CHIA USER WORKGROUP

C
H
I
A
U
S
E
R
W
O
R
K
G
R
O
U
P
CENTER FOR HEALTH INFORMATION AND ANALYSIS
Don Kirkwood (Manager of Data Release and Procurement)
Sylvia Hobbs (Manager of User Support)
Scott Curley (Manager Privacy & Compliance)
December 22, 2020


Announcements
:
APCD Release 8.0 Updates
FY19 Case Mix Release Projections
Data Release and Application Update
Website Updates
Application Reminders
User Support Questions
Casemix Knee/Hip Replacement Volume compared to MA APCD
Admission Source Codes
Emergency Department Busyness
Tracking Observation Stays
Principal Diagnosis
Principal Indicator
Race, Ethnicity and Hispanic Indicator
Visit Sequencing
Q&A
A
g
e
n
d
a
2
User Workgroup | CHIA User Support
A
v
a
i
l
a
b
l
e
N
O
W
Applicants with
approved projects
that require updated APCD
data (Release 8.0) should submit to CHIA a completed Exhibit B
(
Certificate of Continued Need and Compliance
) of the Data
Use Agreement. After submitting a completed Exhibit B you will
receive an invoice (if applicable) for the requested data. Upon
payment of the invoice the order for the data will be placed.
R
e
l
e
a
s
e
8
.
0
i
n
c
l
u
d
e
s
d
a
t
a
o
n
s
e
r
v
i
c
e
s
f
r
o
m
J
a
n
u
a
r
y
2
0
1
4
–
D
e
c
e
m
b
e
r
2
0
1
8
w
i
t
h
s
i
x
m
o
n
t
h
s
o
f
c
l
a
i
m
r
u
n
o
u
t
(
i
n
c
l
u
d
e
s
p
a
i
d
c
l
a
i
m
s
t
h
r
o
u
g
h
6
/
3
0
/
1
9
)
.
Will be linkable to Release 7.0 via crosswalk
Additional information on highlights and enhancements will be
presented in future APCD User Workgroups.
M
A
A
P
C
D
R
e
l
e
a
s
e
8
.
0
3
User Workgroup | CHIA User Support
*CURRENT* RELEASE TIMEFRAMES FOR EACH FILE:
Inpatient (HIDD)
A
v
a
i
l
a
b
l
e
f
o
r
r
e
q
u
e
s
t
a
n
d
d
e
l
i
v
e
r
y
Emergency Department (ED)
A
v
a
i
l
a
b
l
e
f
o
r
r
e
q
u
e
s
t
a
n
d
d
e
l
i
v
e
r
y
Outpatient Observation (OOD)
A
v
a
i
l
a
b
l
e
f
o
r
r
e
q
u
e
s
t
Applicants with
approved projects
that require newly available year(s) of Case Mix
Data (e.g., FY 19) should submit to CHIA a completed Exhibit B (
Certificate of
Continued Need and Compliance
) of the Data Use Agreement. After submitting a
completed Exhibit B you will receive an invoice (if applicable) for the requested
data. Upon payment of the invoice the order for the data will be placed.
C
a
s
e
M
i
x
F
Y
1
9
R
e
l
e
a
s
e
4
User Workgroup| CHIA User Support
Due to Governor Baker’s emergency actions to limit the spread of COVID-19 CHIA’s
workforce will be remote, for now. This arrangement will limit CHIA’s ability to produce
and deliver data extracts. At this time, CHIA is releasing data and providing extracts to
requestors.
During this time, CHIA will continue to accept and review data applications for both Case
Mix and All-Payer Claims Database (MA APCD) datasets. Review committees, DRC and
DPC, will continue their meetings remotely as necessary.
Due to CHIA’s physical office being closed, applications will be accepted without a fee.
After receipt of the application, CHIA will issue an invoice which will allow applicants to
remit payment online.
If you are a Data User that has a CHIA hard drive in your possession, please keep the
hard drive at this time while CHIA’s physical office is closed.
D
a
t
a
R
e
l
e
a
s
e
a
n
d
A
p
p
l
i
c
a
t
i
o
n
U
p
d
a
t
e
s
5
User Workgroup| CHIA User Support
U
p
d
a
t
e
s
o
n
t
h
e
p
r
o
d
u
c
t
i
o
n
o
f
A
P
C
D
a
n
d
C
a
s
e
M
i
x
d
a
t
a
b
a
s
e
s
a
n
d
s
t
a
t
u
s
o
f
d
a
t
a
r
e
q
u
e
s
t
s
a
r
e
n
o
w
p
o
s
t
e
d
t
o
C
H
I
A
’
s
w
e
b
s
i
t
e
!
