Clinical Management of a 66-Year-Old Male with COPD Exacerbation
A 66-year-old male with COPD presents with increased breathlessness, fatigue, confusion, and acute kidney injury. Using the CURB-65 and DECAF scores, appropriate treatment decisions are discussed based on severity assessment guidelines to optimize patient outcomes.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
SpR 2 SCE Questions Matt Dickson
Question 1 A 66 year old male with a background of COPD is admitted with increased breathlessness, fatigue and confusion. He has a respiratory rate of 30 breaths/minute, BP 91/65mmHg and blood results reveal high inflammatory markers and an acute kidney injury (creatinine 170, urea 10). His chest radiograph reveals left basal consolidation. He has no allergies. Which of the following statements is the most appropriate for this patient? a) He has a CURB-65 score of 1, and should be treated with IV Amoxicillin initially b) He has a CURB-65 score of 2, and should be treated with oral amoxicillin and clarithromycin c) He has a CURB-65 score of 3, and should be treated with IV Co-amoxiclav and Clarithromycin d) He has a CURB-65 score of 4, and should be treated with IV Co-amoxiclav and Clarithromycin e) He has a CURB-65 score of 4, and should be treated with IV Levofloxacin
Question 1 A 66 year old male with a background of COPD is admitted with increased breathlessness, fatigue and confusion. He has a respiratory rate of 30 breaths/minute, BP 91/65mmHg and blood results reveal high inflammatory markers and an acute kidney injury (creatinine 170, urea 10). His chest radiograph reveals left basal consolidation. He has no allergies. Which of the following statements is the most appropriate for this patient? a) He has a CURB-65 score of 1, and should be treated with IV Amoxicillin initially b) He has a CURB-65 score of 2, and should be treated with oral amoxicillin and clarithromycin c) He has a CURB-65 score of 3, and should be treated with IV Co-amoxiclav ad Clarithromycin d) He has a CURB-65 score of 4, and should be treated with IV Co-amoxiclav and Clarithromycin e) He has a CURB-65 score of 4, and should be treated with IV Levofloxacin
CURB-65 NICE guidance Low severity: PO Amoxicillin/Doxycycline/Clarithromyci n/Erythromycin for 5 days Moderate severity: PO Amoxicillin with Clarithromycin/Erythromycin or Doxycycline or Clarithromycin only (Penicillin allergic) High severity: PO/IV Co-amoxiclav with PO/IV Clarithromycin or PO Erythromycin or PO/IV Levofloxacin if penicillin allergic
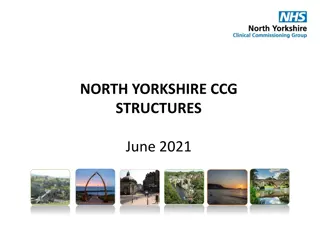
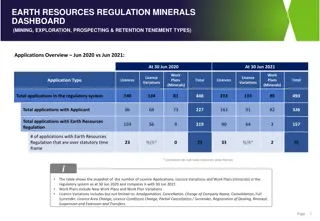
Question 2 A 66 year old male with a background of COPD (eMRCD 5a) is admitted with increased breathlessness, fatigue and confusion. He has a respiratory rate of 30 breaths/minute, BP 91/65mmHg and blood results reveal high inflammatory markers, eosinopenia of 0.02 and an acute kidney injury (creatinine 170, urea 10). His chest radiograph reveals left basal consolidation. He has no allergies. Which of the following statements is the most appropriate for this patient? a) He has a DECAF score of 1 and can be managed in the community b) He has a DECAF score of 2, with an inpatient mortality of up to 15% c) He has a DECAF score of 3, with an inpatient mortality of up to 35% d) He has a DECAF score of 4, with an inpatient mortality of up to 30% e) CURB-65 may over-estimate risk of mortality in this patient
Question 2 A 66 year old male with a background of COPD (eMRCD 5a) is admitted with increased breathlessness, fatigue and confusion. He has a respiratory rate of 30 breaths/minute, BP 91/65mmHg and blood results reveal high inflammatory markers, eosinopenia of 0.02 and an acute kidney injury (creatinine 170, urea 10). His chest radiograph reveals left basal consolidation. He has no allergies. Which of the following statements is the most appropriate for this patient? a) He has a DECAF score of 1 and can be managed in the community b) He has a DECAF score of 2, with an inpatient mortality of up to 15% c) He has a DECAF score of 3, with an inpatient mortality of up to 35% d) He has a DECAF score of 4, with an inpatient mortality of up to 30% e) CURB-65 may over-estimate risk of mortality in this patient
DECAF score CURB-65 score Actual mortality in pAECOPD Predicted from CURB-65 0-1 11.1% <3% 2 16% 3-15% 3-5 31.2% 28% Steer J, Gibson J, Bourke SC. The DECAF Score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax 2012;67:970-976. Steer J, Norman EM, Afolabi OA, et al. Dyspnoea severity and pneumonia as predictors of in-hospital mortality and early readmission in acute exacerbations of COPD. Thorax 2012;67:117-121.
