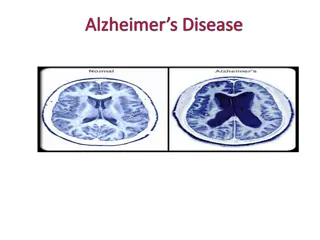
New FDA Guidance on Early Alzheimer's Disease - Janice Hitchcock, Ph.D.

Janice Hitchcock, Ph.D., discussed the new FDA guidance on early Alzheimer's disease in a webinar. The guidance highlights key sections such as introduction, background, and diagnostic criteria. It emphasizes the importance of early intervention, appropriate outcome measures, and diagnostic criteria based on consensus criteria. The presentation provides insights into trial designs, flexibility in population inclusion, and the clinical meaningfulness of cognitive endpoints in Alzheimer's drug development strategy.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
New FDA Guidance on Early Alzheimer s Disease Janice Hitchcock, Ph.D. Hitchcock Regulatory Consulting, Inc. Alzheimer s Association Business Consortium Ask the Expert Webinar 29 August 2018
Disclosures Former employee of Eli Lilly and Company Independent regulatory consultant on Alzheimer s disease and other neurodegenerative disorders Pharmaceutical industry Academia Advocacy groups Note: Advice is my opinion based on experience and is meant to start discussion; whether it applies or not will depend on individual development program 2
Outline Overview of each section Differences from 2013 guidance Interpretations and recommendations for Alzheimer s disease drug development strategy https://www.fda.gov/downloads/Drugs/GuidanceCompliance RegulatoryInformation/Guidances/UCM596728.pdf 3
Guidance Section I: Introduction Similar to 2013 guidance, scope limited to sporadic AD prior to dementia Autosomal dominant AD and AD dementia not included; some principles may apply Recommendation: Trial designs in excluded populations should still consider this guidance Unlike 2013 guidance, specifically recognizes overlap between later stages of early AD and early stage of dementia Allows flexibility for continued use of mixed population of mild cognitive impairment (MCI) + mild AD 4
Guidance Section II: Background Newly rewritten section; cognition as core symptom Discusses clinical meaningfulness in historical context of co-primary endpoints in dementia trials Cognition and global Cognition and function Acknowledges that cognition can be clinically meaningful, depending on magnitude and/or breadth of effect But small effects on sensitive measures may not have apparent clinical meaning Discusses need for Intervention at earliest stages of disease Appropriate outcome measures 5
Guidance Section III: Diagnostic Criteria for Early Alzheimer s Disease Newly rewritten section; retains importance of biomarkers to identify pathophysiological changes States that enrollment should be based on current consensus diagnostic criteria NIA-AA research diagnostic criteria, International Working Group criteria, NIA-AA research framework (A /tau/neurodegeneration [AT(N)] criteria) Proposes AD stages to categorize clinical trial subjects to determine outcome measures Consistent with numeric clinical staging proposed in NIA-AA research framework Albert et al (2011) Alzheimer s & Dementia 7:270 9; Sperling et al (2011) Alzheimer s & Dementia 7:280 92; Dubois et al (2010) Lancet Neurology 9:1118 27; Dubois et al (2014) Lancet Neurology 13:614 29; Jack et al (2018) Alzheimer s & Dementia 14:535-562 6
Diagnostic Criteria for Early Alzheimers Disease (cont.) FDA stage Description Presumed corresponding research diagnosis Patients with characteristic pathophysiologic changes of AD but no evidence of clinical impact Early preclinical AD Stage 1 Patients with characteristic pathophysiologic changes of AD and subtle detectable abnormalities on sensitive neuropsychological measures, but no functional impairment Late preclinical AD Stage 2 Patients with characteristic pathophysiologic changes of AD, subtle or more apparent detectable abnormalities on sensitive neuropsychological measures, and mild but detectable functional impairment Mild cognitive impairment (MCI) due to AD/prodromal AD Stage 3 Patients with overt dementia Stages 4, 5, and 6, corresponding with mild, moderate, and severe dementia Mild, moderate, severe AD dementia Stage 4, 5, 6 Quotes are from FDA guidance Early Alzheimer s Disease: Developing Drugs for Treatment (2018) https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM596728.pdf 7
