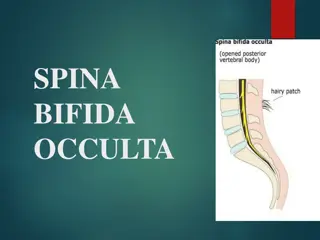
Commonly Tested Neurological Presentations
PACES Neuro
Wang Zhemin
What is commonly Tested?
•
Cranial Nerves: Single nerves (3,6,7), clubs, non-conforming
(meningeal/BOS/H&N tumours), complex ophthalmoplegia,
bulbar/pseudobulbar palsy, Horner’s, VF defects
•
Upper Limbs: Parkinsonism, cerebellar, myelopathy, bilat LL LMN
(muscle
–
FSHD/MD, NMJ - MG, nerve
–
CMT/DM, AHC - MND), LMN
monoparesis (Median/Ulnar/Radial/Mixed, Radiculopathy,
Plexopathy)
•
Lower Limbs: LMN LL (rmb cauda equina pathologies), UMN LL, foot
drop
General Inspection/Screens
•
CN: Ptosis, dysconjugate gaze, facial nerve palsy, NGT, scars, voice
•
UL:
•
Inspect: Neck scars, wasting, abnormal posturing
•
Screen: Grip myotonia, scapular winging
•
LL:
•
Inspect: Gait aids/WC, IDC, wasting, scars, deformities
•
Screen: Ankle dorsiflexion
CN 3
•
Down and out pupil, impaired EOM, ptosis, pupillary dilation (+/-)
•
Check for intorsion for CN 4
–
look down and in
•
Medical (pupils spared) vs surgical (pupils involved)
–
peripheral
pupillomotor fibers
•
Screen: Pronator drift (Weber’s), cerebellar (Benedikt’s)
•
Causes
•
Medical: DM with microvasc ischemia, vasculitis, demyelinating, infiltrative
•
Surgical: Pcomm aneurysm, tumour, abscess
CN 6
•
Features: Impaired abduction
•
Screen: Fundoscopy (for papilloedema
–
false localising sign of raised
ICP)
•
Causes
•
Medical: Ischemia (DM, HTN), post viral (younger patients), vasculitis
•
Surgical: Any cause of raised ICP
–
Tumours, vascular (bleeds, CVT), BIH
CN 7
•
Features: Weakness of facial muscles; may have hyperacusis (motor branch to stapedius),
loss of taste (corda tympani)
•
LMN (lower and upper facial muscles weak), UMN (upper facial muscles spared)
•
Check for: Parotid enlargement/tenderness, vesicles in EAM (ramsay hunt),
mastoid/parotid scar, pronator drift
•
Causes of unilateral LMN palsy: Bell’s, ramsay hunt’s, ischemic, demyelinating, vasculitic,
infiltrative
•
Causes of bilateral LMN palsy:
•
True bilat facial nerve palsy: Sarcoidosis, Lyme disease, GBS
•
Bilat facial weakness: Myopathies (Myotonic dystrophy, FSHD)
•
Treatment
•
Bell’s Palsy: Pred 60mg OM x 1 week, Acyclovir 400mg 5x/day x 10 days (or valacyclovir 100mg TDS
x 1 week)
•
Ramsay Hunt: Acyclovir 800mg 5x/day x 7 days; no steroids
Clubs
•
Orbital apex/SOF (if 2 involved then orbital apex): 2, 3, 4, 5i, 6
•
Causes: Tumours (meningioma, hemangioma), vasculitis (Wegeners/churg strauss),
infiltrative (sarcoid), infectious (abscesses), trauma
•
Cavernous sinus: 3, 4, 5 i and ii, 6; can have horner’s
•
Causes: Carotid-cavernous fistula, carotid aneurysm, tumour, thrombosis
•
Cerebellopontine angle: 5/6/7/8, cerebellum
•
Acoustic neuroma, meningioma, cholesteatoma
•
Jugular foramen: 9-11
•
Tumours (Glomus tumour, meningioma, schwannoma), infiltrative (lymphoma, sarcoid),
thombosis
•
Lateral medullary syndrome (post commonly affected is the posterior inferior
cerebellar artery)
•
Ipsilateral: Sympathetic (Horner’s), Cerebellar, Sensory nucleus of V, 8/9/10 also involved
•
Contralateral: Spinothalamic
Multiple CNs
–
Cranial Nerve Rules of 4
•
All CNs originate from the brainstem, except 1 & 2
•
CNs are grouped together at certain locations (clubs)
•
All CNs pass through meninges/base of skull: Meningeal (infective,
neoplastic, infiltrative), base of skull (trauma, neoplastic)
•
CNs may be affected by systemic disorders
: Muscle, NMJ, peripheral
nerves, AHC
Complex Ophthalmoplegia
Causes
•
Central: MS (INO
–
check convergence
, one and a half), NMO, PSP, Parinaud
(midbrain)
•
Nerve: MF, GBS, Mononeritis Multiplex
•
NMJ: MG
•