A
i
m
#
1
i
s
t
o
p
r
o
v
i
d
e
w
e
e
k
l
y
o
r
b
i
-
w
e
e
k
l
y
s
t
a
t
u
s
u
p
d
a
t
e
o
n
C
H
I
A
d
a
t
a
p
r
o
d
u
c
t
s
a
s
t
h
e
y
a
r
e
i
n
d
e
v
e
l
o
p
m
e
n
t
.
A
i
m
#
2
i
s
t
o
p
r
o
v
i
d
e
a
p
p
l
i
c
a
n
t
s
w
i
t
h
i
n
f
o
r
m
a
t
i
o
n
a
b
o
u
t
e
x
p
e
c
t
e
d
f
u
l
f
i
l
l
m
e
n
t
s
t
a
t
u
s
f
o
r
i
n
d
i
v
i
d
u
a
l
d
a
t
a
r
e
q
u
e
s
t
s
.
Request IDs will be communicated to Data Requestors via email.
Please visit
http://www.chiamass.gov/status-of-data-requests/
to see
the current status of releases.
W
e
b
s
i
t
e
R
e
l
e
a
s
e
U
p
d
a
t
e
s
6
User Workgroup| CHIA User Support
A
P
P
L
I
C
A
T
I
O
N
R
E
M
I
N
D
E
R
S
1.
If you’re submitting a request for a fee waiver, remember to
include the fee remittance form in your application package on
IRBNet.
2.
Remember to submit supporting documentation (if required).
3.
If you’re requesting a financial hardship waiver, remember to
submit information detailing your project’s financial situation
(examples: project budget, grant funding, organizational /
departmental funding). Also request to pay a specific price
that you reasonably believe you’re able to afford to contribute.
4.
CHIA generally does not offer full financial hardship fee
waivers. We expect all applicants to have made an attempt to
find funding to cover the full cost of the data fees.
5.
Fee waiver requests can take some time to process –
especially financial hardship requests.
F
e
e
W
a
i
v
e
r
R
e
q
u
e
s
t
R
e
m
i
n
d
e
r
s
8
User Workgroup | CHIA User Support
Q
u
e
s
t
i
o
n
:
W
e
a
r
e
a
p
p
l
y
i
n
g
f
o
r
C
H
I
A
d
a
t
a
t
o
d
e
t
e
r
m
i
n
e
t
h
e
t
o
t
a
l
c
o
u
n
t
o
f
t
h
r
e
e
d
i
f
f
e
r
e
n
t
s
a
m
e
d
a
y
o
u
t
p
a
t
i
e
n
t
s
u
r
g
i
c
a
l
p
r
o
c
e
d
u
r
e
s
(
k
n
e
e
r
e
p
l
a
c
e
m
e
n
t
,
h
i
p
r
e
p
l
a
c
e
m
e
n
t
a
n
d
P
C
I
)
b
y
y
e
a
r
,
p
a
t
i
e
n
t
Z
I
P
c
o
d
e
,
a
n
d
f
a
c
i
l
i
t
y
.
B
e
f
o
r
e
s
u
b
m
i
t
t
i
n
g
o
u
r
a
p
p
l
i
c
a
t
i
o
n
,
w
o
u
l
d
i
t
b
e
p
o
s
s
i
b
l
e
t
o
d
e
t
e
r
m
i
n
e
t
h
e
t
r
a
d
e
-
o
f
f
i
n
r
e
l
y
i
n
g
o
n
j
u
s
t
k
n
e
e
r
e
p
l
a
c
e
m
e
n
t
s
,
h
i
p
r
e
p
l
a
c
e
m
e
n
t
s
a
n
d
P
C
I
s
a
s
r
e
p
o
r
t
e
d
i
n
t
h
e
c
a
s
e
m
i
x
o
u
t
p
a
t
i
e
n
t
o
b
s
e
r
v
a
t
i
o
n
s
t
a
y
d
a
t
a
v
e
r
s
u
s
o
u
t
p
a
t
i
e
n
t
p
r
o
c
e
d
u
r
e
s
a
s
r
e
p
o
r
t
e
d
i
n
t
h
e
M
A
A
P
C
D
?
Answer
:
One year (2018) of case mix outpatient observation stay
knee replacements
were compared to one year of MA APCD knee replacements. Of the 67 acute care hospitals
submitting outpatient observation stay data, 29 reported performing 301 knee replacements.
In the MA APCD, over 245 outpatient facilities (including orthopedic surgery centers, sports
medicine centers, ambulatory surgery centers and hospital outpatient medical groups)
performed over 21,000 knee replacements.
Likewise, one year of case mix observation stay
hip replacements
were compared to the
MA APCD. Of the 67 hospitals submitting observation stay data, 21 reported 159 hip
replacements. In the MA APCD, 342 outpatient facilities performed over 14,800 hip
replacements. As with knee replacements, using the MA APCD to analyze hip
replacements captured procedures performed at a wider variety of outpatient care
settings and therefore a higher volume of procedures.
