Verbal De-Escalation Techniques for Connecting with Kids at School Health Conference
This content highlights the importance of verbal de-escalation in connecting with kids through a school health conference, providing insights on crisis development models, handling anxiety, empathic listening, and dealing with defensive behavior. The workshop emphasizes building rapport and understanding different crisis behavior levels to effectively support individuals in distress.
- Verbal De-Escalation
- School Health Conference
- Crisis Development Models
- Empathic Listening
- Defensive Behavior

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Verbal De-Escalation Workshop Connecting with Kids Through School Health Conference Connecting with Kids Through School Health Conference Eaton RESA Instructional Services Micki Fuhrman, Regional School Health Coordinator, Certified Crisis Prevention Institute Trainer, Prevention Consultant
Introductions Who s in the room? Do you ever deal with a person who is upset?
Crisis Development Model Crisis Development Behavior Levels Staff Attitudes and Behaviors Understanding these levels of crisis development and the corresponding attitudes and behaviors for staff response can help to de- escalate a potential crisis.
Anxiety Definition: a feeling of worry, nervousness, or unease, typically about an imminent event or something with an uncertain outcome. Response: Supportive. An empathetic, nonjudgmental approach attempting to alleviate anxiety.
Empathic Listening Definition - An active process to discern what someone is really trying to communicate. Be non-judgmental Give your undivided attention Listen to what the person is REALLY saying Focus on feelings as well as facts Allow for silence
Brene Brown Empathy What do you take away from this video? Is there a concept or phrase that will stay with you?
Defensive Definition Individual may challenge authority and become belligerent This is the beginning stage of the loss of rationality
Closer Look at Defensive Behavior Questioning: Rational Answer question Challenging Redirect, or repeat
Defensive behavior Refusal--Restate Release--Allow venting Intimidation--Begin documentation Tension Reduction Therapeutic Rapport
Acting Out Person Acting Out Person The total loss of control and rationality which often results in physical acting out behavior.
Physically Acting Out Person What could this look like? Distinguish between frustration and physically acting out What is your safety plan and protocol?
Safety Plan Where do you meet? Who is near you? What can be done to support you? Is there a panic signal?
Tension Reduction Decrease in physical and emotional energy Regain rationality Drop in energy Examples?
Re-establish Connection (Therapeutic Rapport) An attempt to re-establish communication with an individual who is in the tension reduction stage Examples
Personal Space How do you define personal space? Average personal space is_______. Considered an extension of self. (What?) Influencing factors: How do you respond when someone is in your personal space?
Nonverbal (or Kinesic) Behavior **even when people can t see you** Definition - Non-verbal messages communicated by body postures, gestures or motions. Your kinesic behavior can serve to escalate or de- escalate a given situation
Nonverbal Behavior Body Posture and Motion Communicating with body language: facial expressions gestures posture movement
Supportive Stance Communicates Respect Is non-threatening Contributes to staff member s personal safety
Paraverbal Communication **How you say what you say** Tone: Avoid inflections of: Impatience Condescension (insincerity) Inattention Loudness: Appropriate for the distance and situation; enough to be heard Cadence: Talk in an even rate and rhythm
Paraverbal Communication I didn t say you were stupid
CPI Verbal Escalation Key Points to Remember! Don t take the verbal acting out personally Avoid getting into power struggles Be consistent SET LIMITS
Keys To Setting Limits Simple (limit choices, no technical jargon, acronyms) Reasonable (consequence fits offence) Enforceable(you re able to follow through)
Verbal Intervention Tips and Techniques Do - Remain calm Isolate the situation Enforce limits Listen Be aware of nonverbal signs Be consistent Watch personal space
Verbal Intervention Tips and Techniques Don ts Engage in power struggles Make false promises Fake attention Be threatening Use sarcasm Overreact
No time to wait for a response? Pay now or Pay later
Tools in your tool belt Be supportive Empathic listening Answer questions (information seeking) Re-direct (if challenged) Set limits (positive choice) Allow venting Call for help
