SWAG Cancer Alliance Rapid Diagnostic Services Implementation Plan


N
H
S
L
o
n
g
T
e
r
m
P
l
a
n
:
R
a
p
i
d
D
i
a
g
n
o
s
t
i
c
C
e
n
t
r
e
s
(
R
D
C
)
T
h
e
S
W
A
G
A
p
p
r
o
a
c
h
Patricia McLarnon, Programme Manager SWAG Cancer Alliance on
behalf of Dr Amelia Randle, Clinical Lead, SWAG Cancer Alliance

Rapid
Diagnostic
Service
•
By 2028 75% Cancers to be
diagnosed at Stage 1&2
•
67% of people with vague symptoms
are diagnosed at a late stage in
comparison to 45% for people
without vague symptoms (ACE
Programme, Multidisciplinary
Diagnostic Centre (MDC) based
pathways for patients with non-
specific but concerning symptoms:
Interim report)
•
Patients with vague symptoms are
more often diagnosed at an
emergency presentation (PHE-
Routes to diagnosis 2006-2015)
•
Absence of an optimal referral
pathway for patients presenting with
non-specific but concerning
symptoms and variation in standards
•
As SWAG is a rural Alliance one RDC will
not meet the needs of our diverse
population
•
The SWAG Cancer Alliance
would like to
support the development of Rapid
Diagnostic Services (RDS) providing
services to 30-50,000 patients within
Primary Care Networks (PCN)
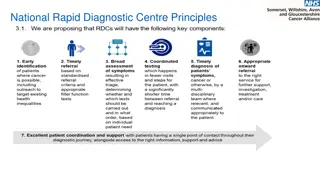
RDC Principals
•
A single point of access to a diagnostic
pathway for all patients with symptoms
that could indicate cancer
•
A personalised, accurate and timely
diagnosis of patients’ symptoms by
integrating existing diagnostic provision
and utilising networked clinical expertise
and information locally
4
1
.
T
h
e
p
r
o
b
l
e
m
•
Offer 45-minute appointment for eligible patients – providing comprehensive clinical assessment
including health and social assessment relevant to the patient’s efficient navigation of their forward
pathway. This assessment to be within the GP network geography providing the service for patients
close to their home.
•
Establish relationships with secondary care teams to enable rapid access to appropriate investigation
and multidisciplinary clinical advice. Investigations will be arranged in a streamlined way by
establishing provision with existing diagnostic services. e.g. ring-fenced CT slots available on the day
following the clinic.
•
Establish relationships with clinicians within the GP network to support early diagnosis of cancer and
appropriate referral to service.
•
Work with the Cancer Alliance to share outcomes from each of the sites to evolve the service provision
as we gain experience of what works well and, in due course, support roll out of services in
neighbouring networks.
•
T
h
e
c
l
i
n
i
c
a
l
l
e
a
d
c
o
u
l
d
b
e
a
G
P
,
c
o
n
s
u
l
t
a
n
t
o
r
A
l
l
i
e
d
H
e
a
l
t
h
p
r
o
f
e
s
s
i
o
n
a
l
a
n
d
c
o
u
l
d
b
e
e
m
p
l
o
y
e
d
b
y
p
r
i
m
a
r
y
o
r
s
e
c
o
n
d
a
r
y
c
a
r
e
.
T
h
e
i
n
i
t
i
a
l
a
s
s
e
s
s
m
e
n
t
w
i
l
l
b
e
p
r
o
v
i
d
e
d
w
i
t
h
i
n
t
h
e
n
e
t
w
o
r
k
g
e
o
g
r
a
p
h
y
e
i
t
h
e
r
G
P
p
r
a
c
t
i
c
e
o
r
o
t
h
e
r
p
r
o
v
i
d
e
r
s
u
c
h
a
s
a
l
o
c
a
l
h
o
s
p
i
t
a
l
i
f
l
o
c
a
t
e
d
w
i
t
h
i
n
t
h
e
n
e
t
w
o
r
k
.
E
a
c
h
R
D
S
s
e
r
v
i
c
e
w
i
l
l
h
a
v
e
a
l
e
a
d
c
l
i
n
i
c
i
a
n
w
h
o
w
i
l
l
:
5
1
.
