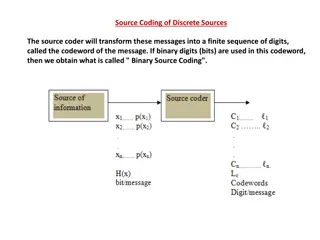
Understanding Changes in E&M Coding for 2021
Updates to E&M coding in 2021 include major changes in determining E&M codes based on time or medical decision making. The traditional codes have been revised and new guidelines have been introduced. Time can now be a key factor in selecting the appropriate E&M code, taking into account various aspects of patient care. Additionally, services that are reported separately need to be carefully managed to avoid duplication of time and efforts.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Disclaimer: updates Please note AMA and Medicare are currently updating the codes and the requirements It is expected that the codes will continue to be redefined as the AMA/Medicare encounter issues that occur with the use of the new codes
Major Changes Time or Medical Decision Making are now used to determine the E/M code Eliminates code 99201 Revised codes 99202-99215 Prolong service code changes for 99454-55 and 99356 and 99417
Changes to 2021 E/M codes History Exam Medical Decision Making Straight forward 99201 Prob. Focused Prob. Focused 99202 Exp. Prob. Focused Exp. Problem Focused Straight forward 99203 Detailed Detailed Low complex 99204 Comp. Hx. Comprehensive Moderate 99205 Comprehensive Comprehensive High complex
Based on Time Time may be used for in office /outpatient services whether or not counseling and/or coordination of care dominates the service BUT if the key element/dominating factor of the exam is counseling and or coordination of care TIME must be used, not Medical decision making.
What is included in TIME Includes face to face and non-face to face time Preparation( to see pt) such as review of test Obtain/review Separately obtained history Performing medically appropriate exam/evaluation/documentation Counseling/education of pt/family/caregiver Ordering meds/tests/procedures Referring/communicating with other Health care professionals WHEN NOT SEPERATELY REPORTED Independently interpreting results (WHEN NOT SEPERATELY REPORTED ) and communicating results to pt/family Care coordination ( NOT SEPERATELY REPORTED)
Services Reported Separately Any procedure code or service ( identified with a specific CPT code) performed on the date of the E/M service may be reported separately If reported separately, cannot include time for the testing and interpretation within the time for the E/M code Interpretation of tests/results with preparation of a separate distinctly identifiable written report can be reported separately with modifier 26 if required. Modifier 26 used when only professional component is being billed when services combine both the professional and technical portion in one procedure code
What Happens if test is not separately reported? Test/studies that independently interpreted in order to manage the patient as part of the E/M service but is not separately reported, becomes part of the Medical Decision Making
Guidelines: History and/or Evaluation Only a medically appropriate history and/or physical examination is need The treating physician determines the nature and extent of exam and/or history. The care team can collect the information and provide it directly to the reporting physician/qualified health care professional for review. Can be completed via questionnaire, portal
Code selection based on Time: Codes Time (does not incl. separate reported procedures) Codes Time (does not incl. separate reported procedures) 99211 99202 15-29 min 99212 10-19 min 99203 30-44 min 99213 20-29 min 99204 45-49 99214 30-39 min 99205 60-74 99215 40-54 min
Prolonged Services: Direct Contact 99354: direct face-to-face patient contact that requires one hour beyond the usual service, when billed on the same day by the same physician or qualified NPP Codes 99354-99357 ( inpt. and outpt.) cannot be used with 99202-99205 or 99211-99215 Can be used with consult codes Used for psychotherapy, domiciliary/rest home, home services, family/couples therapy For prolong service for office or outpatient services use 99417
Prolong Service Codes: Direct contact 99417: new prolong code use with 99205/99215 99415 Prolonged clinical staff service (the service beyond the highest time in the range of total time of the service) during an evaluation and management service in the office or outpatient setting, direct patient contact with physician supervision; first hour 99416 Prolonged clinical staff service (the service beyond the highest time in the range of total time of the service) during an evaluation and management service in the office or outpatient setting, direct patient contact with physician supervision; each additional 30 minutes DO NOT report 99354, 99355 with 99415,99416 or 99417
Prolong Services: without direct pt contact 99538 and 99539 can not be used with 99202-99205 or 99211- 99215 Can be reported on a different date than visit date 99417: prolong time with and without direct patient contact on the date of office or outpatient service Use with 99205 or 99215
99417 prolong time Used to report for prolonged total time ( with and without direct patient contact) provided by physician or qualified health care professional on the date of office or outpatient service Can only be used when service is coded based on time and only after total time exceeds the highest level of service (99205 or 99215) Reported in 15 min increments Recommend follow historical rule of 1/2 ; exceed the 7.5 min to reports** May be changed, some coders recommending coding at first minute over, waiting for AMA/CMS to confirm/update changes during the year Time spent on separate reported service is not counted toward 99205/99215 and prolong service time