Also, one year of observation stay
PCIs
were compared to the MA APCD. Of 67 hospitals,
20 reported performing 235 PCI procedures. In the MA APCD, 194 outpatient facilities
(including outpatient cardiology and cardiovascular centers, physician’s practice groups,
and hospital outpatient radiology and specialty centers) performed over 9,000 procedures.
Therefore, the case mix observation stay data alone would not allow you to achieve your
study goal to validate the outpatient volume of the three procedures of interest. The
MA APCD captures care provided in any setting for which a carrier submits claims to CHIA.
Q
u
e
s
t
i
o
n
:
I
n
c
r
e
a
t
i
n
g
a
f
l
a
g
f
o
r
E
D
a
c
t
i
v
i
t
y
,
w
e
e
x
p
a
n
d
e
d
o
n
t
h
e
C
H
I
A
E
D
f
l
a
g
t
o
i
n
c
l
u
d
e
a
d
m
i
s
s
i
o
n
s
o
u
r
c
e
=
R
(
w
i
t
h
i
n
h
o
s
p
i
t
a
l
e
m
e
r
g
e
n
c
y
r
o
o
m
t
r
a
n
s
f
e
r
)
a
n
d
t
h
e
v
a
r
i
o
u
s
r
e
v
e
n
u
e
c
o
d
e
s
y
o
u
s
u
g
g
e
s
t
e
d
i
n
t
h
e
P
P
T
o
n
y
o
u
r
w
e
b
s
i
t
e
.
D
o
y
o
u
a
l
s
o
s
u
g
g
e
s
t
i
n
c
o
r
p
o
r
a
t
i
n
g
E
D
r
e
g
i
s
t
r
a
t
i
o
n
d
a
t
e
f
i
e
l
d
o
r
a
d
m
i
s
s
i
o
n
s
o
u
r
c
e
=
7
(
o
u
t
s
i
d
e
h
o
s
p
i
t
a
l
e
m
e
r
g
e
n
c
y
r
o
o
m
t
r
a
n
s
f
e
r
)
?
Answer
:
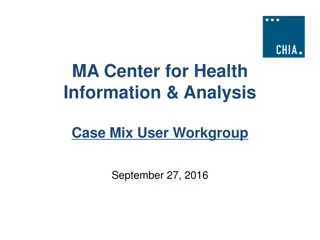
FY2018 Hospital Inpatient Discharge Data has 809,270 discharges. When you compare the fields that can be used
to indicate whether a patient was admitted through the ED, the revenue code 450 (the billing code for utilization of
emergency room services) appeared on 59% of the discharge records, followed by ED Registration Date on 51% of the
discharges, ED Flag Code 2 on 40%, and primary or secondary admission source 16% (
See Figure 1 below
). Therefore, the
two most reliable indicators appear to be 450 revenue code and ED registration data. The use of admission source ‘7’
(outside hospital emergency room transfer) depends on your study. Some studies distinguish how they analyze interfacility
transfers where there may a different type of delay in reaching definitive care from within hospital admissions.
Q
u
e
s
t
i
o
n
:
S
i
m
i
l
a
r
l
y
,
i
f
w
e
w
a
n
t
e
d
t
o
a
n
a
l
y
z
e
p
a
t
i
e
n
t
s
w
h
o
a
r
e
a
d
m
i
t
t
e
d
t
h
r
o
u
g
h
o
b
s
e
r
v
a
t
i
o
n
s
t
a
y
t
o
i
n
p
a
t
i
e
n
t
h
o
s
p
i
t
a
l
i
z
a
t
i
o
n
,
w
h
a
t
f
i
e
l
d
s
h
o
u
l
d
w
e
u
s
e
t
o
e
n
s
u
r
e
t
h
a
t
w
e
h
a
v
e
f
i
l
t
e
r
e
d
f
o
r
a
l
l
s
u
c
h
p
a
t
i
e
n
t
s
?
Answer
:
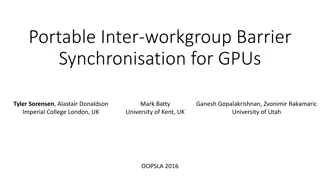
Hospitals report observation room charges under revenue code 762. However, if the
patient has been seen in Observation as well as another outpatient department and is then
admitted, hospitals use Revenue Code 762 and use the alternate outpatient department as the
admission source. Since this is frequently the case with observation stay patients, you will find a
small number of discharges with source code ‘X’ for observation admission source (see Figure 2
below) and a larger number with Revenue Code 762 and Observation Stay Flag indicating ‘Yes’. It is
important to note that the revenue code units of service are reported in hours and a patient might
have a longer observation stay, say 48 hours, than inpatient length of say, which could be only 1 day
.
