Advancements in Alzheimer Disease Therapeutics Program
The MGB Alzheimer Therapeutics
Program
Ushering in a new era of disease-modifying therapies for Alzheimer disease
Fall 2023
BWH, MGH Departments of Neurology
Collective effort over years
•
The plans presented reflect the tireless efforts of dozens of individuals over many years
•
Aducanumab working group
lecanemab working group
ATP
•
Weekly meetings for months; committees, logistical teams, multiple institutions, depts
•
Clinicians, clinical scientists, pharmacists, radiologists, nursing, administrators, staff, IT
•
The underlying scientific neurobiological models were pioneered here
•
The clinical science has been advanced here
•
Disease-modifying therapies, especially those targeting amyloid, has grown from a vision to a plan to
now a reality
•
This is a joyful moment – there is now an option for slowing down the progression of Alzheimer
disease
•
This is a moment of intense focus; ensuring success requires careful systems to ensure a safe,
efficacious, and equitable delivery
BWH, MGH Departments of Neurology
Lecanemab (Leqembi)
Outline
Lecanemab (Leqembi)
•
Dosing and administration
•
Clinical efficacy
•
Side effects: ARIA
Alzheimer Therapeutics Program (ATP)
•
Shared care model
•
Requirements before referring
•
How to refer in Epic
•
Emergency Department considerations
BWH, MGH Departments of Neurology
Lecanemab
•
Monoclonal antibody given as IV infusion every two weeks to remove amyloid plaques
•
Targets Ab oligomers and protofibrils, which are highly toxic
•
Amyloid hypothesis – that amyloid toxicity is central to the pathophysiology of AD
•
FDA approved for treating
mild cognitive impairment or mild dementia due to Alzheimer disease
•
Mild cognitive impairment (MCI)
: abnormal cognitive testing results, but full independence in
instrumental (e.g., household tasks; finances) and basic (e.g., bathing, dressing) activities of daily
living (ADLs)
•
Mild dementia
: abnormal cognitive testing results, some dependence in instrumental ADLs, but
full independence in basic ADLs
‒
Patients with any loss of independence in basic ADLs due to cognitive impairment have
moderate dementia and are not eligible for lecanemab
•
due to Alzheimer disease:
evidence of amyloid plaques in their brain by CSF biomarkers (lumbar
puncture) or by amyloid PET scan
BWH, MGH Departments of Neurology
•
Large, double-blind, placebo-controlled study
•
Who: 1766 pts across 245 sites, ~900 received
lecanemab
•
Diagnosis: mild cognitive impairment or mild
dementia
•
Cognitive: MMSE >21, with memory loss
•
Function: CDR global 0.5-1.0
•
Biological: positive amyloid-PET scan or CSF
markers
•
Excluded: people with bleeding in the brain,
others
•
Allowed anticoagulant use
Followed for 18 months
Lecanemab Phase 3 Trial: CLARITY AD
BWH, MGH Departments of Neurology
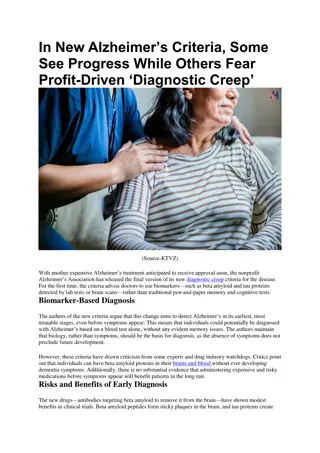
Lecanemab: Phase 3 Study Results
•
Placebo and lecanemab groups declined cognitively and functionally,
but lecanemab group declined ~27% less over 18 months
BWH, MGH Departments of Neurology
Van Dyck
et al.
(2023) New Engl J Med 388:9-21.