Prolong time and new pts. Total Duration of New Patient Office or Other Outpatient Services (use with 99205) Codes <74 Not reported separately 75-89 min* 99205 1 unit and 99417 1 unit 90-104 min 99205 1 unit and 99417 2 unit 105 min or more 99205 1 unit and 99417 3 units or more for each additional 15 min *recommend reporting first unit once exceed 7.5 min, waiting on AMA/CMS to uphold or change during year
Prolong time and established pts. Total Duration of Established Patient office or other outpatient services ( use with 99215) Less than 55 min Codes Not reported separately 55-69 minutes* 99215 1 unit and 99417 1 unit 70-84 minutes 99215 1 unit and 99417 2 units 85 min or more 99215 1 unit and 99417 3 units or more for each additional 15 minutes *recommend reporting first unit once exceed 7.5 min, waiting on AMA/CMS to uphold or change during year
Complex PT code : GPC1X Visit complexity inherent to evaluation and management associated with medical care services that serve as the continuing focal point for all needed health care services and/or with medical care services that are part of ongoing care related to a patient s single, serious, or complex chronic condition. Add for primary care of medical care that is part of ongoing care related to single serious or complex chronic condition Can be used for specialty care CMS currently seeking feedback: not finalized
Elements for code selection: Medical Decision Making Number and complexity of Problems Addressed Amount and/or complexity of Data to be reviewed and analyzed Risk of complications and/or morbidity or mortality of patient management
Medical Decision Making Level (based on 2 of 3 elements) Number/compl exity of problems addressed Amount and/or complexity of data to be reviewed and analyzed Risks of complication and/or morbidity or mortality of patient management N/A 99211 N/A N/A N/A 99202/99212 Straightforward Minimal Minimal or none Minimal 99203/99213 low low Limited low 99204/99214 Moderate Moderate Moderate Moderate 99205/99215 High High Extensive High
MDM: number and complexity of problems addressed Minimal: 1 self limited or minor problem Low: 2 or more self limited problems or 1 stable chronic illness or 1 acute uncomplicated illness or injury
MDM: number and complexity of problem addressed Moderate: 1 or more chronic illness with exacerbation, progression or side effects of treatment OR 2 or more stable chronic illnesses or 1 undiagnosed new problem with uncertain prognosis OR 1 acute illness with systemic symptoms OR 1 acute complicated injury
MDM: number and complexity of problems addressed High 1 or more chronic illnesses with SEVERE exacerbation, progression or side effects of treatment OR 1 acute or chronic illness or injury that poses a threat to life or bodily function
New definitions/standards for medical decision making: Comorbidities/underlaying diseases are not considered in E/M selection unless there are ADDRESSED and the presence increases: Amount and/or complexity of data to be reviewed and analyzed OR Risk of complications and/or morbidity or mortality of patient management
What does addressed or managed mean To be addressed/managed it must be evaluated or treated at your encounter Physician can address/manage the disease, a symptom/sign, complaint etc. Diagnosis does not have to be established at the time of the visit Included testing or testing that cannot be performed due to ADR
When is it not addressed? If it is being managed by another provider and you are not providing additional assessment or care coordination that is does not qualify as being addressed/managed. If a referral is made without an evaluation or treatment considerations for the issue it is not considered addressed
Self limited or minor problem Runs a defined and prescribed course Transient in nature Not likely to alter health status permanently Example: Sub conjunctival Heme
What is a chronic illness? Chronic illnesses Stable: HTN- well controlled DM- well controlled Cataract ( yes listed specifically)
What is an acute uncomplicated illness or injury ? Recent or new short term problem Low risk of morbidity Full recovery expected without treatment Self limiting but not resolving as expected Examples: Allergic rhinitis Simple sprain
Illness with exacerbation progress or treatment side effect Chronic illness that is: Worsening Poorly controlled Progressing even though intent to control progression occurs Needs treatment for side effects
What is undiagnosed new problem with uncertain prognosis New problem Differential diagnosis that shows a high risk of morbidity without treatment Example: breast lump
Acute illness with systemic symptoms Under moderated MDM High risk of morbidity without treatment Systemic symptoms may be within a single system Does not have to be general symptoms I.e. fever body aches may be treated to eliminate the symptoms or shorten the illness or reduced complications are consider minor/acute and uncomplicated illness or injury IE: COLITIS, pyelonephritis pneumonitis
Acute complicated injury Moderate MDM Injury requiring treatment Needs evaluation of bodily systems not directly related to injury Injury is extensive Multiple treatment options possible Treatment option associated with morbidity