T
h
e
p
r
o
b
l
e
m
Model 1
GP as providing service in their practice for patients in all network practices offering 45-minute
appointments on one day a week. GPs working in the practice identify appropriate patients and
book them directly into the slot leaving referral information to be accessed on the clinical
system. They will organise basic tests, so the results are available for this appointment. GP lead
clinician assesses patient in clinic slot, discusses with secondary care and/or arranges rapid
access to appropriate investigations at the local hospital.
Model 2
Acute trust within geography of three GP networks providing clinic at hospital outpatients for
all three networks with GPs referring according to agreed criteria. This gives potential for same
day investigation with e.g. CT.
Model 3
Advanced Nurse practitioner employed by acute trust provides clinical service for a number of
primary care networks – offering clinic slots at different GP practices on different days of the
week
P
o
t
e
n
t
i
a
l
s
e
r
v
i
c
e
m
o
d
e
l
s
B
e
n
e
f
i
t
s
NHS
Patient
Reduce 2WW
Optimised use of investigations
More efficient use of consultant, CNS and GP
time
Holistic care closer to home
Continuity of care
Multidisciplinary specialist opinion
Rapid investigations
Faster diagnosis
EOI to be submitted by 31
st
July 2019
STP Lead
Secondary care lead
PCN Lead
Brief outline of proposal / ideas. (You do
not need to have a full proposal at this
stage, enthusiasm to work with local
teams and develop a service is more
important but we would be interested to
hear your early thoughts on how this
may work within your network –
continued evaluation and evolution
throughout the pilots
Cost effective service to be
commissioned
8
1
.
T
h
e
p
r
o
b
l
e
m
O
p
p
o
r
t
u
n
i
t
i
e
s
f
o
r
h
a
e
m
a
t
o
l
o
g
y
T
o
b
e
c
r
e
a
t
i
v
e
f
o
r
t
h
i
s
p
a
t
i
e
n
t
c
o
h
o
r
t
T
o
t
r
a
n
s
f
o
r
m
a
n
d
b
e
i
n
v
o
l
v
e
d
i
n
d
e
s
i
g
n
i
n
g
t
h
e
s
e
s
e
r
v
i
c
e
s
–
1.
f
u
n
d
e
d
c
l
i
n
i
c
a
l
l
e
a
d
t
i
m
e
2.
p
r
o
v
i
d
e
c
l
i
n
i
c
a
l
e
x
p
e
r
t
i
s
e
t
o
t
h
e
R
D
S
d
e
s
i
g
n
C
o
n
t
a
c
t
S
T
P
c
a
n
c
e
r
l
e
a
d
o
r
D
r
A
m
e
l
i
a
R
a
n
d
l
e
a
m
e
l
i
a
.
r
a
n
d
l
e
@
n
h
s
.
n
e
t
Mobile: 07733101554
The SWAG Cancer Alliance aims to develop Rapid Diagnostic Services for patients with non-specific symptoms within Primary Care Networks. By 2028, the goal is to diagnose 75% of cancers at Stage 1 & 2, emphasizing personalized, timely diagnoses integrated with existing diagnostic provision. The approach includes a phased implementation over five years, ensuring a holistic diagnostic assessment and a single access point to diagnostic pathways for potential cancer symptoms.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
NHS Long Term Plan: Rapid Diagnostic Centres NHS Long Term Plan: Rapid Diagnostic Centres (RDC) (RDC) The SWAG Approach The SWAG Approach Patricia McLarnon, Programme Manager SWAG Cancer Alliance on behalf of Dr Amelia Randle, Clinical Lead, SWAG Cancer Alliance
By 2028 75% Cancers to be diagnosed at Stage 1&2 67% of people with vague symptoms are diagnosed at a late stage in comparison to 45% for people without vague symptoms (ACE Programme, Multidisciplinary Diagnostic Centre (MDC) based pathways for patients with non- specific but concerning symptoms: Interim report) Patients with vague symptoms are NHS England Service Specification (To be published mid July) 15% of Alliance Funds for 2019/20 to be spent on development of rapid diagnostic service for patients with serious but non-specific symptoms 900,000 for SWAG - The RDC vision will be achieved by taking a phased approach to implementation over a five-year period Rapid Diagnostic Service more often diagnosed at an emergency presentation (PHE- Routes to diagnosis 2006-2015) Absence of an optimal referral pathway for patients presenting with non-specific but concerning symptoms and variation in standards A personalised, accurate and timely diagnosis of patients symptoms via co-ordinated and rapid series of tests. integrating existing diagnostic provision and utilising networked clinical expertise and information locally (rad/path networks) Holistic Diagnostic Assessment Not a rule in- rule out service but get a diagnosis (28d) Single point of access to a diagnostic pathway for symptoms that could be cancer Participation in minimum dataset