Clinical Dementia Rating – Sum of Boxes (primary outcome):
Activities of daily living (ADCS-MCI-ADL, secondary outcome):
Lecanemab: Phase 3 Study Results
•
Lecanemab removes amyloid effectively (PET)
•
Lecanemab improved biomarker profiles in CSF and blood
•
AD-specific: total and phosphorylated tau
•
Degenerative markers - neurogranin
BWH, MGH Departments of Neurology
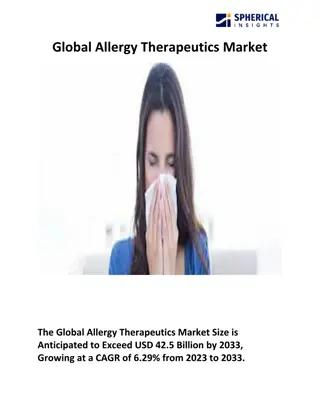
Lecanemab: Amyloid Related Imaging Abnormalities
(ARIA)
•
Focal areas of cerebral edema (ARAI-E) and associated
microhemorrhages (ARIA-H) occurring in patients on
lecanemab
•
Occurred in 13% of all lecanemab-treated clinical trial
patients
•
Highest risk in first 3-6 months
•
Mostly asymptomatic (>70% of ARIA)
•
Case reports of fatal or debilitating injury (risk <1%)
•
Risk factors for ARIA:
•
Pre-treatment brain microhemorrhages (visible on
MRI)
•
Having the ApoE gene
ε
4 allele (homozygotes >
heterozygotes > non-carriers)
•
Therapeutic anticoagulation
•
ARIA requires MRI monitoring
BWH, MGH Departments of Neurology
Alzheimer Therapeutic Program
~400 currently treated MGB patients
would meet criteria for lecanemab treatment,
plus ~600 new patients
with early AD evaluated
annually. The process for determining drug eligibility includes a focused history and physical exam, standardized cognitive screening
assessments, brain MRI, Alzheimer-specific biomarker testing (e.g., CSF testing or amyloid-PET), and APOE genetic testing.
Alzheimer Therapeutics Program (ATP) Overview
Safety Monitoring and Triage
Key Objectives
Screening and Eligibility
Determination
Collect Clinical Data
Coordinate the Work of
Interdisciplinary Provider Teams
A critical function of the ATP clinic is drug safety monitoring with neuroimaging and clinical assessments.
Patients will be triaged
and offered urgent
/ emergent visits to address any possible side effects.
The ATP will be a
collaboration
led by the Departments of Neurology at Massachusetts General Hospital (MGH) and Brigham and
Women’s Hospital (BWH), with appropriate partnerships with Geriatric Psychiatry, Pharmacy, Radiology, Nursing (Infusion), and the
Mind & Memory Care Program at MGB institutions; and many allied clinicians across MGB.
To support
quality improvement efforts
and
clinical research,
clinical data will be collected, monitored and tracked for the ATP clinic.
The ATP clinic will also contribute to a national registry to better understand the biological and clinical impact of anti-Alzheimer
drugs.
As future AD drugs come to market in the short term, this will be critical to the
successful depl
oyment of these drugs as well.
•
Shared provider model akin to anticoagulation management service (similar to a “Coumadin clinic”)
Responsible for administration and safety monitoring of lecanemab
Not responsible for other aspects of dementia care
(other memory medications, psychiatric care, community services,
etc.)
--Referring provider remains main resource for patient and family; ATP always available for lecanemab-specific concerns
--Typical cognitive and behavioral neurology referrals remain available for comprehensive cognitive
evaluations
•
The ATP has harmonized procedures across MGB, but BWH and MGH have separate referrals and physician
pools (for now)
Shared Service Model
•
On/Off call model - 1 week on
•
On-call provider takes care of much of the ATP activities:
•
Sees patients in clinic (starting out with 4-hour session per week)
•
Triages incoming referrals
•
Orders pending eligibility studies (CSF, APOE, etc)
•
Reviews MRIs for ARIA
•
Reviews and addresses patient messages/calls/emails
•
Makes decisions if/when to pause therapy plans based on MRI/symptoms
•
24-7 pager coverage for emergencies
•
Passes off active issues to incoming on-call provider
•
Supported by a growing administrative team
Requirements for ATP referral
1. Patient has
mild cognitive impairment
or
mild dementia
•
i.e.,
cognitive impairment does
not
affect basic activities of daily living (bathing, dressing, eating,
toileting, etc
.