Example of chronic illness with severe exacerbation or progression Under High medical decision making Severe side effect of treatment with significant risk of morbidity May require hospital care/hospitalization
Illness or injury that poses a threat to bodily life or function Under high MDM Acute illness with systemic symptoms Acute complicated injury Chronic illness/injury with exacerbation or progression Side effects of treatment with threat to life or bodily function in near term without treatment Example: Acute renal failure Severe respiratory distress Psychiatric illness with potential self threat or threat to others
to qualify for E&M Addressed at visit Presence increases amount or complexity of dated to be reviewed Risk of complication morbidity or mortality of patient management
ELEMENT 2 : DATA Tests/documents/ orders or independent historian (each unique test id counted) Independent interpretation of tests performed by another physician or QHP that is not separately reported Discussion or management or test interpretation with external physician or QHP MD, OT, PT , O&M*
MDM: amount/complexity of Data to be reviewed or analyzed Minimal or none Limited: (must meet requirements or at least 1 of the 2 below) Cat 1 Test and documents: Any combination of 2 from the following Review of prior external notes from each unique source or Review of the result of each unique test OR Ordering of each unit test OR Cat 2 assessment requiring an independent historian Independent interpretation of a test performed by another physician/other qualified health care professional ( not separately reported) Discussion of management or testing interpretation with external physician/other qualified health care professional ( not separately reported)
MDM: amount/complexity of Data to be reviewed or analyzed Moderate: must meet at least one of the 3 categories cat 1: tests and documents, or indep historian Review of prior external notes rom each unique source Review of the result of each unique test Ordering of reach unique test Assessment requiring an independent historian OR Cat 2 independent interpretation of tests Indep interpretation of a test performing by another external physician/qualified health care provider ( not separately reported) OR Cat 3: discussion of management or test interpretation Discussion of management or test interpretation with external physician /QHCP appropriate source ( not separately reported)
MDM: amount/complexity of Data to be reviewed or analyzed Extensive (must meet 2 of 3 categories) cat 1: tests and documents, or indep historian Review of prior external notes rom each unique source Review of the result of each unique test Ordering of reach unique test Assessment requiring an independent historian OR Cat 2 independent interpretation of tests Indep interpretation of a test performing by another external physician/qualified health care provider ( not separately reported) OR Cat 3: discussion of management or test interpretation Discussion of management or test interpretation with external physician /QHCP appropriate source ( not separately reported)
Risk of complication and /or morbidity or mortality of patient management Straightforward: minimal risk of morbidity from additional diagnostic testing or treatment Low: low risk of morbidity from additional diagnostic testing or treatment
Risk of complication and /or morbidity or mortality of patient management Moderate: Ex: prescription drug management Decision regarding minor surgery with identified person or procedure risk factors Decision regarding elective surgery without identified patients patient or procedure risk factors Diagnosis or treatment significantly limited by social determinants of health
Risk of complication and /or morbidity or mortality of patient management HIGH: high risk of morbidity from additional diagnostic testing or treatment Ex: drug therapy requiring extensive monitoring for toxicity Decision regarding elective major surgery with identified patient or procedure risk factors Decision regarding emergency minor surgery Decision regarding hospitalization Decision not to resuscitate or to de-escalate care because of poor prognosis
RVU s Code 2020 work RVU 0.93 1.42 2.43 3.17 2021 work RVU 0.93 1.60 2.60 3.50 Additional codes 99241 99242 99243 99244 99245 2020 RVU 99202 99203 99204 99205 0.64 1.34 1.88 3.02 3.77 99211 99212 99213 99214 99215 99417 GPC1X 0.18 0.48 0.97 1.50 2.11 n/a n/a 0.18 0.70 1.30 1.92 2.80 0.61 0.33 92002 92004 92012 92014 0.88 1.82 0.92 1.42
CODING LOW VISION REHABILITATION EXAMINATION E&M Codes 99202-99215 Based on TIME or MDM Plus ophthalmic procedure codes If medically necessary Plus Rehabilitation Procedure codes Once the treatment plan has been established
MDM: Straightforward 99202 and 99212 Number and Complexity of Problems addressed Amount and/or Complexity of Data to be Reviewed and Analyzed Risk of complications and/or Morbidity or Mortality of patient management 1 self-limited or minor problem Minimal or none Minimal Risk Patient presents at risk for: -Effective gathering visual information -Inaccurate medication management -Inadequate management of chronic disease -Inadequate meal preparation ability/nutritional compromise -Inability to use telephone for emergencies -Ambulation/mobility compromise -Vision reduction in poor illumination -Vision reduction in outdoor illumination -Misidentification of faces -Misinterpretation of facial expressions -Social isolation -Financial mismanagement -Inability to store/recall vital information -Dual sensory impairment -Safe driving -Visual hallucinations (CBS) -Lack of social support -Travel difficulties Patient complains only of difficulty reading newsprint, blurred vision, no scotomas; minimal contrast sensitivity loss, no suspicion of depression. Problem resolved with higher add and/or light