Muscle: Thyroid, CPEO (mitochondrial myopathy)
•
Melanoma with glass eye
•
Predominant Upgaze: PSP (downgaze affected first, check vestibulo-occular
reflex), Parinaud syndrome (upgaze affected first)
Additional Steps
Cerebellar (MS, MF), reflexes (areflexia in MF, hyperreflexia in MG), neck
flexion/fatigueability of arm (MG), tone/bradykinesia (PSP)
Bulbar/Pseudobulbar Palsy
Differentiating Features
•
Speech: Bulbar (nasal) vs pseudobulbar (hot-potato)
•
Tongue: Bulbar (fasciculations, wasted), pseudobulbar (spastic)
•
Jaw jerk: Bulbar (hyporeflexic), pseudobulbar (hyperreflexic)
Causes
•
Pseudobulbar: Stroke, SOL, dyelinating, trauma, MND
•
Bulbar: Causes of LMN pathology
–
Screen fatigueability (MG),
cerebellar (MF), reflexes, sensation (GBS)
Horner’s
•
Features: Ptosis, miosis, anhidrosis
•
Causes
•
1
st
order: LMS, syringomyelia/bulbia
•
2
nd
order: Pancoast tumour, neck pathology (masses, thyroid, scars)
•
3
rd
order: Cavernous sinus, internal carotid dissection
•
Examination: Cerebellar (LMS), UL sensation (syringomyelia), neck
examination (scars, lymph nodes, masses, bruit), hand examination
(wasting), lung examination (pancoast tumour)
•
Invx
•
Confirm: Cocaine test
•
Localise: Hydroxyamphetamine test (dilation = preganglionic lesion)
•
Scans: Brain, neck, thorax
Ptosis
•
Muscle: CPEO, myotonic dystrophy
•
NMJ: MG
•
Nerve: CN3 (dilated pupil
–
if surgical)
•
Others: Horner’s (constricted pupil)
•
Ptosis + Ophthalmoplegia: Muscle (mitochondrial myopathy, CPEO),
NMJ disorder, CN3 pathology
Visual Field Defect
•
Monocular: Eye, Retinal, Optic Nerve
•
Bitemporal Hemianopia: Compress from above and affect lower fields
first (craniopharyngioma), Compress from below and affect upper
fields first (Pituitary, suprasellar meningioma)
•
Homonymous Hemianopia: Retrochiasmal (contralateral side)
•
Macular Sparing: Occipital Lobe
•
Homonymous Quandrantopia (TIPS)
•
Temporal Lobe = Inferior
•
Parietal Lobe = Superior
Parkinsonism
•
Cardinal Features: Rest tremor, rigidity, bradykinesia (hands and feet),
postural instability
•
Additional Examination
•
MSA: Cerebellar, pyramidal weakness, check for IDC
•
PSP: Eye movements
•
Corticobasal degneration: Comb hair action
•
Function: Open bottle, writing (micrographia)
•
Offer: Drug/sleep/mood history, MMSE, postural BP, smell
Cerebellar
•
Unilateral:
•
Causes: Stroke, SOL, MS, Trauma
•
Extra: Pronator drift (ataxic hemiparesis), eye movements/pupillary reaction
(MS), CPA/LMS features
•
Bilateral
•
Causes: Congenital (inherited ataxias), metabolic (alcohol), drug (AEDs,
lithium, chemo, tacrolimus), infectious (meningoencephalitis, post infectious
cerebellitis), autoimmune (MS, MF, SLE), paraneoplastic, others (hypothyroid)
•
Extra:
•
Eye movement/pupillary reaction (MS), LL involvement (inherited ataxias), reflexes
(UMN – MS, ataxic hemiparesis, spinocerebellar ataxia, LMN – MF, Friedrich’s
), tone
(MSA)
•
Gingival hypertrophy (phenytoin), parotidomegaly (alcohol)
Myelopathy
•
Localisation: Level and portion of cord (ant, post, central)
•
Causes: Based on demographic, nature of cord involvement
•
Young: Congenital (HSP), Demyelinating (MS, transverse myelitis, NMO),
trauma
•
Old: Degenerative (DDD), neoplastic (primary/mets)
•
Posterior Column: SCAD, Tabes dorsalis, Friedrich’s Ataxia
•
Anterior Column: Anterior spinal infarction
•
Central Cord (UL > LL involvement, suspended sensory level to pinprick,
preserved proprioception, may have horners, may have distal UMN signs):
Syringomyelia, intramedullar tumours
Symmetrical LMN Weakness
•
Key distinguishing features: Sensory involvement, proximal vs distal
•
Muscle:
•
Proximal: FSHD, DMD/BMD, Cushing’s, DM/PM