ED Surge Volume
ED Surge Volume
Q
u
e
s
t
i
o
n
:
I
s
c
a
s
e
m
i
x
d
a
t
a
o
n
i
n
p
a
t
i
e
n
t
h
o
s
p
i
t
a
l
i
z
a
t
i
o
n
s
(
a
n
d
E
D
u
s
e
)
d
a
t
e
d
i
n
s
u
c
h
a
w
a
y
t
h
a
t
y
o
u
c
a
n
a
s
s
e
s
s
t
h
e
b
u
s
y
n
e
s
s
o
f
a
h
o
s
p
i
t
a
l
o
r
E
D
a
t
a
s
p
e
c
i
f
i
c
t
i
m
e
p
e
r
i
o
d
?
?
Answer
:
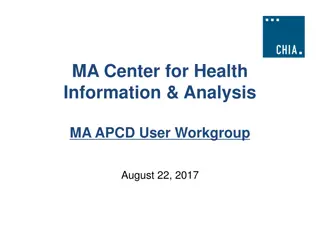
The emergency department registration times are not released as part of the
limited data set to non-government researchers. However, in both the ED Visit data and
now as part of the hospital inpatient discharge data, the ED registration date can be
requested by non-government applicants.
The ED Visit data does however include a length of stay in hours and this field can be
requested by non-government applicants. The length of stay in hours, date and patient
visit volume does enable simulating seasonal surge models and looking at the
relationship between patient volume and days on which specific patient volumes begin
to hit the 24-hour ceiling. For example, while Figure 1 below shows FY2018 outpatient
ED visit volume by length of stay in hours, the same annual comparison can be made
by quarters, months, weeks, or days.
Q
u
e
s
t
i
o
n
:
T
h
e
E
D
d
a
t
a
c
o
n
t
a
i
n
s
V
i
s
i
t
S
e
q
u
e
n
c
e
v
a
r
i
a
b
l
e
a
n
d
a
S
e
q
u
e
n
c
e
v
a
r
i
a
b
l
e
.
C
a
n
y
o
u
e
x
p
l
a
i
n
t
h
e
d
i
f
f
e
r
e
n
c
e
?
I
o
n
l
y
s
e
e
S
e
q
u
e
n
c
e
v
a
r
i
a
b
l
e
s
i
n
t
h
e
E
D
p
r
o
c
e
d
u
r
e
a
n
d
d
i
a
g
n
o
s
i
s
t
a
b
l
e
s
,
b
u
t
V
i
s
i
t
S
e
q
u
e
n
c
e
o
n
l
y
i
n
t
h
e
m
a
i
n
E
D
V
i
s
i
t
.
Answer
:
For patients who had multiple ED visits within a year, the Visit Sequence variable in the main ED visit table
indicates the sequence of the patient’s visit based on the date when their specific UHIN appeared first within that
year’s release. As you can see in Figure 1 below, the majority of patients just have only one visit. The term sequence in
the diagnosis and procedure codes field is simply how hospitals order each subsequent associated codes after the first
diagnosis and first procedure.
Q
u
e
s
t
i
o
n
:
W
e
f
o
u
n
d
t
h
e
p
r
i
n
c
i
p
a
l
d
i
a
g
n
o
s
i
s
c
o
d
e
s
i
s
s
o
m
e
t
i
m
e
s
l
i
s
t
e
d
i
n
b
o
t
h
t
h
e
m
a
i
n
t
a
b
l
e
a
n
d
t
h
e
s
e
p
a
r
a
t
e
d
i
a
g
n
o
s
i
s
t
a
b
l
e
f
o
r
i
n
p
a
t
i
e
n
t
a
n
d
E
D
d
a
t
a
,
b
u
t
i
n
m
a
n
y
t
i
m
e
s
o
n
t
h
e
E
D
s
i
d
e
i
t
i
s
n
o
t
l
i
s
t
e
d
i
n
b
o
t
h
p
l
a
c
e
s
–
d
o
y
o
u
k
n
o
w
w
h
y
t
h
i
s
i
s
t
h
e
c
a
s
e
?
Answer
:
Hospitals report an admitting diagnosis, principal diagnosis, and discharge diagnosis which CMS defines
as follow:
•
Admitting Diagnosis -
patient's initial diagnosis at the time of admission
•
Principal Diagnosis – the diagnosis chiefly responsible for the medical services provided
•
Discharge Diagnosis – patient’s final diagnosis at the time of discharge
There are instances when the admitting diagnosis rendered before any diagnostic tests have been run, is the same
at the principal diagnosis and discharge diagnosis. The admitting diagnosis and discharge diagnosis are used to
generate separate DRGs.
