Approach to Headache and Neurological Symptoms in Clinical Practice
Comprehensive overview of primary and secondary headaches, red flags, and patterns in neurological presentations. Discusses distinguishing features, differential diagnoses, and management approaches for various conditions affecting the central and peripheral nervous system. Highlights important conditions like cerebral venous sinus thrombosis, pituitary apoplexy, and giant cell arteritis.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
PACES Approaches Ep1: Neurology Approaches (I)
Content Headache Giddiness Loss of Consciousness Weakness/Lethargy
Approach Primary vs Secondary Red Flags Patterns: Raised ICP features, thunderclap, visual disturbances, hypertension Intracranial vs Extracranial (don t forget SYSTEMIC things like pheochromocytoma, OSA, hyperviscosity)
Primary Headaches Migraine Secondary Headaches Red Flags: Progressive, thunderclap (sudden onset, worst ever headache), raised ICP (cough, lying down), neurological symptoms, meningism (neck stiffness, photophobia, rash), constitutional symps (fever, LOW/LOA), extremities of age Intracranial Vascular (sudden): SAH (APKD), venous sinus thrombosis, pituitary apoplexy, carotid/vertebral artery dissection Infection: Meningitis, encephalitis, abscess Tumour: Primary, haematological malignancy, metastasis, pituitary (acromegaly) Others: Benign intracranial hypertension Extracranial GCA, sinusitis, glaucoma, dental Systemic Hypertension (pheochromocytoma, OSA) medication induced (analgesia, CCB, nitrates), hyperviscosity (polycythemia, haem malig) Preceding light flashes, abnormal smells Prefer dark room Cluster Unilateral tearing, rhinorrhea, droopy eyelid Tension Band like Stressors
Important Conditions Neuro: Cebebral venous sinus thrombosis (hypercoagulable states), BIH, SAH (b/g APKD) Endocrine: Pituitary apoplexy, pheochromocytoma, acromegaly Rheum: GCA Others: OSA
Patterns Hypertension: Pheochromocytoma, Hypertension causing HA, CCB use, Raised ICP with Cushing s reflex, Pituitary tumours with 2 endocrinopathy (acromegaly, cushing s) BOV: GCA, glaucoma, BIH, SOL with visual tract compromise (pituitary tumour, cerebral SOL) Thunderclap : SAH, cerebral venous sinus thrombosis, cervical artery dissection, reversible cerebral vasoconstriction syndromes Raised ICP features: SOL (rmb pituitary tumour), BIH, thrombosis/hemorrhage
Approach Big Groups: Vertiginous (central vs peripheral) Pre-Syncope (similar causes to syncope) Light-headedness Pre-syncope causes feature quite significantly Especially postural hypotension group (DM, Drugs, Autonomic, Adrenal Insufficiency, Anemia) Other conditions: Conduction defects (Ank spond, DM/PM, MD), NF2 with acoustic neuroma, hypoglycemia (adrenal insufficiency, MEN1)
Vertiginous: Spinning sensation Peripheral -BPPV, Vestibular neuronitis, Labyrinthitis, Meniere s, migrainous vertigo -Ear: Otitis media, ototoxic drugs (aminoglycosides) Acute vs chronic? Episodic vs first episode? Ear symptoms: Ringing in ears? Deafness? Fullness of ear? Neurological symptoms: Especially cerebellar (coordination) Central -Cerebellar: All causes, CPA, MS -Brainstem: VBI, posterior fossa infarction Acoustic neuroma (ask hearing loss, consider NF2) Chest pain, SOB, diaphoresis, palpitations Presyncope: Near black out? Improve with sitting/lying? Preceding cardio/neuro symptoms? Postural association? Cardiac -Aortic stenosis, AMI, HOCM, arrhythmias (brady, sick sinus, heart block, VT, QT prolong) PACES conditions that cause CMP/arrhythmia problems include muscle pathology (MD, DMD), Ank spond Sudden head movements, wearing tight collar? Vascular: Subclavian steal syndrome Neuro: -Carotid sinus hypersensitivity -Vasovagal, situational (cough, micturition, defecation) Oral intake. Polyuria/polydipsia? Tremors/slowing of movements? Hot environment, prolonged standing? TCM use Blood loss Orthostatic / Postural Hypotension: Dehydration Drugs Autonomic: DM, PD/MSA, LEM, GBS/CIDP Adrenal insufficiency Anemia Hypoglycemia (adrenal insufficiency, insulinoma in MEN) Any form of acute illness (electrolytes, sepsis) Light-headedness Missed meals? Do you have any fever? LOW/LOA
