Portal Vein Imaging Techniques and Anomalies Overview
Portal vein imaging is crucial for evaluating conditions affecting the abdominal part of the gastrointestinal tract. Techniques such as spleno-portography and CT triphasic contrast imaging are used to visualize the portal vein and diagnose anomalies like portal-systemic collaterals and porto-systemic shunts. Various shunt types, including porto-systemic, porto-arterial, and arterio-systemic, can be identified through imaging modalities like CECT and Doppler. Understanding anomalies like persistent ducts, venous paths, and portal vein abnormalities is essential for diagnosing and managing hepatic conditions related to portal hypertension. Evaluation of portal vein abnormalities can help in detecting complications like thrombosis, rupture, and portal hypertension.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
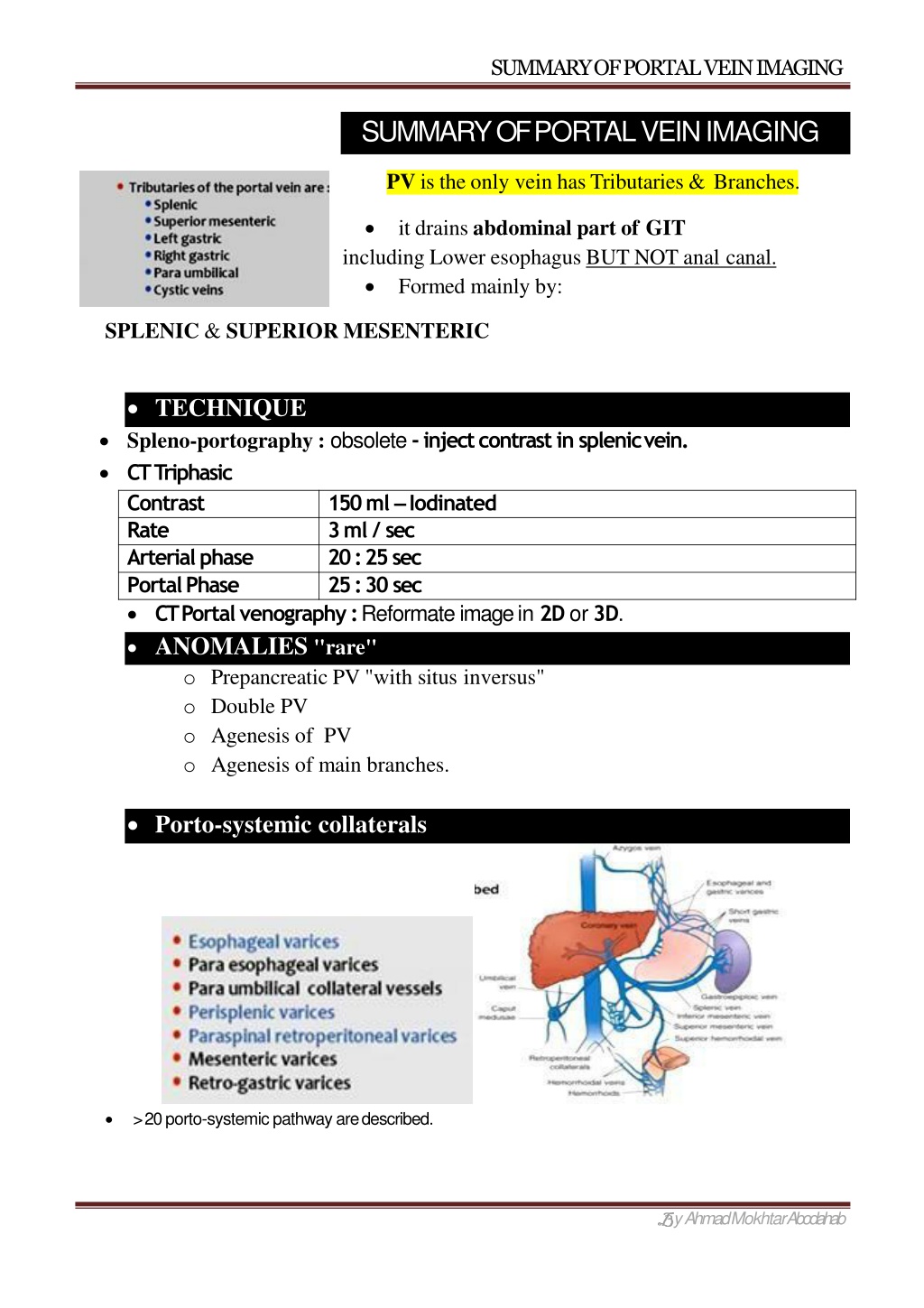
SUMMARY OF PORTAL VEINIMAGING SUMMARY OF PORTAL VEINIMAGING PV is the only vein has Tributaries & Branches. it drains abdominal part of GIT including Lower esophagus BUT NOT anal canal. Formed mainly by: SPLENIC & SUPERIOR MESENTERIC TECHNIQUE Spleno-portography : obsolete -inject contrast in splenicvein. CTTriphasic Contrast 150 ml Iodinated Rate 3 ml / sec Arterialphase 20 : 25sec PortalPhase 25 : 30sec CT Portal venography : Reformate image in 2D or3D. ANOMALIES "rare" o Prepancreatic PV "with situs inversus" o Double PV o Agenesis of PV o Agenesis of main branches. Porto-systemic collaterals > 20 porto-systemic pathway aredescribed. y Ahmad MokhtarAbodahab
SUMMARY OF PORTAL VEINIMAGING Caput Medusa "Paraumblical" Esophageal &Paraesophageal varices Rectal PORTALCAVERNOMA o PV stenosis or occlusions Multiple dilated venous channels at porta hepatis. o "worm Like" mass of veins. SHUNTS PV/HV PV/HA Hv/HA Porto-systemic Arterio-Portal A-V shunt commonest Can occur Rare in Liver I Porto-Systemicshunts: Etiology: Congenital / Cirrhosis / Traumatic / P. Hypertension Sites : C.P.: Rt P.V. branch / IVC Commonest Hepatic encephalopathy Imaging: CECT Show communication Color Doppler "Best tool to diagnose " y Ahmad MokhtarAbodahab
SUMMARY OF PORTAL VEINIMAGING PERSISTENT DUCTS VENOUSSES -Lt PV /IVC TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT TIPSS ttt of portal Hypertension. Indications: Varices Budd chiari - Refractory ascitis Hypersplinism (connecting Hepatic vein / Portal vein) II Porto-Arterial shunts: Etiology: - Congenital : rare o Traumatic : stab, bullet o Iatrogenic : common / as PTC, biopsy o Malignant : main cause CT : Enhanced PV at arterial phase Porto-Arterial shunt contrasttransmit to PV at arterial phase enhancing of Nonmalignantarea,but MimicHCC To Differentiate: - - - US Doppler MRI SPIO"SuperParamagneticIron Oxide " : * Deposited inHCC * Washed out inshunt No Focal lesion arterial flow inPV y Ahmad MokhtarAbodahab
