Understanding Endometriosis: Causes and Effects
Endometriosis is a condition where tissue similar to the uterine lining grows outside the uterus, leading to various theories on its origin like implantation, metaplasia, and hormonal influence. This disorder poses challenges and requires proper diagnosis and treatment.

Uploaded on Oct 05, 2024 | 0 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
StudyMafia.Org ENDOMETRIOSIS Submitted To: Studymafia.org Submitted By: Studymafia.org
Table of Content Endometriosis Etiology Sites Of Endometriosis Chocolate Cyst Classification Clinical Features Differential Diagnosis Treatment Conclusion
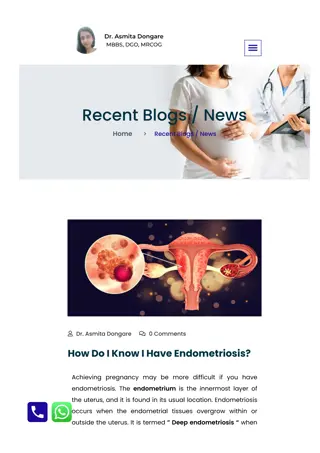
ENDOMETRIOSIS Endometriosis is a disorder in which tissue similar to the lining of your uterus grows outside of your uterine cavity. The lining of your uterus is called the endometrium. Endometriosis occurs when endometrial-like tissue grows on your ovaries, bowel, and tissues lining your pelvis. It s rare for endometrial-like tissue to spread beyond your pelvic region, but it s not impossible. Endometrial-like tissue growing outside of your uterus is known as an endometrial implant.
ETIOLOGY Various theories proposed to explain the histogenesis of endometriosis: 1)IMPLANTATION THEORY 2)COELOMIC METAPLASIA THEORY 3)INDUCTION THEORY 4)METASTATIC THEORY 5)HORMONAL INFLUENCE THEORY 6)IMMUNOLOGICAL THEORY
ETIOLOGY contd., Implantation theory: this theory explains that endometriosis is caused by implantation of endometrial cells by trans tubal retrograde menstruation. eg.1) Endometriosis in dependent portions of pelvis ovaries, uterosacral lig., cul-de-sac etc., 2) Scar endometriosis following classical caesarian section, hysterotomy & episiotomy.
ETIOLOGY contd., Coelomic Metaplasia theory: endometriosis arises as a result of metaplastic changes in embryonic cell rests of embryonic mesothelium which respond to hormonal stimulation. Induction theory: it proposes that an endogenous biochemical factor can induce undifferentiated peritoneal cells to develop into endometrial tissue.
ETIOLOGY contd., Metastatic theory: this thoery explains extra pelvic endometriosis which result from vascular or lymphatic dissemination of endometrial cells to gynaecological ( vulva, vagina, cervix) and non gynaecological sites like bowel, pelvic lymph nodes, ureter, lung, pleura etc. Hormonal Influence theory: after implantation development of endometriotic implants depend on presence of hormones mainly oestrogen.
ETIOLOGY contd., Immunological theory: endometriosis can be caused by decreased clearance of peritoneal fluid endometrial cells resulting from reduced Natural Killer cell activity or decreased macrophage activity.
Endometriosis symptoms Pelvic pain is the most common symptom of endometriosis. You may also have the following symptoms: painful periods cramps 1 or 2 weeks around menstruation heavy menstrual bleeding or bleeding between periods infertility pain during sexual intercourse discomfort with bowel movements lower back pain that may occur at any time during your menstrual cycle
SITES OF ENDOMETRIOSIS Most common site is ovary. Other sites cul-de-sac including uterosacral lig., back of uterus, posterior broad lig, peritoneum overlying bladder, intestinal coils etc., Scar endometriosis occur in umbilicus following laparotomy, tubal stumps following tubectomy, amputated stumps of cervix, episiotomy scars etc,
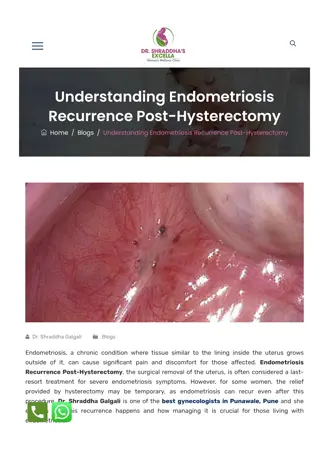
PATHOLOGY An endometriotic lesion appears as dark red, bluish or black cystic area adherent to site where it is lodged. Scarring around the lesion gives puckered appearance. Powder burnt areas represent inactive lesions.
BLUE BLACK APPEARANCE OF LESIONS
HISTOLOGY Histological confirmation is essential in the diagnosis of endometriosis. Microscopically, endometrial implants consist of endometrial glands & stroma with or without hemosiderin laden macrophages. Endometriod stroma is more characteristic of endometriosis than endometrial glands.
