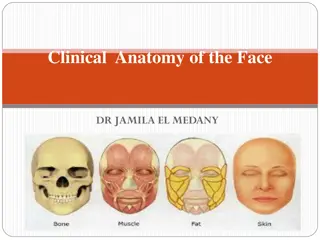
Overview of Joint Anatomy and Injections by Dr. Olude

Dr. Olude presents a comprehensive guide on applied anatomy, arthrology, and intra-articular injections. The content covers types of joints, classifications of synarthroses, diarthroses, and amphiarthroses, as well as thoracic limb articulations and important bones and joints of the forelimb. Detailed descriptions and images enhance understanding of joint structures and functions.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
VBA 501: APPLIED ANATOMY ARTHROLOGY AND INTRA ARTICULAR INJECTIONS. DR OLUDE, M.A.
TYPES OF JOINTS Synarthroses Diarthroses Amphiarthroses
SYNARTHROSES Joints united by a fibrous tissue, cartilage or a mixture of both. Often termed immovable joints. E.g. Suture: margins interlock 1. squamos overlyinig edges (temporal mandibular) 2. serrata: frontal 3. harmonious: nasal Syndesmosis: uniting medium is elastic tissue, fibrous or both Synchondrosis/synostosis: uniting medium is cartilage/bone Symphisis: joints in the median plane Gomphosis: tooth in alveoli
DIARTHROSES Joint with a: cavity, capsule with synovial fluid Mobility CLASSIFICATION Ginglymus: hinge joint (elbow) Arthrodia: gliding (intercarpals) Trochlear: pivot (atlantoaxial) Enarthrosis: ball and socket (hip)
Diagramatic representation of the Synovial joint A typical diarthroses
AMPHIARTHROSES Joints have both synarthrodial and diarthrodial features: Intercentral vertebral joints (between bodies) Interneural vertebral joints (between articular processes).
Thoracic limb articulations Shoulder Elbow Carpal Fetlock Pastern Coffin
Important bones and joints of the forelimb Scapula (shoulder blade): flat bone with a large area of cartilage that partially forms the withers. The shoulder length and angle is very important to horsemen when evaluating conformation. Humerus: lies between the scapula and the radius, making an angle of about 55 degrees down and back. Radius: extends from the elbow, where it articulates with the humerus, and travels downward to the carpus. It forms the "forearm" of the horse along with the ulna. Ulna: caudal to the radius, it is usually partially fused to that bone in an adult horse.
Shoulder joint (scapulohumeral joint): usually has an angle of 120-130 degrees when the horse is standing, which can extended to 145 degrees, and flexed to 80 degrees (such as when the horse is jumping and obstacle). Elbow joint (humeroradial joint): hinge joint that can flex 55-60 degrees. Carpus (knee): consists of 7-8 bones placed in 2 rows to form 3 joints. The 1st carpal bone is present only 50% of the time.
Pelvic limb articulations Sacro Iliac Hip Stifle -femoro-patellar -femoro-tibial Hock -tibio-tarsal -intertarsal -tarso-metatarsal
Important bones and joints of the hindlimb Pelvis: made up of the os coxae, the largest of the flat bones in a horse. It is made up of the ilium, the ischium, and the pubis. At the junction of these three bones is a cavity called the acetabulum, which acts as the socket of the hip joint. The pelvic cavity is larger in diameter in the mare than in the stallion, providing more room for the foal during birth. Femur: the largest long bone in a horse. Proximally it forms a ball-and-socket joint with the pelvis to form the hip joint, and distally it meets the tibia and patella at the stifle joint. It serves as an attachment point for the deep and middle glueteal muscles, and the accessory and round ligaments. Patella
Tibia: runs from stifle to hock. The proximal end provides attachment for the patellar ligaments, meniscal ligaments, cruciate ligamnents, and collateral lligaments of the stifle. The distal end provides attachment for the collateral ligaments of the hock. Fibula: completely fused to the tibia in most horses. Hip joint : Ball-and-socket joint made up of the acetabulum of the pelvis and the femur. It is very stable. Stifle joint (femoropatellar joint): actually composed of three joint compartments: the femoropatellar joint, the medial femorotibial joint, and the lateral femorotibial joint, which are stabilized by a network of ligaments. The stifle has an articular angle of about 150 degrees. Tarsus (hock): consists of 6 bones (of which one is made up of the fused 1st and 2nd tarsal bones) aligned in 3 rows. The largest bone in the hock, the calcaneus or fibular tarsal bone, corresponds to the human heel, and creates the tuber calcis (point of hock). It is to this point that the tendon of the gastrocnemius, portions of the biceps femoris, and portions of the superficial digital flexor attach.
INDICATIONS Intra-articular injections are performed to sterilely deliver one or more pharmaceutical drugs or other products directly into the joint. The two most common reasons for a Veterinarian to perform a joint injection are to anesthetize or block a joint during a lameness examination or to medicate a joint to help keep the horse s joints pain-free. INDICATIONS Joint injury, joint disease secondary to trauma or injury and osteoarthritis (OA) are major causes of attrition and loss of function in horses.
TECHNIQUE Regardless of the product being administered, the process of delivering intra-articular medications is essentially the same. The joint is cleaned with an antiseptic soap for approximately 10-20 minutes. The soap is rinsed off with isopropyl alcohol. Clipping the horse s hair is often not necessary. The Veterinarian then injects the desired drugs or products into the clean joint using sterile needles and syringes while wearing sterile gloves. Well behaved horses might only require a twitch to ensure sufficient restraint, but less-well mannered horses will require sedation.