You do typically see this duplication in ED data because the ED setting is outpatient care where the patient receives
care without being admitted. DRGs are not run on ED Data.
Q
u
e
s
t
i
o
n
:
C
a
n
y
o
u
d
i
s
c
u
s
s
t
h
e
R
a
c
e
,
E
t
h
n
i
c
i
t
y
,
H
i
s
p
a
n
i
c
I
n
d
i
c
a
t
o
r
a
n
d
t
h
e
d
i
f
f
e
r
e
n
c
e
s
b
e
t
w
e
e
n
t
h
e
m
i
n
t
h
e
d
a
t
a
?
Answer
:
Race is a system of labelling that provides a source of identity
and has the following five categories provided by the CDC: American
Indian or Alaska Native, Asian, Black or African American, Native
Hawaiian or Other Pacific Islander, and White.
Ethnicity is a term that describes shared culture, including practices,
values, and beliefs of a group. Collection of ethnicity data depends on the
questions asked and the format of the questions, which in turn, depends
on the system’s field capacity. CHIA adheres to the OMB guidance, using a
two-question format, which includes the Hispanic ethnicity question, and
then, granular ethnicity.
Hence, the Case Mix data has the Hispanic Indicator flag variable that
determines whether or not a patient is Hispanic or Latino regardless of
race, the majority of patients just have only one visit. The term sequence
in the diagnosis and procedure codes field is simply how hospitals order
each subsequent associated codes after the first diagnosis and first
procedure.
U
S
E
R
Q
U
E
S
T
I
O
N
S
http://www.chiamass.gov/ma-apcd-and-case-mix-user-workgroup-
information/
W
h
e
r
e
c
a
n
I
f
i
n
d
p
a
s
t
U
s
e
r
W
o
r
k
g
r
o
u
p
P
r
e
s
e
n
t
a
t
i
o
n
s
?
17
User Workgroup | CHIA User Support
W
h
e
n
i
s
t
h
e
n
e
x
t
U
s
e
r
G
r
o
u
p
m
e
e
t
i
n
g
?
•
The next User Group will meet Tuesday, January
26.
•
http://www.chiamass.gov/ma-apcd-and-case-mix-user-workgroup-
information/
Questions related to MA APCD:
apcd.data@state.ma.us
Questions related to Case Mix:
casemix.data@state.ma.us
R
E
M
I
N
D
E
R
:
P
l
e
a
s
e
i
n
c
l
u
d
e
y
o
u
r
I
R
B
N
e
t
I
D
#
,
i
f
y
o
u
c
u
r
r
e
n
t
l
y
h
a
v
e
a
p
r
o
j
e
c
t
u
s
i
n
g
C
H
I
A
d
a
t
a
.
Q
u
e
s
t
i
o
n
s
?
19
User Workgroup | CHIA User Support
I
f
t
h
e
r
e
i
s
a
T
O
P
I
C
t
h
a
t
y
o
u
w
o
u
l
d
l
i
k
e
t
o
s
e
e
d
i
s
c
u
s
s
e
d
a
t
a
n
M
A
A
P
C
D
o
r
C
a
s
e
M
i
x
w
o
r
k
g
r
o
u
p
i
n
2
0
2
1
,
c
o
n
t
a
c
t
A
m
y
W
y
e
t
h
[
a
m
y
.
w
y
e
t
h
@
s
t
a
t
e
.
m
a
.
u
s
]
I
f
y
o
u
a
r
e
i
n
t
e
r
e
s
t
e
d
i
n
P
R
E
S
E
N
T
I
N
G
a
t
a
M
A
A
P
C
D
o
r
C
a
s
e
M
i
x
w
o
r
k
g
r
o
u
p
i
n
2
0
2
1
,
c
o
n
t
a
c
t
A
m
y
W
y
e
t
h
[
a
m
y
.
w
y
e
t
h
@
s
t
a
t
e
.
m
a
.
u
s
]
You can present remotely, or in-person at CHIA
We may be reaching out to some data users with invitations to
present, and hope you will consider this!