HISTOLOGY OF ENDOMETRIOTIC LESION
CHOCOLATE CYST OF OVARY Also called as endomeriotic cyst of ovary. Exclusive ovarian disease found in only 1% of patients. Ovarian endometriosis appears to be a marker of more extensive pelvic & intestinal disease. FORMATION OF CHOCOLATE CYST: Islets of endometriosis show cyclical changes during menstruation menstrual blood & debris collect collection with each episode absorption of fluid causes blood to become dark coloured to produce chocolate cyst.
CHOCOLATE CYST cont, Features of choclate cyst: 1.cyst diameter <12 cm 2.adhesion to pelvic side wall or broad lig 3.endometriosis on surface of ovary 4.contains tarry,thick,chocolate coloured fluid It consists of thick tunica albuginea & vascular red adhesions on undersurface of ovary.
CLASSIFICATION Revised American Fertility Society Classification Classification based on size & location of the endometriotic lesion. Classified as minimal, mild, moderate & severe. Classification correlated with fertility outcome rather than symptoms.
CLINICAL FEATURES SYMPTOMS: classical symptoms include dysmenorrhoea, dyspareunia & infertility. Dysmenorrhoea: usually congestive type. pain related to location not extent of lesion. Dyspareunia: involvement of cul-de-sac & uterosacral lig., produce adhesions & fixation of uterus. Movements of cervix elicit tenderness.
CLINICAL FEATURES Infertility: involvement of ovaries produce adhesions blocking tubo-ovarian motility & ovum pick up leading to infertility. Chronic pelvic pain: brownish yellow peritoneal fluid containing PGE2 is responsible for pain. Endocrinological abnormalities: anovulation, luteal insufficiency, lutenisation of unruptured follicle, hyperprolactinemia etc, Others: adhesions around ureter produce hydronephrosis, painful defaecation & melaena due to invol., of sigmoid colon.
ENDOMETRIOSIS LESIONS & ADHESIONS
CLINICAL FEATURES SIGNS: abdominal examination: may reveal tender & fixed cystic mass in case of chocolate cyst. Speculum examination: may reveal bluish or blackish puckered spots in posterior fornix. P/V: may reveal fixed tender retroverted uterus, cobble stone feel of uterosacral lig, thickened nodules in pouch of douglas etc,
DIFFERENTIAL DIAGNOSIS Pelvic inflammatory diseaes Uterine myomas Malignant ovarian disease with metastasis in pouch of douglas D.D of acute abdomen in case of ruptured chocolate cyst Chronic pelvic congestion syndrome Rectal carcinoma when involves rectovaginal septum
INVESTIGATIONS Ultrasound: TVS may reveal an echo free cyst whose wall is thick & irregular. Laparoscopy: laparoscopy is gold standard in the diagnosis of endometriosis. Histological confirmation CA125:it is a glycoprotein & cell surface antigen. Raised >35U/ml proportional to extent of disease. Raised level indicate recurrence or persistence of disease.
TREATMENT If asymptomatic observe for 6-8 months. Medical treatment : Indications: a) mild pelvic endometriosis b)to treat residual& recurrent disease following surgery OC PILLS: the objective of treatment is induction of amenorrhoea pseudo pregnancy & decidualisation of endometrial tissue which relieves pain & dysmenorrhoea. Dose :low dose OCP containing 30-35mcg of oestrogen for 6-12 months. PROGESTINS: considered as first choice for treatment of endometriosis with lower incidence of side effects.
TREATMENT DANAZOL: inhibits pituitary gonadotropins. It has anti-oestrogenic ,anti progestational & androgenic. Dose: 200-800mg for 3-6 months. GnRH ANALOGUES: cause atrophy of endometrial tissue AROMATASE INHIBITORS- letrozole MINIMALLY INVASIVE SURGERY: Goal of surgery is to excise all visible endometriotic lesion & associated adhesions & restore normal anatomy.
MINIMALLY INVASIVE SURGERY Ovarian endometrioma < 3cm in diameter removed by vapourisation by CO2 OR Nd:YAG laser. Ovarian cystectomy done for ovarian endometriotic cyst > 3 cm in diameter. Laparoscopic adhesiolysis: restore patency of tubes. LUNA(laparoscopic uterosacral nerve ablation): relieves pain.
LAPAROSCOPIC EXCISION OF ENDOMETRIOTIC CYST
TREATMENT LAPAROTOMY: presevered for advanced stage disease. Salpingo-oophorectomy Abd hysterectomy & bil salpingo-oophorectomy. COMBINED TREATMENT: pre operative medical treatment reduce vascularisation & size of nodules. post operative treatment decerase the incidence of recurrence.
PROPHYLAXIS Low dose OCP reduce endometrial growth & protect against endometriosis. Tubal patency tests should be avoided in immediate pre menstrual phase. Operations on the genital tract should be done in post menstrual phase. Classical c/s & hysterotomy may cause scar endometriosis & hence should be avoided.
CONLUSION Endometriosis is a chronic condition that s idiopathic, meaning what causes it has yet to be determined. And currently, it does not have a cure. However, effective treatments, such as medications, hormone therapy, and surgery, are available to help manage its side effects and complications like pain and fertility issues, respectively. And the symptoms of endometriosis usually improve after menopause.
References Google.com Wikipedia.org Studymafia.org Slidespanda.com
Thanks To StudyMafia.org