)
2. Brief cognitive screening test within the past 6 months
•
Mini-mental State Exam (MMSE), Montreal Cognitive Assessment (MoCA), or St. Louis University
Mental Assessment (SLUMS)
•
Mini-cog
not sufficient
3. Brain MRI within the past year
4. Blood tests within the past 6 months: CBC, CMP, PT-INR, PTT, TSH, Vitamin B12
5. For now, full-strength anticoagulation is a strict contraindication for lecanemab
6. A continued follow-up plan with the referring provider
Alzheimer disease biomarkers (lumbar puncture or amyloid PET) and ApoE genotyping will be handled
by the ATP, but can be done in advance if referring provider is comfortable
When in doubt, please ask: mgbatp@mgb.org
BWH, MGH Departments of Neurology
BWH, MGH Departments of Neurology
A
T
P
c
l
i
n
i
c
i
a
n
s
w
i
l
l
r
e
v
i
e
w
a
v
a
i
l
a
b
l
e
r
e
f
e
r
r
a
l
i
n
f
o
r
m
a
t
i
o
n
t
o
d
e
t
e
r
m
i
n
e
i
f
t
h
e
p
a
t
i
e
n
t
m
a
y
m
e
e
t
e
l
i
g
i
b
i
l
i
t
y
c
r
i
t
e
r
i
a
,
a
n
d
w
h
a
t
w
o
r
k
u
p
r
e
m
a
i
n
s
w
i
t
h
i
n
t
h
e
A
T
P
:
•
Clinical diagnosis of AD-spectrum syndrome at severity of MCI or mild dementia
•
MoCA 15 or greater, MMSE 22 or greater, SLUMS 16 or greater within 6 months of referral (exceptions may be
considered)
•
Does not have clinical diagnosis of
Lewy body dementia
or frontotemporal dementia-spectrum syndrome
•
Is not on full-strength anticoagulation or immunosuppression
•
Does not have other poorly controlled chronic medical, neurological, or psychiatric conditions
•
Able to comply with infusion visits every 2 weeks
•
CMP, B12, TSH, CBC, PT, PTT within 6 months of referral without abnormalities requiring further investigation
•
MRI brain within 12 months of referral without exclusionary findings (>4 microbleeds, severe small vessel
disease, large vessel infarcts)
•
Elevated p-tau181/Abeta42 (Mayo Clinic labs), Abeta42/p-tau - 0.0105(t-tau) < 3.694 (Athena ADMark), or
amyloid PET suggesting elevated brain amyloid
•
APOE
genotyping
C
h
a
l
l
e
n
g
i
n
g
c
a
s
e
s
w
i
l
l
b
e
r
e
v
i
e
w
e
d
b
y
t
h
e
A
T
P
’
s
P
l
a
q
u
e
a
n
d
T
a
n
g
l
e
B
o
a
r
d
(
s
i
m
i
l
a
r
t
o
a
n
o
n
c
o
l
o
g
y
t
u
m
o
r
b
o
a
r
d
)
ATP lecanemab eligibility checklist
How to refer in Epic
BWH, MGH Departments of Neurology
After referral
•
ATP will screen chart and then contact patient
•
May contact referring provider instead if more workup is required before referral or if there is a
contraindication from chart review
•
Up to three ATP visits before starting lecanemab:
1.
Intake and eligibility
‒
Obtaining Alzheimer disease biomarkers (spinal fluid)
2.
Discussion of biomarker results, counseling and ordering genetic testing (ApoE)
3.
Review of ApoE; prescribing lecanemab
•
Lecanemab infusions at MGB sites every two weeks
•
Three additional safety monitoring MRIs within the first six months (plus more PRN)
BWH, MGH Departments of Neurology
Emergency Department Considerations
Acute stroke:
•
Thrombolysis (tPA, Tenecteplase)
strictly contraindicated
within 3 months of lecanemab therapy
•
No contraindications to thrombectomy
•
No contraindications to antiplatelet therapy
•
Please discuss initiation of anticoagulation in patients on lecanemab with ATP
Suspected
severe
ARIA:
•
MRI T2 FLAIR hyperintensity >10 cm associated with gyral swelling, sulcal effacement
•
Risk of intracerebral hemorrhage, seizure, coma
•
Treat with IV methylprednisolone 1 g daily for 5 days followed by oral taper
•
Consider ICU admission, continuous EEG monitoring
Protocol in Ellucid
BWH, MGH Departments of Neurology
Pitfalls … and opportunities
Pitfalls
•
Will demand outstrip our capacity?