Diagnostic Criteria (cont.) Need to consider stage at beginning and projected stage at end of trial Recommendation: Use consensus research diagnostic criteria to enroll subjects for trial, but also include reference to corresponding FDA-defined AD stage at enrollment projected for majority of subjects at end of trial Does not preclude use of more than one AD stage in trial population But FDA may expect use of endpoint for latest stage; impacts powering / probability of technical success Recommendation: Consider proportion of each stage and discuss proposed primary endpoint with FDA Mentions possibility of co-development of companion diagnostic Recommendation: Discuss with FDA early in development; time and resource implications if required 8
Guidance Section IV: Outcome Measures Newly rewritten section FDA stage Outcome measure and regulatory pathway Stage 3 (MCI/prodromal AD) Similar to 2013 guidance, accepts composite endpoint (cognitive and functional) or co-primaries Recommendation: Discuss with FDA if your trial proposes primary endpoint not consistent with guidance; provide scientific justification Cognitive-functional composite standard approval, or Co-primaries standard approval Stage 3 (~MCI / prodromal AD) Cognition only accelerated approval, or Cognition only standard approval possible, depending on effect magnitude and/or breadth Stage 2 (~late preclinical AD) Stage 2 (late preclinical AD) Different from 2013 guidance, opens possibility of standard (full) rather than accelerated approval pathway with cognitive endpoint Depends on magnitude and/or breadth of cognitive effect Biomarker effects also expected Notes that evolution of the scientific understanding of AD may also influence these considerations Recommendation: Include several cognitive and biomarker endpoints Biomarker only accelerated approval theoretically possible, but not yet Alternative: Longer duration and use Stage 2 measure (cognition) Stage 1 (~early preclinical AD) 9
Outcome Measures (cont.) Stage 1 (early preclinical AD): Suggests theoretical possibility ( in principle ) of accelerated approval pathway based on biomarker effect(s) FDA stage Outcome measure and regulatory pathway Cognitive-functional composite standard approval, or Co-primaries standard approval Stage 3 (~MCI / prodromal AD) But not yet supported by current state of science as reasonably likely to predict clinical benefit (regulatory standard) Suggests alternative sufficient duration for Stage 1 subjects transition to Stage 2; use Stage 2 outcomes Cognition only accelerated approval, or Cognition only standard approval possible, depending on effect magnitude and/or breadth Stage 2 (~late preclinical AD) Recommendation: Include biomarkers and cognitive endpoints; consider longer duration with interim analysis Similar to 2013 guidance, time-to-event analysis is possible endpoint for early AD Biomarker only accelerated approval theoretically possible, but not yet Alternative: Longer duration and use Stage 2 measure (cognition) Stage 1 (~early preclinical AD) No discussion of potential issues from empirical standpoint Recommendation: Consult with AD thought leaders on pros and cons 10
Guidance Section IV. E: Assessment of Disease Course Unlike 2013 guidance, does not mention disease modification ; instead permanently alter disease course or persistent effect on disease course Recommendation: Consider disease modification as concept for labeling; if allowed, likely to be different wording consider market research on alternatives Similar to 2013 guidance, discusses randomized (delayed) start design; most convincing approach to demonstrate persistent effect on disease course Recommendation: Include delayed start extension if disease modification claim is sought Different than 2013 guidance, states that biomarkers are not yet well enough understood to demonstrate persistent effect on disease course (disease modification) Recommendation: Include biomarkers as supportive evidence for drug effect (not disease modification claim) Similar to 2013 guidance, states that biomarker data can be analyzed without hierarchical structure; this could change depending on advances in AD research 11
Questions? 12
Potential questions What is the probability that FDA would allow a disease modification claim in labeling? What trial design features and outcome measures should be included to enable such a claim? How does FDA determine whether an outcome measure is clinically meaningful? Which diagnostic criteria should be used for inclusion of subjects in a clinical trial? Which biomarkers are most important to include in a clinical trial? What are the pros and cons of pursuing an accelerated approval pathway vs. a standard (full) approval pathway in AD? 13







")

")