection 12 Trainers: please see facilitation prompts within the notes section of the slides
Service user feedback on DIALOG and DIALOG+ Service users have described the benefits of using DIALOG and DIALOG+ Watch this short video to hear what service users who have used DIALOG think Monitor [Placeholder] We recommend that Trusts co-deliver the training with service users, with service users reflecting on their own experience of how DIALOG/DIALOG+ has supported them. In the initial delivery of training Trusts may not be able have a pool of service users to co deliver sessions. They may wish to play the service user vignette video or the Pat Deegan video
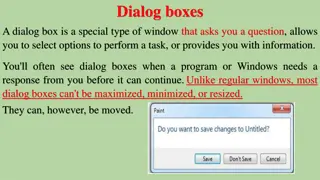
The data can be understood at an individual level. These charts shows how individual DIALOG question categories can be viewed to explore trends over time. The example is over a 10-month period. Useful examples of how DIALOG data is starting to be used There are different ways that DIALOG data can be understood and used to support a person s mental health and improve the quality of the service. The data can be used to better understand team needs. The data shows other aspects of people s lives that they are dissatisfied with, beyond their mental health, such as physical health, job situation and leisure activities. This can be used to direct focus around patients needs or for example staff skills and expertise. Source: This data is anonymised data taken from East London NHS Foundation Trust
Each of the DIALOG questions are rated using a Likert scale from 1 (totally dissatisfied) 7 (totally satisfied). Analysing DIALOG data Subjective quality of life The first eight DIALOG questions rate the satisfaction levels within different areas of life e.g accommodation. The mean score of all eight questions gives an overall score of subjective quality of life as a Patient Rated Outcome Measure (PROM). Treatment domains The final three items ask to rate different aspects of treatment. The mean score of the last three question gives an overall score for treatment satisfaction as a Patient Reported Experience Measure (PREM). When analysing the difference between scores over two timepoints it is important to acknowledge the initial score to understand the overall scope for improvement in satisfaction. When evaluating treatment episode satisfaction the change score should be considered to understand if subjective quality of life has improved. Either mean scores across the eight rated life domains or ratings of single life domains can be selected. This may depend on the focus, and context of care, the situation of the patients and the purpose of the evaluation. A high initial score = less room for improvement A low score = improvement is more likely When evaluating satisfaction of the treatment episode the most recent score given during the current treatment period is most relevant than changes over time. *Treatment episode- refers to the period of time a person is receiving treatment (from the initial DIALOG score to the last DIALOG score).
Analysing DIALOG data DIALOG data can be analysed at an individual item level or represented as mean scores for the team, service or organisation. The below information should be read in conjunction with the analytical framework. Organisation Individual Service The data can be viewed in different ways- Scores of single domains (DIALOG questions) of people in a service can be shown as means (average satisfaction scores) or as a % of patients who have explicit dissatisfaction/satisfaction. Mean team scores allow for review of data across every item. Used for an assessment of personal problems and areas of strength. Follows same principles as the interpretation for all patients in a service. For subjective quality of life scores below 4 (explicit dissatisfaction) require particular attention. When evaluating data at an organisation level the patient groups become very large, this means that the differences between the mean scores tend to become smaller therefore percentages of explicit dissatisfaction or very satisfied become more informative than mean scores. When considering changes over time, global mean scores as well as single can be used depending on the purpose For example if one evaluates full services with variable treatment tasks for a range of patients, it is reasonable to explore first the global scores before considering the ratings of single life domains. This applies to most services in most situations. However, there may also be specific questions, e.g. on how services affect the wide spread dissatisfaction of patients with their physical health. When evaluating treatment episode, any improvement in subjective quality of life is a meaningful increase. Analysing the global score provides a general evaluation, whilst the analysis of single domains provides more specific information about what exactly services do and do not achieve. When interpreting scores: The average subjective quality of life score of ALL patients in a service should not improve as patients with better quality of life will be discharged and new patients with lower quality of life be admitted, yet when you look at individual scores improvements should be expected. A change of overall mean scores of >0.125 reflects an average improvement of at least one scale point in at least one life domain (question) and may be a guide for overall meaningful improvement. Ideally treatment satisfaction scores should consistently stay above 4 and the % of patients with dissatisfaction <4 kept to a minimum For service users receiving long term care it is unrealistic to expect consistent and ongoing improvements; understanding personal context is important. Domain- refers to the individual DIALOG question e.g How satisfied are you with your job situation? Treatment episode- refers to the period of time a person is receiving treatment (from the initial DIALOG score to the last DIALOG score). Global score- refers to the total DIALOG scores rather than single items
How to use DIALOG on Electronic Patient Records (EPR) systems [Placeholder] Trusts to add in EPR information e.g. screenshots and instructions of how to navigate your EPR system in relation to DIALOG
Using DIALOG+ in the care plan [Placeholder] Trust might want to add examples of their care plans. DIALOG can improve the care planning process. Where Trusts move towards DIALOG+ there may be an opportunity to streamline this process.


















")