Precipitating Factors Internal or external causes of an acting out behavior over which we have little or no control. Understanding precipitating factors can help: prevent acting out behavior, depersonalize the crisis & avoid becoming a precipitating factor.
What is trauma? Trauma is defined by the American Psychological Association (APA) as the emotional response someone has to an extremely negative event. While trauma is a normal reaction to a horrible event, the effects can be so severe that they interfere with an individual s ability to live a normal life.
ACEs (adverse childhood experiences) have a powerful correlation to adult health outcomes later in life. As the number of traumatic experiences increases, so does the risk of an array of social and health problems experienced in adulthood, such as: social, emotional and cognitive impairment; adoption of health-risk behaviors; Disease Disability Social problems; and early death
ACEs-Adverse Childhood Experiences Physical, sexual and verbal abuse. Physical and emotional neglect. A family member: depressed or diagnosed with other mental illness; Addiction in prison. Witnessing a mother being abused. Losing a parent to separation, divorce or other reason.
Adverse Childhood Experiences Include: Physical/Emotional/Sexual neglect or abuse Alcohol/Drug use/abuse in the home Incarcerated household member Household member who is chronically depressed, mentally ill, institutionalized, or suicidal Domestic violence Absent Parent
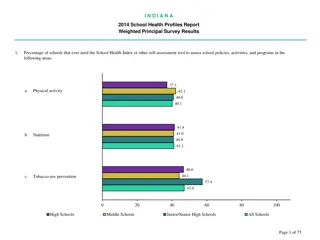
ACEs Data 46% of all children in the United States have at least one ACE. 35% of children in Michigan have 1- 2 ACE s. 14% of children in Michigan have 3 or more. The most common ACE in the country is economic hardship.
ACEs Data (continued) Most common ACE s in Michigan(in order) Divorce/Separation Economic Hardship Alcoholism Mental illness
Behavioral and Developmental Effects of Trauma: Biologically based challenges: Problems with movement and sensation Hypersensitivity to physical contact Insensitivity to pain. Problems with coordination and balance Unexplained physical symptoms Increased medical problems (asthma, skins problems, autoimmune disorders Body reactions such as racing hearts, churning stomach or sweatiness.
Behavioral and Developmental Effects of Trauma- Children may have difficulties with mood regulations as demonstrated by difficulty: Knowing/identifying their feelings Describing feelings and internal states Describing their wishing and desires to others Utilizing coping skills.
Behavioral and Developmental Effects of Trauma Attachment difficulties characterized by: Difficulties with boundaries. Feeling distrustful and suspicions of others. Becoming socially isolated and having difficulty relating to and empathizing with others.
Behavioral and Developmental Effects of Trauma Cognition and Self- Concept challenges Difficulties focusing and completing tasks. Problems planning and anticipating the future. Understanding their own role in their own life. Disturbed/distorted body image. Low self esteem Shame, guilt Dissociation
Behavioral and Developmental Effects of Trauma Children may demonstrate: Poor impulse control Self-destructive behaviors Verbal and physical aggression towards others. Excessive amounts of energy. Incongruent emotions (crying, laughing, etc.) Yelling Name calling Provocative behaviors
Rational Detachment Staff s ability to maintain professionalism and not take acting out behavior personally - To stay in control of one s behavior and not take it personally Maintain a professional attitude Find positive outlets to relieve negative energy
Integrated Experience The concept that staff s attitude, action and behavior directly influences a client s response, attitude and behavior. Can I control someone s behavior?
Debriefing Why is it important? How do you do it? Who do you do it with? Is there an office protocol?
COPING Control Rationality returned Orient To the basic facts Patterns Of behavior Investigate - Alternatives Negotiate Agree to changes Give Support, encouragement, THE RETURN TO COMMUNITY
Ive come to a frightening conclusion that I am the decisive element in the classroom. It s my personal approach that creates the climate. It s my daily mood that makes the weather. As a teacher, I possess a tremendous power to make a child s life miserable or joyous. I can be a tool of torture or an instrument of inspiration. I can humiliate or humor, hurt or heal. In all situations, it is my response that decides whether a crisis will be escalated or de-escalated and a child humanized or dehumanized. - Haim Ginott
THE END THE END THANK YOU FOR PARTICIPATING


















 Behavior")












 have a powerful")



")