Understanding Digoxin Pharmacology and Clinical Use

Digoxin, a cardiac glycoside, is utilized in managing congestive heart failure and atrial fibrillation due to its inotropic and chronotropic effects on the heart. It functions by inhibiting Na,K-ATPase, leading to increased intracellular calcium concentrations and augmented myocardial contractility. The therapeutic and toxic concentrations of digoxin are crucial considerations in its administration. Serum concentrations reflect the drug's action site, with notable differences between oral and intravenous dosing. Understanding the pharmacokinetics of digoxin is essential for safe and effective use in clinical practice.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Digoxin Dr. Kadhim Ali Kadhim B.Sc, Mcs.,Ph.D, in Clinical Pharmacy Lecturer in Dept. of Clinical Pharmacy/ College of Pharmacy/University of AL-Mustansiriyah. Kadhimali_2011@yahoo.com
Introduction Digoxin is the primary cardiac glycoside in clinical use. It is used for the treatment of congestive heart failure (CHF) because of its inotropic effects on the myocardium and for the treatment of atrial fibrillation because of its chronotropic effects on the electrophysiological system of the heart. The positive inotropic effect of digoxin is caused by binding to sodium- and potassium activated adenosine triphosphatase, also known as Na,K-ATPase or the sodium pump.
Introduction Digoxin-induced inhibition of Na,K-ATPase leads to decreased transport of sodium out of myocardial cells and increased intracellular sodium concentrations that aid calcium entry and decrease calcium elimination via the sodium-calcium exchanger. The increased intracellular calcium is stored in the endoplasmic reticulum so that action potential induced calcium release is augmented causing enhanced myocardial contractility.
THERAPEUTIC AND TOXIC CONCENTRATIONS When given as oral or intravenous doses, the serum digoxin concentration time curve follows a two- compartment model and exhibits a long and large distribution phase of 8 12 hours. During the distribution phase, digoxin in the serum is not in equilibrium with digoxin in the tissues, so digoxin serum concentrations should not be measured until the distribution phase is finished. When drug distribution is complete, digoxin serum and tissue concentrations will be proportional to each other so that digoxin serum concentrations reflect concentrations at the site of action.
FIGURE 6-1 Digoxin serum concentrations after 250-g doses given intravenously (circles and solid line) and orally as a tablet (squares with dashed line). After an intravenous dose, digoxin serum concentrations are very high because all of the drug is initially contained in the blood. During the distribution phase, digoxin begins to move out of the vascular system into the tissues. It is also cleared from the body during this phase. Digoxin serum concentrations decline relatively rapidly over an 8- to 12-hour time period until the blood and tissues are in psuedo-equilibrium with each other. During the elminination phase, digoxin serum concentrations in patients with good renal function (creatinine clearance >80 mL/min) decline with a half-life of about 36 hours. After oral tablet administration, about 70% of a digoxin dose is absorbed from the gastrointestinal tract. Maximum, or peak, concentrations occur about 1.5 2 hours after oral dosing with tablets, and the distribution phase still lasts 8 12 hours. During the elimination phase, intravenous and oral digoxin have the same terminal half-life.
There is a great deal of inter- and intrapatient variability in the pharmacodynamic responses to digoxin. Clinically beneficial inotropic effects of digoxin are generally achieved at steady-state serum concentrations of 0.5 1 ng/mL. Increasing steady-state serum concentrations to 1.2 1.5 ng/mL may provide some minor, additional inotropic effect. Chronotropic effects usually require higher digoxin steady- state serum concentrations of 0.8 1.5 ng/mL. Additional chronotropic effects may be observed at digoxin steady-state serum concentrations as high as 2 ng/mL. Because of pharmacodynamic variability, clinicians should consider these ranges as initial guidelines and rely heavily on patient response to monitor digoxin therapy.