C
a
l
l
f
o
r
T
o
p
i
c
s
a
n
d
P
r
e
s
e
n
t
e
r
s
20
User Workgroup | CHIA User Support
The CHIA User Workgroup agenda encompasses important announcements and updates regarding APCD Release 8.0, FY19 Case Mix Release Projections, data release and application updates. The agenda covers a range of topics including user support, casemix comparisons, admission source codes, emergency department tracking, and more. It also highlights the availability of MA APCD Release 8.0 and Case Mix FY19 Release, with information on data timeframes and submission processes. Additionally, it addresses changes in data release and application procedures due to COVID-19, emphasizing remote work arrangements and continued data processing operations by CHIA.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
CHIA USER WORKGROUP Don Kirkwood (Manager of Data Release and Procurement) Sylvia Hobbs (Manager of User Support) Scott Curley (Manager Privacy & Compliance) December 22, 2020 CENTER FOR HEALTH INFORMATION AND ANALYSIS
Agenda Announcements: APCD Release 8.0 Updates FY19 Case Mix Release Projections Data Release and Application Update Website Updates Application Reminders User Support Questions Casemix Knee/Hip Replacement Volume compared to MA APCD Admission Source Codes Emergency Department Busyness Tracking Observation Stays Principal Diagnosis Principal Indicator Race, Ethnicity and Hispanic Indicator Visit Sequencing Q&A 2 User Workgroup | CHIA User Support
MA APCD Release 8.0 Available NOW Applicants with approved projects that require updated APCD data (Release 8.0) should submit to CHIA a completed Exhibit B (Certificate of Continued Need and Compliance) of the Data Use Agreement. After submitting a completed Exhibit B you will receive an invoice (if applicable) for the requested data. Upon payment of the invoice the order for the data will be placed. Release 8.0 includes data on services from January 2014 December 2018 with six months of claim runout (includes paid claims through 6/30/19). Will be linkable to Release 7.0 via crosswalk Additional information on highlights and enhancements will be presented in future APCD User Workgroups. 3 User Workgroup | CHIA User Support
Case Mix FY19 Release *CURRENT* RELEASE TIMEFRAMES FOR EACH FILE: Inpatient (HIDD) Available for request and delivery Emergency Department (ED) Available for request and delivery Outpatient Observation (OOD) Applicants with approved projects that require newly available year(s) of Case Mix Data (e.g., FY 19) should submit to CHIA a completed Exhibit B (Certificate of Continued Need and Compliance) of the Data Use Agreement. After submitting a completed Exhibit B you will receive an invoice (if applicable) for the requested data. Upon payment of the invoice the order for the data will be placed. Available for request 4 User Workgroup| CHIA User Support
Data Release and Application Updates Due to Governor Baker s emergency actions to limit the spread of COVID-19 CHIA s workforce will be remote, for now. This arrangement will limit CHIA s ability to produce and deliver data extracts. At this time, CHIA is releasing data and providing extracts to requestors. During this time, CHIA will continue to accept and review data applications for both Case Mix and All-Payer Claims Database (MA APCD) datasets. Review committees, DRC and DPC, will continue their meetings remotely as necessary. Due to CHIA s physical office being closed, applications will be accepted without a fee. After receipt of the application, CHIA will issue an invoice which will allow applicants to remit payment online. If you are a Data User that has a CHIA hard drive in your possession, please keep the hard drive at this time while CHIA s physical office is closed. 5 User Workgroup| CHIA User Support
Website Release Updates Updates on the production of APCD and Case Mix databases and status of data requests are now posted to CHIA s website! Aim #1 is to provide weekly or bi-weekly status update on CHIA data products as they are in development. Aim #2 is to provide applicants with information about expected fulfillment status for individual data requests. Request IDs will be communicated to Data Requestors via email. Please visit http://www.chiamass.gov/status-of-data-requests/ to see the current status of releases. User Workgroup| CHIA User Support 6
Fee Waiver Request Reminders 1. If you re submitting a request for a fee waiver, remember to include the fee remittance form in your application package on IRBNet. Remember to submit supporting documentation (if required). If you re requesting a financial hardship waiver, remember to submit information detailing your project s financial situation (examples: project budget, grant funding, organizational / departmental funding). Also request to pay a specific price that you reasonably believe you re able to afford to contribute. CHIA generally does not offer full financial hardship fee waivers. We expect all applicants to have made an attempt to find funding to cover the full cost of the data fees. Fee waiver requests can take some time to process especially financial hardship requests. 2. 3. 4. 5. 8 User Workgroup | CHIA User Support
Question Question: We are applying for CHIA data to determine the total count of : We are applying for CHIA data to determine the total count of three outpatient surgical procedures (knee replacement, hip replacement and PCI) by outpatient surgical procedures (knee replacement, hip replacement and PCI) by year, facility facility. . Before submitting our application Before submitting our application, , would would it be possible to determine the trade knee replacements, hip replacements and PCIs as knee replacements, hip replacements and PCIs as reported in the case mix outpatient observation stay reported in the case mix outpatient observation stay data versus outpatient procedures versus outpatient procedures as reported in the MA APCD as reported in the MA APCD? ? three different same different same day year, patient patient ZIP code, off in relying on day ZIP code, and relying on just and just data it be possible to determine the trade- -off in Knee Replacement Answer: One year (2018) of case mix outpatient observation stay knee replacements were compared to one year of MA APCD knee replacements. Of the 67 acute care hospitals submitting outpatient observation stay data, 29 reported performing 301 knee replacements. In the MA APCD, over 245 outpatient facilities (including orthopedic surgery centers, sports medicine centers, ambulatory surgery centers and hospital outpatient medical groups) performed over 21,000 knee replacements. Likewise, one year of case mix observation stay hip replacements were compared to the MA APCD. Of the 67 hospitals submitting observation stay data, 21 reported 159 hip replacements. In the MA APCD, 342 outpatient facilities performed over 14,800 hip replacements. As with knee replacements, using the MA APCD to analyze hip replacements captured procedures performed at a wider variety of outpatient care settings and therefore a higher volume of procedures. Hip Replacement Also, one year of observation stay PCIs were compared to the MA APCD. Of 67 hospitals, 20 reported performing 235 PCI procedures. In the MA APCD, 194 outpatient facilities (including outpatient cardiology and cardiovascular centers, physician s practice groups, and hospital outpatient radiology and specialty centers) performed over 9,000 procedures. Therefore, the case mix observation stay data alone would not allow you to achieve your study goal to validate the outpatient volume of the three procedures of interest. The MA APCD captures care provided in any setting for which a carrier submits claims to CHIA.