•
Neurologists/PCP may be uncomfortable prescribing, also neuroradiologists for ARIA
•
Eligibility screening is resource intensive (CSF, cog assessments, genetic counseling)
•
Safety monitoring is resource intensive (e.g., multiple MRIs, urgent visit availability)
•
What happens to patients who have cognitive decline but are not eligible?
•
Increasing demand on our longitudinal services
•
Protocols to ensure safety in preventing ARIA/side effects
•
Treatment plans, 24-7 pager, open lines of communication
Opportunities
•
Can we break free from siloed care and coordinate better?
•
Subcutaneous formulations, combination therapy, prevention (AHEAD)?
•
Opportunities for research engagement; national registry
BWH, MGH Departments of Neurology
Gratitude and Optimism
•
The progresses in the clinical science of AD come from the collective efforts of many individuals
•
Researchers, clinicians
•
Public investment, private enterprise, philanthropy
•
Patients, research participants, and their families
•
This is a start, but there is much, much more work to do
BWH, MGH Departments of Neurology
Questions?
Pagers:
BWH: 31439
MGH: 25997
Email: mgbatp@mgb.org
BWH, MGH Departments of Neurology
The MGB Alzheimer Therapeutics Program is a collaborative effort leading to groundbreaking disease-modifying therapies for Alzheimer's disease. The development of Lecanemab (Leqembi), a monoclonal antibody targeting amyloid plaques, offers a new option to slow disease progression. The program's focus on clinical efficacy, dosing, and shared care models reflects years of dedicated work by multidisciplinary teams. Lecanemab aims to remove toxic amyloid oligomers and protofibrils, addressing the central role of amyloid in Alzheimer's pathophysiology. Eligibility criteria for treatment include mild cognitive impairment or mild dementia with specific cognitive testing and functional independence criteria. This advancement marks a significant achievement in Alzheimer's research and care delivery.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
The MGB Alzheimer Therapeutics Program Ushering in a new era of disease-modifying therapies for Alzheimer disease Fall 2023 BWH, MGH Departments of Neurology
Collective effort over years The plans presented reflect the tireless efforts of dozens of individuals over many years Aducanumab working group lecanemab working group ATP Weekly meetings for months; committees, logistical teams, multiple institutions, depts Clinicians, clinical scientists, pharmacists, radiologists, nursing, administrators, staff, IT The underlying scientific neurobiological models were pioneered here The clinical science has been advanced here Disease-modifying therapies, especially those targeting amyloid, has grown from a vision to a plan to now a reality This is a joyful moment there is now an option for slowing down the progression of Alzheimer disease This is a moment of intense focus; ensuring success requires careful systems to ensure a safe, efficacious, and equitable delivery 2 BWH, MGH Departments of Neurology
Outline Lecanemab (Leqembi) Dosing and administration Clinical efficacy Side effects: ARIA Alzheimer Therapeutics Program (ATP) Shared care model Requirements before referring How to refer in Epic Emergency Department considerations 4 BWH, MGH Departments of Neurology
Lecanemab Monoclonal antibody given as IV infusion every two weeks to remove amyloid plaques Targets Ab oligomers and protofibrils, which are highly toxic Amyloid hypothesis that amyloid toxicity is central to the pathophysiology of AD FDA approved for treating mild cognitive impairment or mild dementia due to Alzheimer disease Mild cognitive impairment (MCI): abnormal cognitive testing results, but full independence in instrumental (e.g., household tasks; finances) and basic (e.g., bathing, dressing) activities of daily living (ADLs) Mild dementia: abnormal cognitive testing results, some dependence in instrumental ADLs, but full independence in basic ADLs Patients with any loss of independence in basic ADLs due to cognitive impairment have moderate dementia and are not eligible for lecanemab due to Alzheimer disease: evidence of amyloid plaques in their brain by CSF biomarkers (lumbar puncture) or by amyloid PET scan 5 BWH, MGH Departments of Neurology