•
Distal: Myotonic Dystrophy, Inclusion Body Myositis
•
NMJ: Fatigueability
•
Myasthenia Gravis
•
Peripheral Nerves: Typically distal involvement with sensory
component; but variable
•
Anterior Horn Cell: Wasting, fasciculations
Myopathies
•
FSHD
•
Cardinal Features: Scapular winging, proximal myopathy; facial weakness,
peroneal weakness
•
Associated Features: Cardiomyopathy, hearing loss, cognitive impairment
•
Myotonic Dystrophy
•
Cardinal Features: Grip myotonia, percussion myotonia, eye closure myotonia
•
Associated Features: Cardiomyopathy, DM, hypogonadism, cataracts, hearing
loss
Myasthenia Gravis
•
Cardinal Features: Fatigueable ptosis, complex opthalmoplegia, bulbar
involvement, limb involvement
•
Examination: Eye (shine torch, elevate eyelid, count from 1-20), upper
limbs (continuous or intermittent fatiguing)
•
Investigations:
•
Immediate: NIF
–
if < 20cmH2O consider respiratory support
•
Bedside: Ice pack test
•
Neurophysiological studies: Single fiber EMG (jitter pattern), repetitive nerve
stimulation (decremental pattern)
•
Antibodies: Acetylcholine Receptor or Muscle Specific Kinase (MuSK) antibodies;
New abs Agrin and LRP4
•
Management: Acute (ABC, PLEX/IVIG), Long term (pyridostigmine,
immunomodulators, thymectomy)
Peripheral Neuropathy
•
Causes:
•
D, A-J: Diabetes, Alcohol, B12/folate, Cancer, Drugs (isoniazid, cisplatin,
amiodarone, phenytoin, dapsone), Environmental (Lead), Familial (CMT),
GBS/CIDP, Hypothyroid, Infections (HIV, Lyme), sJogrens
•
Motor Predominant: AIDP/CIDP, MMN, Lead toxicity, Diabetic amyotrophy,
drugs (dapsone), critical care neuropathy, porphyria
•
Sensory Neuronopathy (dysasthesiae, asymmetrical sensory loss, ataxia,
absent reflexes, no motor loss): Paraneoplastic, Sjogren’s, Drugs
(chemotherapy)
•
Specific Antibodies
•
Multifocal Motor Neuropathy: Anti GM1 antibody
•
Paraneoplastic: Anti Hu and Yo
Median Nerve
•
Inspection: Scars, thenar wasting
•
Motor: Benediction sign on hand closure (proximal lesion), weakness
of thumb abduction, weakness of radial 2 DIPJ flexion (proximal
lesion)
•
Sensation: Radial 3.5 fingers affected, thenar eminence affeted
(proximal lesion)
•
Special Tests: Phalen’s (CTS), O-sign (AIN), Tinel’s
Ulnar Nerve
•
Inspection: Interossei guttering, hypothenar wasting, ulnar claw
(distal lesion)
•
Motor: Weakness of finger abduction, weakness of ulnar 2 DIPJ
flexion (proximal lesion)
•
Sensation: Ulnar 1.5 fingers affected, volar and dorsal ulnar aspects
affected in proximal lesions
•
Special Tests: Froment’s
•
Sites: Distal (Guyon’s canal), Proximal (Cubital tunnel syndrome)
Radial Nerve
•
Inspection: Wrist drop, finger drop
•
Motor: Finger extension (specifically MCPJ, extension can still occur at
IPJ because supplied by intrinsic muscles), wrist extension (spared for
PIN pathology), elbow extension, supination, test triceps jerk too
•
Sensation: Anatomical snuffbox (spared in PIN pathology)
•
Level of injury: Axilla (crutches, Saturday night palsy), humeral shaft,
elbow (fracture, dislocation)
•
Differential would be C7 radiculopathy which has additional features
of weak shoulder adduction and wrist flexion
Foot Drop
•
Motor
•
Foot inversion: Affected suggests L4/5 or sciatic nerve
•
Hip abduction and internal rotation: Affected suggests L4/5
•
Reflexes: Ankle jerks lost in sciatic nerve or S1 radiculopathy
•
Sensory
•
Deep br of common peroneal: only 1
st
webspace
•
Common peroneal: 1
st
webspace, dorsum of foot, lateral calf
•
Sciatic (L4/5/S1 dermatomes): whole leg
•
L4/5: sensation of foot dorsum and lateral calf,
extending to lateral side of leg
•