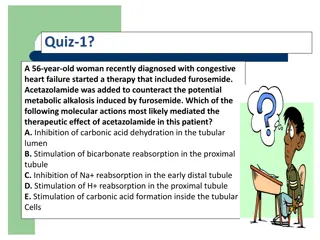
At digoxin concentrations of 2.5 ng/mL or above ~50% of all patients will exhibit some form of digoxin toxicity. Most digoxin side effects involve the gastointestinal tract, central nervous system, or cardiovascular system. Steady-state digoxin serum concentrations above 2 ng/mL are associated with an increased incidence of adverse drug reactions. In the case of life-threatening digoxin overdose, digoxin antigen binding fragments or digoxin immune Fab (Digibind) are portions of digoxin-specific antibodies that can be used to rapidly reverse the adverse symptoms
Clinical Monitoring Parameters In patients receving digoxin for heart failure, the common signs and symptoms of CHF should be routinuely monitored; Left-sided failure dyspnea on exertion, paroxysmal nocturnal dyspnea, orthopnea, tachypnea, cough, hemoptysis, pulmonary rales/edema,S3 gallop, pleural effusion, Cheyne- Stokes respiration. Right-sided failure abdominal pain, anorexia, nausea, bloating, constipation, ascites, peripheral edema, jugular venous. distention, hepatojugular reflux, hepatomegaly; general symptoms fatigue, weakness, nocturia, CNS symptoms, tachycardia, pallor, digital cyanosis, cardiomegaly
When used for the treatment of atrial fibrillation, digoxin will not stop the atrial arrhythmia but is used to decrease, or control, the ventricular rate to an acceptable value (usually <100 beats/min). The patient s pulse or ventricular rate should be monitored, and an electrocardiogram can also be useful to clinicians able to interpret the output. Atrial fibrillation is characterized by 400 600 nonuniform atrial beats/min.
Patients with severe heart disease such as cornary artery disease (angina, myocardial infarction) can have increased pharmacodynamic sensitivity to cardiac glycosides, and patients receiving these drugs should be monitored closely for adverse drug effects. Also, augmented pharmacologic responses to digitalis derivatives occur with serum electrolyte disturbances such as hypokalemia, hypomagnesemia, and hypercalcemia even though steady-state digoxin serum concentrations are in the therapeutic range. Serum potassium concentrations should be routinely monitored in patients receiving digoxin and potassium-wasting diuretics. Potassium supplimentation may be necessary in some of these patients. Also, many patients receiving digoxin and diuretics will be receiving angiotensin I converting enzyme (ACE) inhibitors which can cause potassium retention.
As an adjunct to the patients clinical response, postdistribution (812 hours postdose) steady-state digoxin serum concentrations can be measured 3 5 half-lives after a stable dose is initiated. Digoxin is primarily eliminated unchanged by the kidney (~75%) so its clearance is predominately influenced by renal function. Once stable, therapeutic steady-state digoxin serum concentrations and dosage levels have been established, serum creatinine measurements can be used to detect changes in renal function which may result in digoxin clearance and concentration alterations. Hospitalized patients with severe or acute heart failure may need to have serum creatinine determinations 2 3 times weekly to monitor renal function, while ambulatory patients with stable heart failure may only need yearly serum creatinine measurements.
BASIC CLINICAL PHARMACOKINETIC PARAMETERS The primary route of digoxin elimination from the body is by the kidney via glomerular filtration and active tubular secretion of unchanged drug (~75%). The remainder of a digoxin dose (~25%) is removed by hepatic metabolism or biliary excretion. The primary transporter involved in active tubular secretion and biliary excretion is p-glycoprotein (PGP). Enterohepatic recirculaton (reabsorption of drug from the gastrointestinal tract after elimination in the bile) of digoxin occurs. Digoxin is given as an intravenous injection or orally as a tablet, capsule, or elixir. When given intravenously, doses should be infused over at least 5 10 minutes. Average bioavailability constants (F) for the tablet, capsule, and elixir are 0.7, 0.9, and 0.8.
BASIC CLINICAL PHARMACOKINETIC PARAMETERS Digoxin is not usually administered intramuscularly due to erratic absorption and severe pain at the injection site. Plasma Protein binding is ~25% for digoxin. Usual digoxin doses for adults are 250 g/d (range: 125 500 g/d) In patients with good renal function (creatinine clearance 80 mL/min) While, 125 g every 2 3 days in patients with renal dysfunction (creatinine clearnace 15 mL/min).
Effects of Disease States and Conditions on Digoxin Pharmacokinetics and Dosing Disease States and Conditions That Alter Digoxin Pharmacokinetics that shown as in Table (6-2) . Adults with normal renal function (creatinine clearance 80 mL/min, have an average digoxin half-life of 36 hours (range: 24 48 hours) and volume of distribution of 7 L/kg (range: 5 9 L/kg). The volume of distribution is large due to the extensive tissue binding of digoxin in the body. Digoxin pharmacokinetics are not effected by obesity (>30% over ideal body weight), so volume of distribution and dosage estimates should be based on ideal body weight.