Question 3 A 66 year old male with a background of COPD (eMRCD 5a) is admitted with increased breathlessness, fatigue and confusion. He has a respiratory rate of 30 breaths/minute, BP 91/65mmHg and blood results reveal high inflammatory markers, eosinopenia of 0.02 and an acute kidney injury (creatinine 170, urea 10). His chest radiograph reveals left basal consolidation. He has no allergies. In relation to bacterial pneumonia, which of the following statements is true? a) Haemophilus influenzae is responsible for the largest proportion of cases b) Streptococcus pneumoniae is a Gram +ve coccus, found in grape-like clusters c) Mycoplasma pneumoniae outbreaks occur every 10 years d) Moraxella catarrhalis is a Gram ve diplococcus e) Staphylococcus aureus pneumonia can complicate Influenza infection in ~20% of cases
Question 3 A 66 year old male with a background of COPD (eMRCD 5a) is admitted with increased breathlessness, fatigue and confusion. He has a respiratory rate of 30 breaths/minute, BP 91/65mmHg and blood results reveal high inflammatory markers, eosinopenia of 0.02 and an acute kidney injury (creatinine 170, urea 10). His chest radiograph reveals left basal consolidation. He has no allergies. In relation to bacterial pneumonia, which of the following statements is true? a) Haemophilus influenzae is responsible for the largest proportion of cases b) Streptococcus pneumoniae is a Gram +ve coccus, found in grape-like clusters c) Mycoplasma pneumoniae outbreaks occur every 10 years d) Moraxella catarrhalis is a Gram ve diplococcus e) Staphylococcus aureus pneumonia can complicate Influenza infection in ~20% of cases
Question 3 A 66 year old male with a background of COPD (eMRCD 5a) is admitted with increased breathlessness, fatigue and confusion. He has a respiratory rate of 30 breaths/minute, BP 91/65mmHg and blood results reveal high inflammatory markers, eosinopenia of 0.02 and an acute kidney injury (creatinine 170, urea 10). His chest radiograph reveals left basal consolidation. He has no allergies. In relation to bacterial pneumonia, which of the following statements is true? a) Streptococcus pneumoniae is responsible for the largest proportion of cases b) Staphylococcus aureus is a Gram +ve coccus, found in grape-like clusters c) Mycoplasma pneumoniae outbreaks occur every 4 years d) Moraxella catarrhalis is a Gram ve diplococcus e) Staphylococcus aureus pneumonia can complicate Influenza infection in ~3% of cases
Question 4 A 32 year old plumber presents with a 2 day history of headache, dry cough and fever. He has no evidence of consolidation on chest radiograph, his chest is clear, oxygen saturations are 98% on RA and given his employment history you suspect Legionella as the causative organism. Legionella urine antigen is positive. Which of the following statements is correct? a) Treatment with a fluoroquinolone is first line in this case b) Treatment with a macrolide is first line in this case c) He should self-isolate due to risk of transmission to others d) He does not require antibiotic treatment e) Legionella urine antigen has a sensitivity of 50%
Question 4 A 32 year old plumber presents with a 2 day history of headache, dry cough and fever. He has no evidence of consolidation on chest radiograph, his chest is clear, oxygen saturations are 98% on RA and given his employment history you suspect Legionella as the causative organism. Legionella urine antigen is positive. Which of the following statements is correct? a) Treatment with a fluoroquinolone is first line in this case b) Treatment with a macrolide is first line in this case c) He should self-isolate due to risk of transmission to others d) He does not require antibiotic treatment e) Legionella urine antigen has a sensitivity of 50%
Legionella Gram negative rod Non pneumonic disease (Pontiac fever) is self limiting Mild/moderate pneumonia Fluoroquinolone first line Macrolide second line Severe pneumonia Combination fluoroquinolone + macrolide Urine antigen test Sensitivity 80% Specificity >95%
Question 5 You are asked to review a patient admitted electively for a total hip replacement, whose surgery under general anaesthetic was performed 3 days ago. He has a new oxygen requirement, has raised inflammatory markers, fever and new patchy consolidation on a chest radiograph. With respect to nosocomial pneumonia, which statement is correct? a) Ventilator associated pneumonia is the second most common healthcare associated infection in ICU b) Ventilator associated pneumonia is the leading cause of death from healthcare associated infections c) Early onset HAP (<5 days) has a poorer prognosis than late onset (>5 days) d) Streptococcus pneumonia is the most common pathogen in early onset HAP (<5 days) e) Ventilator associated pneumonia is defined as developing 24 hours after intubation
Question 5 You are asked to review a patient admitted electively for a total hip replacement, whose surgery under general anaesthetic was performed 3 days ago. He has a new oxygen requirement, has raised inflammatory markers, fever and new patchy consolidation on a chest radiograph. With respect to nosocomial pneumonia, which statement is correct? a) Ventilator associated pneumonia is the second most common healthcare associated infection in ICU b) Ventilator associated pneumonia is the leading cause of death from healthcare associated infections c) Early onset HAP (<5 days) has a poorer prognosis than late onset (>5 days) d) Streptococcus pneumonia is the most common pathogen in early onset HAP (<5 days) e) Ventilator associated pneumonia is defined as developing 24 hours after intubation