Etiology: Check for scars, palpate peroneal nerve, SLR/check spine
This content discusses commonly tested neurological presentations focusing on Cranial Nerves, Upper Limbs, Lower Limbs, General Inspections, and specific features of CN 3, 6, and 7. It covers signs, symptoms, causes, and treatment options for various neurological conditions to aid in clinical assessment.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
PACES Neuro Wang Zhemin
What is commonly Tested? Cranial Nerves: Single nerves (3,6,7), clubs, non-conforming (meningeal/BOS/H&N tumours), complex ophthalmoplegia, bulbar/pseudobulbar palsy, Horner s, VF defects Upper Limbs: Parkinsonism, cerebellar, myelopathy, bilat LL LMN (muscle FSHD/MD, NMJ - MG, nerve CMT/DM, AHC - MND), LMN monoparesis (Median/Ulnar/Radial/Mixed, Radiculopathy, Plexopathy) Lower Limbs: LMN LL (rmb cauda equina pathologies), UMN LL, foot drop
General Inspection/Screens CN: Ptosis, dysconjugate gaze, facial nerve palsy, NGT, scars, voice UL: Inspect: Neck scars, wasting, abnormal posturing Screen: Grip myotonia, scapular winging LL: Inspect: Gait aids/WC, IDC, wasting, scars, deformities Screen: Ankle dorsiflexion
CN 3 Down and out pupil, impaired EOM, ptosis, pupillary dilation (+/-) Check for intorsion for CN 4 look down and in Medical (pupils spared) vs surgical (pupils involved) peripheral pupillomotor fibers Screen: Pronator drift (Weber s), cerebellar (Benedikt s) Causes Medical: DM with microvasc ischemia, vasculitis, demyelinating, infiltrative Surgical: Pcomm aneurysm, tumour, abscess
CN 6 Features: Impaired abduction Screen: Fundoscopy (for papilloedema false localising sign of raised ICP) Causes Medical: Ischemia (DM, HTN), post viral (younger patients), vasculitis Surgical: Any cause of raised ICP Tumours, vascular (bleeds, CVT), BIH
CN 7 Features: Weakness of facial muscles; may have hyperacusis (motor branch to stapedius), loss of taste (corda tympani) LMN (lower and upper facial muscles weak), UMN (upper facial muscles spared) Check for: Parotid enlargement/tenderness, vesicles in EAM (ramsay hunt), mastoid/parotid scar, pronator drift Causes of unilateral LMN palsy: Bell s, ramsay hunt s, ischemic, demyelinating, vasculitic, infiltrative Causes of bilateral LMN palsy: True bilat facial nerve palsy: Sarcoidosis, Lyme disease, GBS Bilat facial weakness: Myopathies (Myotonic dystrophy, FSHD) Treatment Bell s Palsy: Pred 60mg OM x 1 week, Acyclovir 400mg 5x/day x 10 days (or valacyclovir 100mg TDS x 1 week) Ramsay Hunt: Acyclovir 800mg 5x/day x 7 days; no steroids
Clubs Orbital apex/SOF (if 2 involved then orbital apex): 2, 3, 4, 5i, 6 Causes: Tumours (meningioma, hemangioma), vasculitis (Wegeners/churg strauss), infiltrative (sarcoid), infectious (abscesses), trauma Cavernous sinus: 3, 4, 5 i and ii, 6; can have horner s Causes: Carotid-cavernous fistula, carotid aneurysm, tumour, thrombosis Cerebellopontine angle: 5/6/7/8, cerebellum Acoustic neuroma, meningioma, cholesteatoma Jugular foramen: 9-11 Tumours (Glomus tumour, meningioma, schwannoma), infiltrative (lymphoma, sarcoid), thombosis Lateral medullary syndrome (post commonly affected is the posterior inferior cerebellar artery) Ipsilateral: Sympathetic (Horner s), Cerebellar, Sensory nucleus of V, 8/9/10 also involved Contralateral: Spinothalamic
Multiple CNs Cranial Nerve Rules of 4 All CNs originate from the brainstem, except 1 & 2 CNs are grouped together at certain locations (clubs) All CNs pass through meninges/base of skull: Meningeal (infective, neoplastic, infiltrative), base of skull (trauma, neoplastic) CNs may be affected by systemic disorders: Muscle, NMJ, peripheral nerves, AHC