MDM: Low 99203 and 99213 Number and Complexity of Problems addressed Amount and/or Complexity of Data to be Reviewed and Analyzed Cat1 (2) OR Cat2 Risk of complications and/or Morbidity or Mortality of patient management 2 or more self-limited or minor problem; OR 1 stable chronic illness; OR 1 acute, uncomplicated illness Minimal Risk Patient presents at risk for: -Effective gathering visual information -Inaccurate medication management -Inadequate management of chronic disease -Inadequate meal preparation ability/nutritional compromise -Inability to use telephone for emergencies -Ambulation/mobility compromise -Vision reduction in poor illumination -Vision reduction in outdoor illumination -Misidentification of faces -Misinterpretation of facial expressions -Social isolation -Financial mismanagement -Inability to store/recall vital information -Dual sensory impairment -Safe driving -Visual hallucinations (CBS) -Lack of social support -Travel difficulties Complains of difficulty reading all small print and seeing signs when driving. Small paracentral scotoma in one eye not interfering with fixation or reading, dense central scotoma in other; moderate contrast loss. Category 1: LV OD Reviewed prior external notes form each unique source And Reviewed Results of each unique test (ex: OCT, VF) Requires device for reading, filters, advice on driving, may require OT, scotoma training Category 2: LV OD independently interpreted a test performed by another physician (not separately reported)
MDM: Moderate 99204 and 99214 Number and Complexity of Problems addressed 1+ chronic illnesses with progression; OR 2+ stable chronic, OR 1 undiagnosed new with uncertain prognosis OR 1 acute with systemic symptoms OR 1 acute complicated injury Amount and/or Complexity of Data to be Reviewed and Analyzed Cat1 (3) OR Cat2 OR Cat 3 Risk of complications and/or Morbidity or Mortality of patient management Moderate Risk Patient presents at risk for: -Effective gathering visual information -Inaccurate medication management -Inadequate management of chronic disease -Inadequate meal preparation ability/nutritional compromise -Inability to use telephone for emergencies -Ambulation/mobility compromise -Vision reduction in poor illumination -Vision reduction in outdoor illumination -Misidentification of faces -Misinterpretation of facial expressions -Social isolation -Financial mismanagement -Inability to store/recall vital information -Dual sensory impairment -Safe driving -Visual hallucinations (CBS) -Lack of social support -Travel difficulties Category 1: LV OD Reviewed prior external notes form each unique source AND Reviewed Results of each unique test, OCT/VF AND Ordered additional test Category 2: LV OD independently interpreted a test performed by another physician (not separately reported) Category 3: LV OD discussed management or test results with external physician (not separately reported) Complains of difficulty with all reading, some ADLs at home, transportation, shopping; central or ring scotomas OU or paracentral in one eye interfering with reading; moderate to severe contrast loss; multiple medical issues (e.g., arthritis, risk of falls, CBS, hearing, depression); discouraged. Requires range of devices and filters; requires OT training. Education on driving, CBS
MDM: High 99205 and 99215 Number and Complexity of Problems addressed 1+ chronic illnesses with severe exacerbation, progression OR 1 acute or chronic illness or injury that poses a threat to life or bodily function Amount and/or Complexity of Data to be Reviewed and Analyzed Must meet at least 2 out of 3 categories Risk of complications and/or Morbidity or Mortality of patient management High Risk Patient presents at risk for: -Effective gathering visual information -Inaccurate medication management -Inadequate management of chronic disease -Inadequate meal preparation ability/nutritional compromise -Inability to use telephone for emergencies -Ambulation/mobility compromise -Vision reduction in poor illumination -Vision reduction in outdoor illumination -Misidentification of faces -Misinterpretation of facial expressions -Social isolation -Financial mismanagement -Inability to store/recall vital information -Dual sensory impairment -Safe driving -Visual hallucinations (CBS) -Lack of social support -Travel difficulties Category 1 (3): LV OD Reviewed prior external notes form each unique source AND Reviewed Results of each unique test (ex: OCT, VF) AND Ordered additional test Category 2: LV OD independently interpreted a test performed by another physician (not separately reported) Category 3: LV OD discussed management or test results with external physician (not separately reported) Complains of difficulty with all reading, ADLs at home, transportation, shopping; central scotomas OU; severe contrast loss; multiple medical issues as above; no support system and/or primary caretaker or spouse; high risk for depression; high risk for falling. Requires range of devices, strategies; requires OT training.