Drug-Induced Liver Injury (DILI) and Its Implications
Drug-Induced Liver Injury (DILI) is a serious concern that can lead to fatal liver damage, affecting drug development and potentially causing market withdrawal. This article explores the importance of DILI awareness, the critical functions of the liver, common causes of liver failure, and the background of DILI cases. Understanding DILI can help in identifying susceptible patients and mitigating risks associated with liver injuries caused by drugs.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Drug Induced Liver Injury Mary Ross Southworth, PharmD Division of Cardiovascular and Renal Products Office of New Drugs Center for Drug Evaluation and Research (CDER)
Why should we care about DILI? May cause serious or fatal liver injury Affects drug development Slow development Prevent approval Market withdrawal Identifying susceptible patients may mitigate risk 2 www.fda.gov
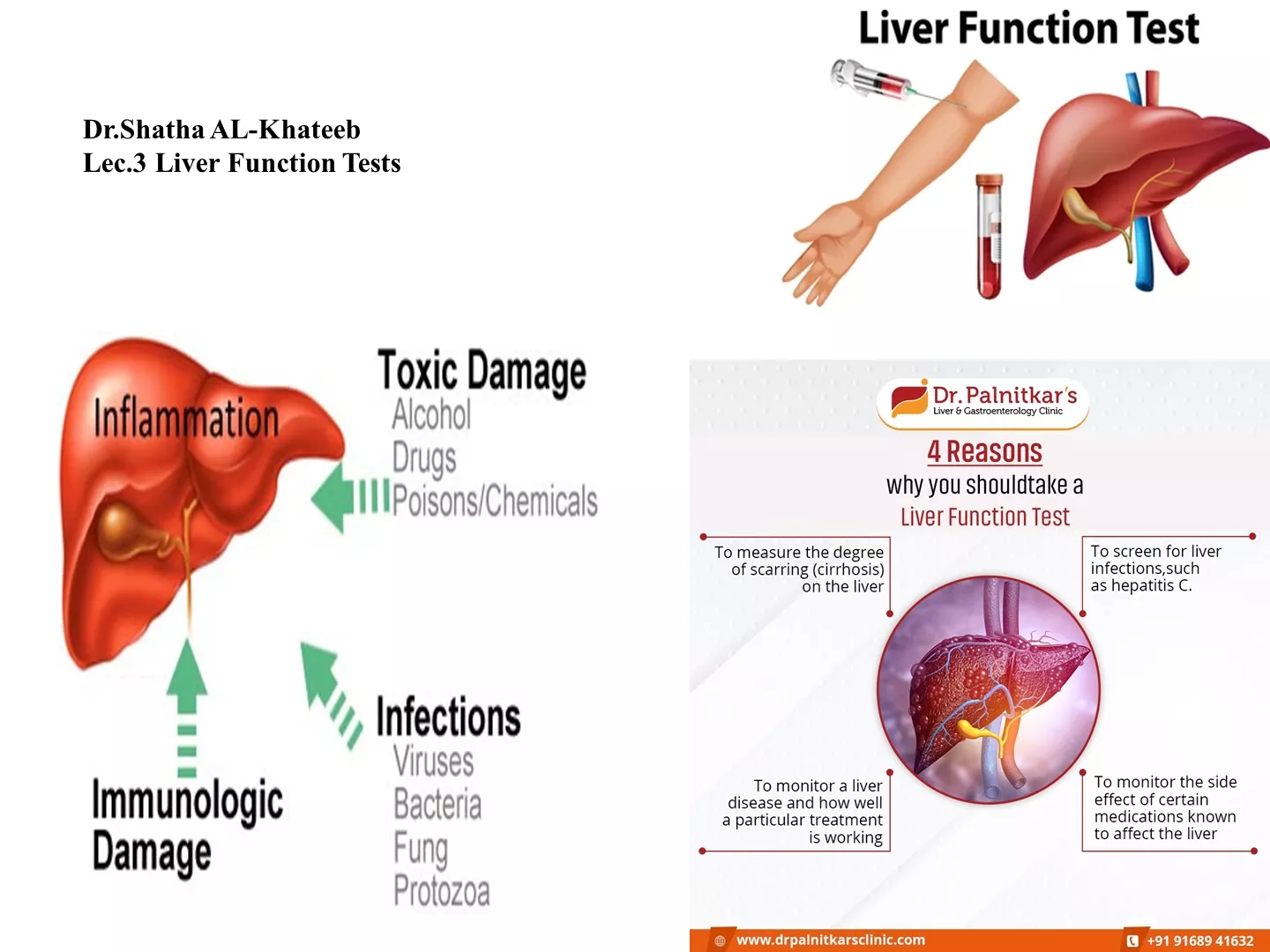
What does the liver do? Serves as the body s chemical engineering and control center Regulates the metabolism of internal compounds Processes compounds from external sources (drugs) Adaptable Can regrow even if 2/3 resected Regenerates rapidly if cells killed/removed Enzyme and transporter function can be altered 3
Common Causes of Acute Liver Failure Approved Drugs OTC Products (APAP) Alcohol 6
Drug Induced Liver Injury (DILI): Background Frequent cause of safety-related drug WITHDRAWALS or FAILURE TO APPROVE Bromfenac Troglitazone Ximelagatran Labeled WARNINGS Felbamate Isoniazid SPECIAL USE Bosentan Tolcapone 8
DILI: Background Drug Hepatotoxins usually cause hepatocellular injury Leakage of aminotransferase enzymes (AST/ALT) from injured liver No evidence of obstruction Drugs can also cause cholestasis Usually reversible Less morbid 9
DILI: Background Cases of severe DILI may not show up in the clinical drug development program Preclinical testing IDs overt hepatoxins Hepatotoxicity rare : 1 per 10,000 subjects Small numbers of patients studied, short duration What you may see: mild liver injuries but enzyme signals certain severe DILI 10
Severe DILI The ability to cause some hepatic injury is not a reliable predictor of potential for severe DILI Severe DILI=liver function affected NOT AST/ALT Bilirubin, PT Reaction often idiosyncratic Genetic factors? Metabolic factors? Concomitant diseases/drugs Nutritional status Alcohol use People are different ( tolerators , adaptors , susceptibles ) No predictive biomarker identified yet 11
Assessing signals of DILI in clinical trials Higher rate of enzyme elevation in drug vs. control group NOT specific, but still a signal Higher rate of marked enzyme elevations (>10x ULN; >1,000 U/L) More specific Hy s Law case Most specific Drug induced hepatocellular jaundice 10 to 50% mortality from ALF 12
Hys law: 3 Components Drug causes hepatocellular injury ( enzyme drug>control) Among those with enzyme elevations >3x ULN, some with serum total bilirubin >2x ULN, with no cholestasis ( No other reason can be found to explain the combination Requires clinical adjudication to determine probable cause of liver dysfunction! alk phos) 13