Complex Ophthalmoplegia Causes Central: MS (INO check convergence, one and a half), NMO, PSP, Parinaud (midbrain) Nerve: MF, GBS, Mononeritis Multiplex NMJ: MG Muscle: Thyroid, CPEO (mitochondrial myopathy) Melanoma with glass eye Predominant Upgaze: PSP (downgaze affected first, check vestibulo-occular reflex), Parinaud syndrome (upgaze affected first) Additional Steps Cerebellar (MS, MF), reflexes (areflexia in MF, hyperreflexia in MG), neck flexion/fatigueability of arm (MG), tone/bradykinesia (PSP)
Bulbar/Pseudobulbar Palsy Differentiating Features Speech: Bulbar (nasal) vs pseudobulbar (hot-potato) Tongue: Bulbar (fasciculations, wasted), pseudobulbar (spastic) Jaw jerk: Bulbar (hyporeflexic), pseudobulbar (hyperreflexic) Causes Pseudobulbar: Stroke, SOL, dyelinating, trauma, MND Bulbar: Causes of LMN pathology Screen fatigueability (MG), cerebellar (MF), reflexes, sensation (GBS)
Horners Features: Ptosis, miosis, anhidrosis Causes 1storder: LMS, syringomyelia/bulbia 2ndorder: Pancoast tumour, neck pathology (masses, thyroid, scars) 3rdorder: Cavernous sinus, internal carotid dissection Examination: Cerebellar (LMS), UL sensation (syringomyelia), neck examination (scars, lymph nodes, masses, bruit), hand examination (wasting), lung examination (pancoast tumour) Invx Confirm: Cocaine test Localise: Hydroxyamphetamine test (dilation = preganglionic lesion) Scans: Brain, neck, thorax
Ptosis Muscle: CPEO, myotonic dystrophy NMJ: MG Nerve: CN3 (dilated pupil if surgical) Others: Horner s (constricted pupil) Ptosis + Ophthalmoplegia: Muscle (mitochondrial myopathy, CPEO), NMJ disorder, CN3 pathology
Visual Field Defect Monocular: Eye, Retinal, Optic Nerve Bitemporal Hemianopia: Compress from above and affect lower fields first (craniopharyngioma), Compress from below and affect upper fields first (Pituitary, suprasellar meningioma) Homonymous Hemianopia: Retrochiasmal (contralateral side) Macular Sparing: Occipital Lobe Homonymous Quandrantopia (TIPS) Temporal Lobe = Inferior Parietal Lobe = Superior
Parkinsonism Cardinal Features: Rest tremor, rigidity, bradykinesia (hands and feet), postural instability Additional Examination MSA: Cerebellar, pyramidal weakness, check for IDC PSP: Eye movements Corticobasal degneration: Comb hair action Function: Open bottle, writing (micrographia) Offer: Drug/sleep/mood history, MMSE, postural BP, smell
Cerebellar Unilateral: Causes: Stroke, SOL, MS, Trauma Extra: Pronator drift (ataxic hemiparesis), eye movements/pupillary reaction (MS), CPA/LMS features Bilateral Causes: Congenital (inherited ataxias), metabolic (alcohol), drug (AEDs, lithium, chemo, tacrolimus), infectious (meningoencephalitis, post infectious cerebellitis), autoimmune (MS, MF, SLE), paraneoplastic, others (hypothyroid) Extra: Eye movement/pupillary reaction (MS), LL involvement (inherited ataxias), reflexes (UMN MS, ataxic hemiparesis, spinocerebellar ataxia, LMN MF, Friedrich s), tone (MSA) Gingival hypertrophy (phenytoin), parotidomegaly (alcohol)
Myelopathy Localisation: Level and portion of cord (ant, post, central) Causes: Based on demographic, nature of cord involvement Young: Congenital (HSP), Demyelinating (MS, transverse myelitis, NMO), trauma Old: Degenerative (DDD), neoplastic (primary/mets) Posterior Column: SCAD, Tabes dorsalis, Friedrich s Ataxia Anterior Column: Anterior spinal infarction Central Cord (UL > LL involvement, suspended sensory level to pinprick, preserved proprioception, may have horners, may have distal UMN signs): Syringomyelia, intramedullar tumours