As SWAG is a rural Alliance one RDC will not meet the needs of our diverse population Service to be delivered within PCNs pop 30,000 50,000 The SWAG Cancer Alliance would like to support the development of Rapid Diagnostic Services (RDS) providing services to 30-50,000 patients within Primary Care Networks (PCN) Money to be spent on clinical time and networking NHS England Spec estimates 80 patients / 100,000 per year = 24-40 per PCN RDC Principals A single point of access to a diagnostic pathway for all patients with symptoms that could indicate cancer A personalised, accurate and timely diagnosis of patients symptoms by integrating existing diagnostic provision and utilising networked clinical expertise and information locally Consider broadening scope to include 2ww referrals of limited clinical value Don t want to add additional unnecessary steps where further investigations clearly defined.
1. The problem Each RDS service will have a lead clinician who will: Offer 45-minute appointment for eligible patients providing comprehensive clinical assessment including health and social assessment relevant to the patient s efficient navigation of their forward pathway. This assessment to be within the GP network geography providing the service for patients close to their home. Establish relationships with secondary care teams to enable rapid access to appropriate investigation and multidisciplinary clinical advice. Investigations will be arranged in a streamlined way by establishing provision with existing diagnostic services. e.g. ring-fenced CT slots available on the day following the clinic. Opportunities Establish relationships with clinicians within the GP network to support early diagnosis of cancer and appropriate referral to service. Work with the Cancer Alliance to share outcomes from each of the sites to evolve the service provision as we gain experience of what works well and, in due course, support roll out of services in neighbouring networks. The clinical lead could be a GP, consultant or Allied Health professional and could be employed by primary or secondary care. The initial assessment will be provided within the network geography either GP practice or other provider such as a local hospital if located within the network.
1. The problem Potential service models Model 1 GP as providing service in their practice for patients in all network practices offering 45-minute appointments on one day a week. GPs working in the practice identify appropriate patients and book them directly into the slot leaving referral information to be accessed on the clinical system. They will organise basic tests, so the results are available for this appointment. GP lead clinician assesses patient in clinic slot, discusses with secondary care and/or arranges rapid access to appropriate investigations at the local hospital. Model 2 Opportunities Acute trust within geography of three GP networks providing clinic at hospital outpatients for all three networks with GPs referring according to agreed criteria. This gives potential for same day investigation with e.g. CT. Model 3 Advanced Nurse practitioner employed by acute trust provides clinical service for a number of primary care networks offering clinic slots at different GP practices on different days of the week
Benefits Benefits Holistic care closer to home Continuity of care Multidisciplinary specialist opinion Rapid investigations Faster diagnosis Reduce 2WW Optimised use of investigations More efficient use of consultant, CNS and GP time Patient NHS
EOI to be submitted by 31st July 2019 STP Lead Secondary care lead PCN Lead Aug - EOI review and agreed - RDS design + business plan 10K budget to support project planning and business case Brief outline of proposal / ideas. (You do not need to have a full proposal at this stage, enthusiasm to work with local teams and develop a service is more important but we would be interested to hear your early thoughts on how this may work within your network continued evaluation and evolution throughout the pilots Sept - set up event Dec pre-launch event GO LIVE Jan 1 2020 Cost effective service to be commissioned July 2020 celebration event
1. The problem Opportunities for haematology To be creative for this patient cohort To transform and be involved in designing these services 1. funded clinical lead time 2. provide clinical expertise to the RDS design Opportunities Contact STP cancer lead or Dr Amelia Randle amelia.randle@nhs.net Mobile: 07733101554