SUMMARY OF PORTAL VEINIMAGING III Arterio-Systemic shunts: raretype Etiology: -Congenital AVM "Rendu osler disese" -HCC -Large Hemangioma CT Arterial phase Early enhanced Hepatic vein. Communication of Hepatic Artery & Vein Extra hepatic Porto Caval shunt "Abernathy malformation" 2 Types Congenital Porto-Systemic shunt outside the liver Type 1 More in Females Congenital absent PV Splenic & SMV join IVC separately Complete shunt portal blood to IVC + - Polysplenia - Biliary atresia Type 2 Males Splenic & SMV join each other forming short abnormal PV connected to IVC PV + - Focal nodular Hyperplasia - HCC Associated PORTALVENOUSABEURYSM "Rare" 3% of all venousAneurysms Etiology: -Portal hypertension Site : o mostly at junction of splenic & SMV "i.e. 1st part of PV" o Main PV o Bifurcation or main branches C.P. : - Mostly asymptomatic Complications: - Thrombosis - Rupture - Portal hypertension - Embolism - Compression: on CBD or dudenoum "Commenst sites: Jagular, Popleteal ,Saphenous, " -Pancreatitis -Surgery -Trauma -Abdominal Pain y Ahmad MokhtarAbodahab
SUMMARY OF PORTAL VEINIMAGING Portal & Splenic vein Thrombosis Etiology : Causes of hypercoagulopathy -PV Rim enhanced around filling defect +/- - - - Portal Cavernoma Collaterals "varices" Shunt "arterio-portal" *Malignant Thrombus : Enhanced / dilating PV Metabolic Active "Best diagnosed by US" NB. PV thrombosis phase alternative arterial supply of Hepatic parenchyma Heterogenous areas of enhancement @ arterial = THAD : Transient Hepatic AttenuationDifference y Ahmad MokhtarAbodahab
SUMMARY OF PORTAL VEINIMAGING GAS in Portal System "uncommon sign " BAD SIGN = Surgical emergency / High Mortality rate Etiology : commonest 2 causes - Adult: Mesenteric ischemia - Infants: Necrotizing enterocolitis D. D. : *Biliary gas Central not reaching peripheral 2cm *Portal Gas central & periphery up to subcapsular Passive Hepatic Congestion or Congestive Hepatopathy Etiology: - Budd Chiari Pathology: Congestion impairment of drainage Hepatomegally & dilated hepatic veins Hypoxia / increase enzymes Finally "Cirrhosis" Imaging : - Early enhancement of dilated Hepatic veins & IVC "at arterial phase" "Stasis of blood with in hepatic parenchyma" - Rt Heart Failure - Constrictive Pericarditis -Hepatomegally - Ascitis - Cardiomegally -Pleural / Pericardial effusions DilatedIVC Mottled Liver "Nutmeg" Nutmeg= y Ahmad MokhtarAbodahab
SUMMARY OF PORTAL VEINIMAGING Budd-Chiari Syndrome Congested liver Hepatic Veins or IVC obstruction. "Acute or Chronic" - - - Motteled "Nutmeg"Liver Obstructed HV & or IVC Decreased enhancement ofperophery MRI notice IVCobstruction Jun 2018 AhmadMokhtarAbodahab Ass. Lecturer of radiology SohagUniversity Imaging of Portal Venous system - Prof Dr. Mamdouh Mahfouz (Cairo2018) https://www.youtube.com/watch?v=dwIU4USk6zM y Ahmad MokhtarAbodahab