Detection and Clinical Evaluation of suspected DILI Detection Frequent monitoring in early clinical studies Symptoms may precede lab evidence! Confirmation/characterization Follow up testing in 48-72 hours; repeat liberally, as needed Obtain detailed history of symptoms Obtain complete medical and medication history Don t forget ETOH, OTC and herbals! GI consult as needed 14
Clinical Management of suspected DILI Drug discontinuation Automatically stopping drug with >3xULN increase may be unnecessary Liver can adapt and become tolerant Close observation warranted Prevent progression to functional impairment Generally, d/c drug if: ALT/AST > 8x ULN ALT/AST > 5x ULN for more than 2 weeks ALT/AST >3x ULN and (total bili >2x ULN or INR > 1.5) ALT/AST >3x ULN with symptoms 15
Clinical Management of suspected DILI Follow-up Follow until enzymes return to normal or baseline Symptoms and enzymes may progress even after discontinuation Bilirubin elevations usually follow enzyme elevations by days to weeks Rechallenge Can be considered Not for patients with significant enzymes (> 5x ULN) Not for patients with accompanying signs of an immunologic reaction 16
Gather more information to assess causality Evaluate alternative causes Acute viral hepatitis Alcoholic and autoimmune hepatitis Biliary tract disorders Cardiovascular causes Other uncommon causes Drug/Exposure history Dietary supplements, occupational exposure to toxic agents Remember the 3rd component of Hy s law: No other reason found for hepatotoxicity 17
Reporting DILI events to FDA Report potential Hy s law cases promptly Narrative summary of the event Include dates/times of symptoms, drug exposure Test results (include time course, normal ranges)\ Treatment provided Dechallenge/rechallenge Clinical assessment External expert consultants 18
DILI Risk: Questions with Regulatory Impact Does the drug cause clinically significant DILI in the target treatment population? What is the clinical signature of injury associated with the drug? What are the ranges of doses & duration are associated with increased risk? What are the critical patients susceptibility factors? What incidences of mild & severe liver injury can be predicted in large treatment population? 19
Take-away points for Investigators Individual susceptibility factors determine patient reaction No predictive markers validated Liver enzymes may indicate signal for risk But they do not measure liver function (bili; INR) Presence of one Hy s law case is concerning Not just lab values 20
Take-away points for investigators Handling enzyme elevations in clinical trials Sponsor should make sure investigators know what to do Confirm abnormality promptly Interrupt drug, if appropriate Close observation and documentation Investigate for probably cause Rule out viral/autoimmune hepatitis; alcohol; drugs Consult experts Follow course until resolution, record and report findings 21
Resources Guidance for Industry-Drug-Induced Liver Injury: Premarketing Clinical Evaluation http://www.fda.gov/downloads/Drugs/.../Guidances/UCM174090.pdf Livertox https://livertox.nih.gov/ Drug Induced Liver Injury Network http://www.dilin.org/ 22







:")