Stifle The stifle joint consists of three compartments: femoropatellar, medial femorotibial and lateral femorotibial. Communication between the medial femorotibial and femoropatellar joints commonly exists and the lateral femorotibial joint usually does not communicate. However, variability in communication between these joints does occur thus, they can be treated (the three compartments of the joint) as separate entities to ensure completeness of diagnostic anesthesia or therapeutic injections. The stifle joint can be blocked differently depending on the case being evaluated and time available for the evaluation. Many times all three joints of the stifle will be anesthetized simultaneously to determine if the lameness does or does not originate from the stifle. An alternative approach that can be applied is to sequentially block individual pouches of the joint. If done in this manner the particular compartment within the stifle with pathology can be identified.
Identifying the compartment involved can be particularly useful in determining therapeutic approaches and may affect other procedures, such as arthroscopic evaluation. routinely anesthetize the medial femorotibial joint first. The most common site of injection is between the medial patellar and medial collateral ligaments, just proximal to the tibia. With deep palpation of the area one can usually recognize the edge of the medial meniscus. Recommendations vary in the length of needles used. 19 gauge 1 inch needle is o.k for this joint. If effusion is present synovial fluid is readily obtained. Effusion is not always apparent in lame horses but a small amount of fluid can usually be retrieved.
The traditional method of injecting this joint is to approach the joint from the dorsal aspect just medial or lateral to the middle patellar ligament. An 18 gauge 3 in. needle is directed in a plantar direction under the patella. OR approach the lateral cul-de-sac of the joint. An 18 gauge 1 -inch needle is inserted plantar to the lateral patellar ligament, approximately 5 cm proximal to the lateral tibial condyle. This procedure can be easier to accomplish and synovial fluid is obtained more often.
Sacro iliac/ Coxofemoral The coxofemoral joint can be the most intimidating joint to inject. However, the joint can be entered in most horses and the more you attempt, the more confidence you will develop. The important landmark to palpate is the greater trochanterof the femur. On a line between the tuber coxaeand the tuber ischii, the greater trochanter is located 3/4 of the distance (measured from cranial to caudal) towards the tuber ischii. The greater trochanter has cranial and caudal parts separated by a notch. The caudal part rises to a greater height than the cranial part, and it is more readily palpated. Deep palpation in a relaxed patient will allow palpation of the cranial part and sometimes in thinly muscled patients the notch separating the cranial and caudal parts can be recognized. In heavily muscled animals palpation of the anatomic landmarks can be difficult.
use an 18 gauge 6 inch spinal needle to inject the coxofemoral joint. The needle is inserted just proximal to the cranial part of the greater trochanterand is directed in a slightly distal cranial direction. In most adult horses approximately 5 inches of the needle will be necessary to enter the joint. The skin in this area is thick and can make penetration difficult. I routinely make a pilot hole with a 14 gauge needle to facilitate entry of the spinal needle. Aspiration should yield synovial fluid. Inject 25 ml of anesthetic into this joint. It is very helpful to having the horse standing squarely when performing this procedure.
External bony landmarks for entry site of the needle and needle advancement. Entry site of the needle is 2-cm cranial to the cranial aspect of the contralateral tuber sacrale (TS). The midpoint distance (X) of the line between the cranial aspect of the ipislateral tuber coxae (TC) and the cranial aspect of the greater trochanter of the femur is used as target for needle advancement (white line)
Fig. 3. Sacroiliac region from cranial with a needle placed adjacent to the sacroiliac joint. The 15-gauge, 25-cm-long spinal needle is advanced towards the dorsal sacrum (A) and along the iliac wing (B) to place medication adjacent to the medial sacroiliac joint margin (C).
Tarsus The tarsometatarsal joint is easiest to inject from the plantar lateral aspect o the horse above the head of the fourth metatarsal bone. There is a palpable small depression about 0 5 cm proximal to the head of the fourth metatarsal bone, approximately 1 cm dorsal to the edge of the superficial digital flexor tendon. A 20 gax 1 in. needle is directed in a distal, dorsomedial direction. Generally, the joint will readily accept approximately 4 ml of anesthetic. An additional two to four ml can be injected under pressure, which can increase communication with the distal intertarsal joint. When injected under pressure, there is also an increased tendency to have anesthetic flush back underneath the skin. To ensure completeness of the diagnostic anesthesia and therapeutic injections, routinely treat the tarsometatarsal and distal intertarsal joints as two separate joints.
The distal inter-tarsal joint is approached from the medial aspect of the distal tarsus. There is a depression between the third tarsal bone and the fused first and second tarsal bone that is bordered dorsally by the central tarsal bone.
Diagramatic example of an intra-artiular injection into the equine fetlock joint View of a fetlock (metacarpal/ metatarsophalangeal) joint injection.
COMPLICATIONS Complications following intra-articular injections are few local irritation, infection and needles breaking, could be encountered. The potential benefits of a joint injection are far- reaching; but, medicating joints can be expensive, might not result in the desired effect, and can potentially result in a post-injection complication such as joint flare, joint infection, and irreversible cartilage degeneration.
To help avoid infection always thoroughly clean the area, use good handling techniques and use disposable needles and syringes. Proper restraint of the animal as well as care in needle placement and handling is important in preventing needle breakage. To avoid post injection irritation, short term anti- inflammatory therapy for the animal may be prescribed and apply support wraps whenever indicated. Any horse with pain or swelling following any joint injection should be re-examined by a Veterinarian as soon as possible.








: usually has an")