Symmetrical LMN Weakness Key distinguishing features: Sensory involvement, proximal vs distal Muscle: Proximal: FSHD, DMD/BMD, Cushing s, DM/PM Distal: Myotonic Dystrophy, Inclusion Body Myositis NMJ: Fatigueability Myasthenia Gravis Peripheral Nerves: Typically distal involvement with sensory component; but variable Anterior Horn Cell: Wasting, fasciculations
Myopathies FSHD Cardinal Features: Scapular winging, proximal myopathy; facial weakness, peroneal weakness Associated Features: Cardiomyopathy, hearing loss, cognitive impairment Myotonic Dystrophy Cardinal Features: Grip myotonia, percussion myotonia, eye closure myotonia Associated Features: Cardiomyopathy, DM, hypogonadism, cataracts, hearing loss
Myasthenia Gravis Cardinal Features: Fatigueable ptosis, complex opthalmoplegia, bulbar involvement, limb involvement Examination: Eye (shine torch, elevate eyelid, count from 1-20), upper limbs (continuous or intermittent fatiguing) Investigations: Immediate: NIF if < 20cmH2O consider respiratory support Bedside: Ice pack test Neurophysiological studies: Single fiber EMG (jitter pattern), repetitive nerve stimulation (decremental pattern) Antibodies: Acetylcholine Receptor or Muscle Specific Kinase (MuSK) antibodies; New abs Agrin and LRP4 Management: Acute (ABC, PLEX/IVIG), Long term (pyridostigmine, immunomodulators, thymectomy)
Peripheral Neuropathy Causes: D, A-J: Diabetes, Alcohol, B12/folate, Cancer, Drugs (isoniazid, cisplatin, amiodarone, phenytoin, dapsone), Environmental (Lead), Familial (CMT), GBS/CIDP, Hypothyroid, Infections (HIV, Lyme), sJogrens Motor Predominant: AIDP/CIDP, MMN, Lead toxicity, Diabetic amyotrophy, drugs (dapsone), critical care neuropathy, porphyria Sensory Neuronopathy (dysasthesiae, asymmetrical sensory loss, ataxia, absent reflexes, no motor loss): Paraneoplastic, Sjogren s, Drugs (chemotherapy) Specific Antibodies Multifocal Motor Neuropathy: Anti GM1 antibody Paraneoplastic: Anti Hu and Yo
Median Nerve Inspection: Scars, thenar wasting Motor: Benediction sign on hand closure (proximal lesion), weakness of thumb abduction, weakness of radial 2 DIPJ flexion (proximal lesion) Sensation: Radial 3.5 fingers affected, thenar eminence affeted (proximal lesion) Special Tests: Phalen s (CTS), O-sign (AIN), Tinel s
Ulnar Nerve Inspection: Interossei guttering, hypothenar wasting, ulnar claw (distal lesion) Motor: Weakness of finger abduction, weakness of ulnar 2 DIPJ flexion (proximal lesion) Sensation: Ulnar 1.5 fingers affected, volar and dorsal ulnar aspects affected in proximal lesions Special Tests: Froment s Sites: Distal (Guyon s canal), Proximal (Cubital tunnel syndrome)
Radial Nerve Inspection: Wrist drop, finger drop Motor: Finger extension (specifically MCPJ, extension can still occur at IPJ because supplied by intrinsic muscles), wrist extension (spared for PIN pathology), elbow extension, supination, test triceps jerk too Sensation: Anatomical snuffbox (spared in PIN pathology) Level of injury: Axilla (crutches, Saturday night palsy), humeral shaft, elbow (fracture, dislocation) Differential would be C7 radiculopathy which has additional features of weak shoulder adduction and wrist flexion
Foot Drop Motor Foot inversion: Affected suggests L4/5 or sciatic nerve Hip abduction and internal rotation: Affected suggests L4/5 Reflexes: Ankle jerks lost in sciatic nerve or S1 radiculopathy Sensory Deep br of common peroneal: only 1stwebspace Common peroneal: 1stwebspace, dorsum of foot, lateral calf Sciatic (L4/5/S1 dermatomes): whole leg L4/5: sensation of foot dorsum and lateral calf, extending to lateral side of leg Etiology: Check for scars, palpate peroneal nerve, SLR/check spine