Lecanemab Phase 3 Trial: CLARITY AD Large, double-blind, placebo-controlled study Who: 1766 pts across 245 sites, ~900 received lecanemab Diagnosis: mild cognitive impairment or mild dementia Cognitive: MMSE >21, with memory loss Function: CDR global 0.5-1.0 Biological: positive amyloid-PET scan or CSF markers Excluded: people with bleeding in the brain, others Allowed anticoagulant use Followed for 18 months 6 BWH, MGH Departments of Neurology
Lecanemab: Phase 3 Study Results Placebo and lecanemab groups declined cognitively and functionally, but lecanemab group declined ~27% less over 18 months Activities of daily living (ADCS-MCI-ADL, secondary outcome): Clinical Dementia Rating Sum of Boxes (primary outcome): Van Dyck et al. (2023) New Engl J Med 388:9-21. 7 BWH, MGH Departments of Neurology
Lecanemab: Phase 3 Study Results Lecanemab removes amyloid effectively (PET) Lecanemab improved biomarker profiles in CSF and blood AD-specific: total and phosphorylated tau Degenerative markers - neurogranin 8 BWH, MGH Departments of Neurology
Lecanemab: Amyloid Related Imaging Abnormalities (ARIA) Focal areas of cerebral edema (ARAI-E) and associated microhemorrhages (ARIA-H) occurring in patients on lecanemab Occurred in 13% of all lecanemab-treated clinical trial patients Highest risk in first 3-6 months Mostly asymptomatic (>70% of ARIA) Case reports of fatal or debilitating injury (risk <1%) Risk factors for ARIA: Pre-treatment brain microhemorrhages (visible on MRI) Having the ApoE gene 4 allele (homozygotes > heterozygotes > non-carriers) Therapeutic anticoagulation ARIA requires MRI monitoring Kate et al, Alz Res and Therapy, 2018 9 BWH, MGH Departments of Neurology
Alzheimer Therapeutics Program (ATP) Overview Shared provider model akin to anticoagulation management service (similar to a Coumadin clinic ) Responsible for administration and safety monitoring of lecanemab Not responsible for other aspects of dementia care (other memory medications, psychiatric care, community services, etc.) --Referring provider remains main resource for patient and family; ATP always available for lecanemab-specific concerns --Typical cognitive and behavioral neurology referrals remain available for comprehensive cognitive evaluations The ATP has harmonized procedures across MGB, but BWH and MGH have separate referrals and physician pools (for now) Key Objectives ~400 currently treated MGB patients would meet criteria for lecanemab treatment, plus ~600 new patients with early AD evaluated annually. The process for determining drug eligibility includes a focused history and physical exam, standardized cognitive screening assessments, brain MRI, Alzheimer-specific biomarker testing (e.g., CSF testing or amyloid-PET), and APOE genetic testing. Screening and Eligibility Determination A critical function of the ATP clinic is drug safety monitoring with neuroimaging and clinical assessments. Patients will be triaged and offered urgent / emergent visits to address any possible side effects. Safety Monitoring and Triage The ATP will be a collaboration led by the Departments of Neurology at Massachusetts General Hospital (MGH) and Brigham and Women s Hospital (BWH), with appropriate partnerships with Geriatric Psychiatry, Pharmacy, Radiology, Nursing (Infusion), and the Mind & Memory Care Program at MGB institutions; and many allied clinicians across MGB. Coordinate the Work of Interdisciplinary Provider Teams To support quality improvement efforts and clinical research, clinical data will be collected, monitored and tracked for the ATP clinic. The ATP clinic will also contribute to a national registry to better understand the biological and clinical impact of anti-Alzheimer drugs. As future AD drugs come to market in the short term, this will be critical to the successful deployment of these drugs as well. Collect Clinical Data 11
Shared Service Model On/Off call model - 1 week on On-call provider takes care of much of the ATP activities: Sees patients in clinic (starting out with 4-hour session per week) Triages incoming referrals Orders pending eligibility studies (CSF, APOE, etc) Reviews MRIs for ARIA Reviews and addresses patient messages/calls/emails Makes decisions if/when to pause therapy plans based on MRI/symptoms 24-7 pager coverage for emergencies Passes off active issues to incoming on-call provider Supported by a growing administrative team 12