Approach Big Groups Seizures Consider neurocutaneous disorders Syncope Cardiogenic, vasovagal, subclavian steal (vasculitis) Others: Drop attacks, fell asleep, drowsiness Remember to consider counselling regarding driving/high risk activity
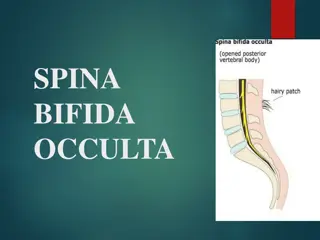
Seizures: Aura, jerking/tensing, up-rolling of eyes, frothing around mouth, tongue biting loss of bowel/urinary continence, post-ictal confusion, Todd s paralysis Syndromes: Sturge Weber, Tuberous sclerosis, Down s syndrome Acute: Infection, inflammation (SLE), electrolyte disturbances, drug overdose, vascular, uremic/hepatic encephalopathy, alcohol withdrawal Chronic: Any CNS insult Cardiac: Valve (aortic stenosis), arrhythmia (HOCM), underlying myopathy (Myotonic dystrophy, DMD/BMD, ank spond), arrhythmics (heart failure, congenital pathology like WPW, Brugada) Postural Hypotension: Hypovolemia, drugs, neurological disorder (DM, Parkinson s, GBS), adrenal insufficiency Vasosagal: Prolonged standing, emotion (fear), situational (micturition) Steal Syndrome: Triggered by upper limb activity Drop Attack: Meniere s, Cataplexy Fell Asleep: OSA CNS pathology: Infection, mets, vascular event Hypoglycemia Electrolytes: Hypercalcemia, Hypo/hypernatremia Drugs Opioids Uremia, hepatic encephalopathy, hypoxia/CO2 narcosis Syncope: Quick resolution following recumbency Cardiac: Chest pain, palpitations Exertion association (general exertion, upper limb exertion) Postural association Postural Hypotension: Precipitated by postural changes, fluid losses, medication Others: Drop attacks, fell asleep Drowsiness
Approach Important to ascertain if it is true weakness vs generalized lethargy/malaise If true weakness: Onset, persistent vs episodic Pattern: Distribution (which limbs? bulbar?), proximal vs distal Other neurological symptoms: Sensory, CN, extrapyramidal, cerebellar, autonomic For lethargy/malaise/fatigue group Endocrinopathies: Hypothyroid, adrenal insufficiency, panhypopit OSA Anemia Systemic diseases Muscle Pains: Myositis, PMR, fibromyalgia
Fatigue/ Lethargy Specific: OSA, anemia, heart failure, panhypopit, hypothyroidism, adrenal insufficiency, drugs (beta blockers), depression, chronic fatigue syndrome, fibromyalgia General: Cancer, chronic infections (HIV, TB), systemic diseases (liver, kidney dysfunction), autoimmune disorders (polymyalgia rheumatica, fibromyalgia) By Distribution: -Hemiparesis Pattern: Usually brain pathology (unless traumatic brown sequard) -Paraparesis Pattern: Usually spinal cord pathology (ask for bowel/urinary incont) -Quadri/Tetraparesis Pattern: Tends to be more non specific cord (neck pain/sensory level) vs LMN Weakness -Onset -Which limbs? -Proximal vs distal vs global -Sensation -Neck/ brainstem symptoms >Proximal Weakness Myopathy: Metabolic, Congenital, Rheum (Dermatomyositis, polymyositis), Endocrine (Grave s, Hypothyroidism, Cushing s, Acromegaly, Adrenal insufficiency), Neoplastic, Drugs NMJ: Myasthemia, Lambert Eaton (small cell lung ca) Anterior horn cell: MND GBS >Distal Weakness Peripheral neuropathies Episodic Weakness: Hypokalemic periodic paralysis, hemiplegia migraine, TIA, hypoglycemia