Nosocomial pneumonia HAP Develops >48 hours from admission Represents ~20% of HAIs, but leading cause of death from HAIs Early onset usually caused by same organisms as CAP Late onset caused by hospital acquired organisms (e.g. Pseudomonas, MRSA) VAP Develops >48 hours after intubation Commonest HAI in ICU 2/3 mechanically ventilated for >48 hours will develop VAP Antibiotic choice should include coverage for anaerobes, MRSA, Legionella, Pseudomonas and Acinetobacter
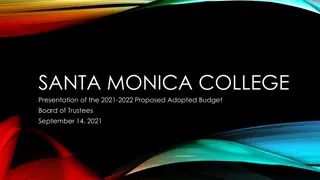
Question 6 A 55 year old homeless male with a history of alcohol dependence and intravenous drug abuse presents with new onset confusion, high fever, and productive cough and has evidence of a recent fall and head injury. He had received a 7 day course of co- amoxiclav from his GP without improvement. Sputum from the community has revealed Gram- positive bacilli with branching filaments. His imaging is adjacent:
Question 6 In relation to his presentation and disease, which of the following is correct? a) The organism is partially acid fast b) The organisms are present as part of normal flora of the mouth, GI tract and GU tract c) Blood culture is highly likely to be positive for the responsible organism d) IV Benzylpenicillin is the initial treatment of choice e) Treatment duration of 3 months is appropriate
Question 6 In relation to his presentation and disease, which of the following is correct? a) The organism is partially acid fast b) The organisms are present as part of normal flora of the mouth, GI tract and GU tract c) Blood culture is highly likely to be positive for the responsible organism d) IV Benzylpenicillin is the initial treatment of choice e) Treatment duration of 3 months is appropriate
Nocardiosis Gram positive, partially acid fast, aerobic bacilli that form branching filaments Pulmonary disease is the most frequent clinical presentation (approximately 50% of cases), and most of the infective organisms are from the Nocardia asteroides complex Non specific chest radiology consolidation, single/multiple nodules (sometimes cavitation), effusion Disseminated disease most commonly affects the central nervous system (CNS) and the skin Nocardia species are not part of the normal human flora Smear and culture principal method of diagnosis (sputum smear usually unhelpful, blood cultures almost always negative) Severe disease, treat with IV co-trimoxazole + carbapenem + aminoglycoside Non severe disease, treat with co-trimoxazole + fluoroquinolone or ceftriaxone or linezolid Treatment duration 6-12 months
Question 7 A 23 year old female presents with fever, cough, diarrhoea, rash and breathlessness 3 months post bone marrow transplantation. Her LFTs are deranged and she is leucopenic. In terms of the likely diagnosis for this patient, which of the following is true? a) Antibody testing would be helpful b) Infection occurs most frequently after 4 months post transplantation c) Oral valganciclovir would be first line d) Histology of infected tissue would reveal inclusion bodies e) Infection decreases risk of graft rejection
Question 7 A 23 year old female presents with fever, cough, diarrhoea, rash and breathlessness 3 months post bone marrow transplantation. Her LFTs are deranged and she is leucopenic. In terms of the likely diagnosis for this patient, which of the following is true? a) Antibody testing would be helpful b) Infection occurs most frequently after 4 months post transplantation c) Oral valganciclovir would be first line d) Histology of infected tissue would reveal inclusion bodies e) Infection decreases risk of graft rejection
Diagnosis of CMV pneumonitis Solid Organ Tranplant Recipients Risk assessment based on CMV serostatus of the donor and the recipient. Diagnosis based on pp65 antigenemia assay of whole blood, PCR based techniques of blood, plasma or PBMCs. End organ disease diagnosed by tissue immunohistopathology or in-situ techniques. HCST Recipients Risk assessment based on CMV serostatus of the donor and the recipient. Diagnosis based on pp65 antigenemia assay of whole blood (false positive results at low PBMC counts), PCR based techniques of blood, plasma or PBMCs. PCR or immunohistochemistry detection of the virus in BAL or lung biopsy. HIV/AIDS Patients Pp65 antigenemia of whole blood or CSF; Quantitative PCR of blood, plasma or PBMCs. Method Specimen Comments Serology Blood IgG only valuable for establishing past infection, IgM has poor sensitivity and specificity to detect recent infection Polymerase Chain Reaction (PCR) Blood, Urine, Saliva, tissue, Very sensitive, detects viral DNA and/or RNA, allows quantitation of viral load, not standardized

























![❤[PDF]⚡ Apollo Mission Control: The Making of a National Historic Landmark (Spr](/thumb/21551/pdf-apollo-mission-control-the-making-of-a-national-historic-landmark-spr.jpg)