Requirements for ATP referral 1. Patient has mild cognitive impairment or mild dementia i.e., cognitive impairment does not affect basic activities of daily living (bathing, dressing, eating, toileting, etc.) 2. Brief cognitive screening test within the past 6 months Mini-mental State Exam (MMSE), Montreal Cognitive Assessment (MoCA), or St. Louis University Mental Assessment (SLUMS) Mini-cog not sufficient 3. Brain MRI within the past year 4. Blood tests within the past 6 months: CBC, CMP, PT-INR, PTT, TSH, Vitamin B12 5. For now, full-strength anticoagulation is a strict contraindication for lecanemab 6. A continued follow-up plan with the referring provider Alzheimer disease biomarkers (lumbar puncture or amyloid PET) and ApoE genotyping will be handled by the ATP, but can be done in advance if referring provider is comfortable When in doubt, please ask: mgbatp@mgb.org 13 BWH, MGH Departments of Neurology
ATP lecanemab eligibility checklist ATP clinicians will review available referral information to determine if the patient may meet eligibility criteria, and what workup remains within the ATP: Clinical diagnosis of AD-spectrum syndrome at severity of MCI or mild dementia MoCA 15 or greater, MMSE 22 or greater, SLUMS 16 or greater within 6 months of referral (exceptions may be considered) Does not have clinical diagnosis of Lewy body dementia or frontotemporal dementia-spectrum syndrome Is not on full-strength anticoagulation or immunosuppression Does not have other poorly controlled chronic medical, neurological, or psychiatric conditions Able to comply with infusion visits every 2 weeks CMP, B12, TSH, CBC, PT, PTT within 6 months of referral without abnormalities requiring further investigation MRI brain within 12 months of referral without exclusionary findings (>4 microbleeds, severe small vessel disease, large vessel infarcts) Elevated p-tau181/Abeta42 (Mayo Clinic labs), Abeta42/p-tau - 0.0105(t-tau) < 3.694 (Athena ADMark), or amyloid PET suggesting elevated brain amyloid APOE genotyping Challenging cases will be reviewed by the ATP s Plaque and Tangle Board (similar to an oncology tumor board) 14 BWH, MGH Departments of Neurology
How to refer in Epic 15 BWH, MGH Departments of Neurology
After referral ATP will screen chart and then contact patient May contact referring provider instead if more workup is required before referral or if there is a contraindication from chart review Up to three ATP visits before starting lecanemab: 1. Intake and eligibility Obtaining Alzheimer disease biomarkers (spinal fluid) 2. Discussion of biomarker results, counseling and ordering genetic testing (ApoE) 3. Review of ApoE; prescribing lecanemab Lecanemab infusions at MGB sites every two weeks Three additional safety monitoring MRIs within the first six months (plus more PRN) 16 BWH, MGH Departments of Neurology
Emergency Department Considerations Acute stroke: Thrombolysis (tPA, Tenecteplase) strictly contraindicated within 3 months of lecanemab therapy No contraindications to thrombectomy No contraindications to antiplatelet therapy Please discuss initiation of anticoagulation in patients on lecanemab with ATP Suspected severe ARIA: MRI T2 FLAIR hyperintensity >10 cm associated with gyral swelling, sulcal effacement Risk of intracerebral hemorrhage, seizure, coma Treat with IV methylprednisolone 1 g daily for 5 days followed by oral taper Consider ICU admission, continuous EEG monitoring Protocol in Ellucid 17 BWH, MGH Departments of Neurology
Pitfalls and opportunities Pitfalls Will demand outstrip our capacity? Neurologists/PCP may be uncomfortable prescribing, also neuroradiologists for ARIA Eligibility screening is resource intensive (CSF, cog assessments, genetic counseling) Safety monitoring is resource intensive (e.g., multiple MRIs, urgent visit availability) What happens to patients who have cognitive decline but are not eligible? Increasing demand on our longitudinal services Protocols to ensure safety in preventing ARIA/side effects Treatment plans, 24-7 pager, open lines of communication Opportunities Can we break free from siloed care and coordinate better? Subcutaneous formulations, combination therapy, prevention (AHEAD)? Opportunities for research engagement; national registry 18 BWH, MGH Departments of Neurology
Gratitude and Optimism The progresses in the clinical science of AD come from the collective efforts of many individuals Researchers, clinicians Public investment, private enterprise, philanthropy Patients, research participants, and their families This is a start, but there is much, much more work to do 19 BWH, MGH Departments of Neurology
Questions? Pagers: BWH: 31439 MGH: 25997 Email: mgbatp@mgb.org 20 BWH, MGH Departments of Neurology


")







 Overview")