Effects of Disease States and Conditions on Digoxin Pharmacokinetics and Dosing Because digoxin is principally eliminated by the kidney, renal dysfunction is the most important disease state that effects digoxin pharmacokinetics.The digoxin clearance rate decreases in proportion to creatinine clearance. The equation that estimates digoxin clearance from creatinine clearance is: Cl = 1.303 (CrCl) + ClNR, where Cl is digoxin clearance in mL/min, CrCl is creatinine clearance in mL/min, and ClNR is digoxin clearance by non-renal routes of elimination which equals 40 mL/min in patients with no or mild heart failure. Digoxin volume of distribution, in addition to clearance, decreases with declining renal function.
FIGURE 6-2 :Digoxin clearance is proportional to creatinine clearance for patients with [circles with solid line: Cl = 1.303(CrCl) + 20] and without [squares with dashed line: Cl = 1.303(CrCl) + 40] moderate-severe (NYHA class III or IV) heart failure. Non-renal clearance (denoted by the y-intercept) is lower for patients with moderate-severe heart failure because reduced cardiac output results in decreased liver blood flow and digoxin hepatic clearance.
The equation that estimates digoxin volume of distribution using creatinine clearance is: Where V is digoxin volume of distribution in L/70 kg, Wt is body weight in kilogram (use ideal body weight if >30% overweight) and CrCl is creatinine clearance in mL/min. Because digoxin volume of distribution and clearance decrease simultaneously in patients with renal failure, the average half-life for digoxin of 5 days is shorter than what might be expected if clearance alone decreased [t1/2 = (0.693 V) / Cl].
Digoxin is not significantly eliminated by hemodialysis or peritoneal dialysis.Hemofiltration does remove digoxin with a typical sieving coefficient of 0.7. In many cases, a sufficient amount of digoxin will not be removed to warrant an increased maintenance dose. However, due to pharmacokinetic variability, some patients may need a periodic booster dose to increase digoxin concentrations Heart failure decreases cardiac output which in turn decreases liver blood flow. Liver blood flow is an important factor in the determination of hepatic clearance for drugs because it is the vehicle that delivers drug molecules to the liver for possible elimination.Moderate-severe heart failure decreases the hepatic clearance of digoxin by this echanism. When estimating digoxin clearance for the purpose of computing initial drug doses, it is necessary to decrease the nonrenal clearance (ClNR) factor to 20 mL/min in the equation to compansate for decreased hepatic clearance: Cl = 1.303 (CrCl) + 20, where Cl is digoxin clearance in mL/min, CrCl is creatinine clearance in mL/min, and 20 is digoxin nonrenal clearance ClNR in mL/min.
Thyroid homone regulates basal metabolic rate, and thyroid status will influence every major organ system in the body including the heart (heart rate and cardiac output), liver (liver blood flow and microsomal drug-metabolizing enzyme function), and kidney (renal blood flow and glomerular filtration rate). Patients who are hypothyroid will have slower metabolic rates and eliminate digoxin more slowly than euthryoid patients (t1/2 = 48 hours with normal renal function). Hyperthyroid patients have faster metabolic rates and elminate digoxin faster than euthyroid patients (t1/2 = 24 hours with normal renal function). Hyperthyroid patients can present with atrial fibrillation which may be treated with digoxin. Generally, these patients require higher digoxin doses to control ventricular rate because of the increase in digoxin clearance.
Similar to other drugs, digoxin clearance is lower in neonates and premature infants because renal and hepatic function are not completely developed. Premature infants and neonates have average digoxin half-lives equal to 60 hours and 45 hours, respectively. In older babies and young children (6 months to 8 years old) renal and hepatic function are fully developed and half-lives can be as short as 18 hours. Older children ( 12 years old) have mean digoxin half-lives (t1/2 = 36 hours) that are similar to those found in adults. Also, volume of distribution is larger in infants and children compared to adults as is found with many other drugs. Malabsorption of oral digoxin has been reported in patients with severe diarrhea, radiation treatments to the abdomen and gastrointestinal hypermotility. In these cases, steady-state digoxin serum concentrations decrease due to poor bioavailability of the drug.
DRUG INTERACTIONS Digoxin has an extensive list of drug interactions with other agents. Because of this, only the most common and severe drug interactions will be discussed. Inhibition of P-glycoprotein, a drug efflux pump which is found in the kidney, liver, and intestine, appears to be involved in the majority of digoxin interactions.
Initial Dosage Determination 1. 2. Volume of distribution estimate 3. Selection of appropriate pharmacokinetic and equations 4. Steady-state concentration selection 5. Dosage computation Pharmacokinetic Dosing Method Clearance estimate