Question Question: : I In n creating a flag for ED activity, we expanded creating a flag for ED activity, we expanded on the CHIA ED ED flag to include admission flag to include admission source = R ( source = R (within room transfer) and room transfer) and the various revenue the various revenue codes incorporating incorporating ED registration ED registration date field or admission date field or admission source=7 on the CHIA within hospital emergency hospital emergency codes you suggested in the PPT on your you suggested in the PPT on your website. Do you also source=7 ( (o outside utside h hospital website. Do you also suggest ospital e emergency mergency r room transfer)? suggest oom transfer)? Answer: FY2018 Hospital Inpatient Discharge Data has 809,270 discharges. When you compare the fields that can be used to indicate whether a patient was admitted through the ED, the revenue code 450 (the billing code for utilization of emergency room services) appeared on 59% of the discharge records, followed by ED Registration Date on 51% of the discharges, ED Flag Code 2 on 40%, and primary or secondary admission source 16% (See Figure 1 below). Therefore, the two most reliable indicators appear to be 450 revenue code and ED registration data. The use of admission source 7 (outside hospital emergency room transfer) depends on your study. Some studies distinguish how they analyze interfacility transfers where there may a different type of delay in reaching definitive care from within hospital admissions. Figure 1. FY2018 Comparison Hospital Inpatient Discharge Indicators for Admitted through ED 100% 80% 332,072 399,162 483,071 60% 679,325 40% 477,198 410,108 20% 326,199 129,945 0% Revenue Code 450 ED Registration Date ED FLAG Code 2 Admission Source Codes 'R' Admitted through ED non-ED
Question Question: Similarly, if we wanted to analyze patients who are admitted through : Similarly, if we wanted to analyze patients who are admitted through observation observation s stay to inpatient tay to inpatient h hospitalization, what field should we use to ensure that we ospitalization, what field should we use to ensure that we have filtered for all such patients? have filtered for all such patients? Answer: Hospitals report observation room charges under revenue code 762. However, if the patient has been seen in Observation as well as another outpatient department and is then admitted, hospitals use Revenue Code 762 and use the alternate outpatient department as the admission source. Since this is frequently the case with observation stay patients, you will find a small number of discharges with source code X for observation admission source (see Figure 2 below) and a larger number with Revenue Code 762 and Observation Stay Flag indicating Yes . It is important to note that the revenue code units of service are reported in hours and a patient might have a longer observation stay, say 48 hours, than inpatient length of say, which could be only 1 day. Figure 2. FY2018 Comparison Hospital Inpatient Discharge Indicators for Admitted through Observation Stay 809,236 751,370 699,134 1,000,000 500,000 34 57,900 - 110,136 Either Admission Source Code 'X' Revenue Code 762 Observation Stay Flag 'Y' Admitted through Observation Stay non-Observation Stay
: Is Is case mix data on case mix data on inpatient hospitalizations inpatient hospitalizations (and (and ED ED use) use) Question Question: dated in such dated in such a a way that you can assess the busyness of a hospital or way that you can assess the busyness of a hospital or ED at a specific time period? ED at a specific time period?? ? ED Surge Volume Answer: The emergency department registration times are not released as part of the limited data set to non-government researchers. However, in both the ED Visit data and now as part of the hospital inpatient discharge data, the ED registration date can be requested by non-government applicants. The ED Visit data does however include a length of stay in hours and this field can be requested by non-government applicants. The length of stay in hours, date and patient visit volume does enable simulating seasonal surge models and looking at the relationship between patient volume and days on which specific patient volumes begin to hit the 24-hour ceiling. For example, while Figure 1 below shows FY2018 outpatient ED visit volume by length of stay in hours, the same annual comparison can be made by quarters, months, weeks, or days. Figure 1. FY2018 Outpatient ED Visit Volume Length of Stay in Hours 1000000 100000 PATIENT VOLUME 10000 1000 100 10 1 32 12 16 20 24 28 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 108 100 104 112 116 120 124 128 132 136 140 144 0 4 8 ED LENGTH OF STAY IN HOURS
: The ED data contains Visit Sequence The ED data contains Visit Sequence variable and a variable and a Sequence only see Sequence variables Sequence variables Visit Sequence only in the Sequence Question Question: variable. variable. Can you explain the difference? Can you explain the difference? I I only see in in the ED procedure and diagnosis tables, but the ED procedure and diagnosis tables, but Visit Sequence only in the main ED Visit. main ED Visit. Answer: For patients who had multiple ED visits within a year, the Visit Sequence variable in the main ED visit table indicates the sequence of the patient s visit based on the date when their specific UHIN appeared first within that year s release. As you can see in Figure 1 below, the majority of patients just have only one visit. The term sequence in the diagnosis and procedure codes field is simply how hospitals order each subsequent associated codes after the first diagnosis and first procedure. FIG 1. FY2019 ED VISIT SEQUENCE 10000000 1000000 NUMBER OF PATIENTS 100000 10000 1000 100 10 1 18 27 36 45 54 63 72 81 90 99 108 173 1 9 117 125 133 144 152 161 171 184 194 VISIT SEQUENCE
: We We found the principal diagnosis codes is sometimes listed in both the main table found the principal diagnosis codes is sometimes listed in both the main table Question Question: and the separate diagnosis table for inpatient and ED data, but in many times on the ED side and the separate diagnosis table for inpatient and ED data, but in many times on the ED side it is not listed in both places it is not listed in both places do you know why this is the case? do you know why this is the case? Answer: Hospitals report an admitting diagnosis, principal diagnosis, and discharge diagnosis which CMS defines as follow: Admitting Diagnosis - patient's initial diagnosis at the time of admission Principal Diagnosis the diagnosis chiefly responsible for the medical services provided Discharge Diagnosis patient s final diagnosis at the time of discharge Admitting Diagnosis Principal Diagnosis Discharge Diagnosis There are instances when the admitting diagnosis rendered before any diagnostic tests have been run, is the same at the principal diagnosis and discharge diagnosis. The admitting diagnosis and discharge diagnosis are used to generate separate DRGs. You do typically see this duplication in ED data because the ED setting is outpatient care where the patient receives care without being admitted. DRGs are not run on ED Data.
Question Question: Can you : Can you discuss the Hispanic Indicator Hispanic Indicator and the them in the data? them in the data? discuss the Race, Ethnicity, Race, Ethnicity, and the differences differences between between Answer: Race is a system of labelling that provides a source of identity and has the following five categories provided by the CDC: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, and White. Ethnicity is a term that describes shared culture, including practices, values, and beliefs of a group. Collection of ethnicity data depends on the questions asked and the format of the questions, which in turn, depends on the system s field capacity. CHIA adheres to the OMB guidance, using a two-question format, which includes the Hispanic ethnicity question, and then, granular ethnicity. Hence, the Case Mix data has the Hispanic Indicator flag variable that determines whether or not a patient is Hispanic or Latino regardless of race, the majority of patients just have only one visit. The term sequence in the diagnosis and procedure codes field is simply how hospitals order each subsequent associated codes after the first diagnosis and first procedure.
Where can I find past User Workgroup Presentations? http://www.chiamass.gov/ma-apcd-and-case-mix-user-workgroup- information/ 17 User Workgroup | CHIA User Support
When is the next User Group meeting? The next User Group will meet Tuesday, January 26. http://www.chiamass.gov/ma-apcd-and-case-mix-user-workgroup- information/
Questions? Questions related to MA APCD: apcd.data@state.ma.us Questions related to Case Mix: casemix.data@state.ma.us REMINDER: Please include your IRBNet ID#, if you currently have a project using CHIA data. 19 User Workgroup | CHIA User Support
Call for Topics and Presenters If there is a TOPIC that you would like to see discussed at an MA APCD or Case Mix workgroup in 2021, contact Amy Wyeth [amy.wyeth@state.ma.us] If you are interested in PRESENTING at a MA APCD or Case Mix workgroup in 2021, contact Amy Wyeth [amy.wyeth@state.ma.us] You can present remotely, or in-person at CHIA We may be reaching out to some data users with invitations to present, and hope you will consider this! 20 User Workgroup | CHIA User Support