Biomarker-Guided Antibiotic Duration in Sepsis Patients




Main Contacts
•
Chief Investigator:
Paul Dark
•
Warwick Clinical Trials Unit:
• Scott Regan (Senior Project Manager)
• Nicola McGowan (Trial Manager)
• Johnny Guck, Maddy Flawn & Uzma Manazar (Trial Coordinators)
•
Salford Royal – NHS Contractor
•
Sponsor:
University of Manchester
•
Funder:
NIHR
Contact
adaptsepsistrial@warwick.ac.uk
with any queries
Background
•
BRIEF:
NIHR Health Technology Assessment Programme commissioned
call
•
Shorter courses of antibiotics associated with – reductions in AEs, reductions in healthcare
resource utilisation, wider downstream benefits for antimicrobial resistance
•
Does a treatment protocol based on serial monitoring of CRP or PCT safely allow reduction in
duration of antibiotic therapy in hospitalised patients with sepsis?
Summary
•
Design:
Multi-centre 3-arm randomised controlled trial with internal
pilot
•
Population:
Hospitalised adults who have been commenced on
intravenous antibiotics for sepsis
•
Intervention:
CRP or PCT-guided antibiotic duration
•
Outcome:
Reduction in number of days patients receive antibiotics
•
Sample size:
2760 over 30 months
Patient Group – Eligibility
Inclusion criteria
•
Hospitalised adult patients at least 18 years of age
•
Up to 24 hours of initiation of empiric intravenous antibiotic treatments for a
suspicion of sepsis
Sepsis:
‘acute organ dysfunction associated with suspected infection’
•
Likely to remain hospitalised and receiving intravenous antibiotic treatment for
at least the next 72 hours
•
Requirement for Critical Care
Patient Group – Eligibility
Main exclusion criteria
•
More than 24 hours since receiving first empiric intravenous antibiotic treatments for a suspicion of sepsis
•
Prolonged (greater than 21 days) antimicrobial therapy mandated (e.g. for tuberculosis, osteomyelitis)
•
Severely immunocompromised (e.g. neutropenia, less than 500 neutrophils/microliter)
•
All treatment for suspected sepsis likely to be stopped within 24 hours of its initiation because of futility
•
Consent declined
•
Previously enrolled in the trial
Patient Group – Eligibility
Recruitment
Stratification factors:
-
Site
-
Sepsis severity
-
Surgery within last 72 hours
Recruitment
Consent procedures
•
Patient consent and lack of objection by Personal or Trust Nominated Consultee will be
monitored throughout antibiotic treatment
•
If a patient regains capacity by time of hospital discharge or by 28 days post-
randomisation, retrospective Patient Information will be given and consent sought
Recruitment plan
•
Target for sites – 1 patient per week
Web based randomisation
Web based randomisation
Web based randomisation
•
Group allocation will be concealed from the participant and
their friends/relatives, the treating clinical teams, local
research staff and main trial team
•
Laboratory staff will have access to the allocation relating to
a sample number but will not be able to identify the patient
Emergency randomisation procedure
•
In the event of system outage affecting the web-based system, the
emergency randomisation procedure will be followed, this can be found
in ISF
•
A telephone randomisation service will be operational 9am – 5pm,
Monday to Friday
•
The research team will be allocated a trial number for a participant
Note – telephone randomisation will only be available if the
randomisation section of the database is unavailable. If the whole
database is not available randomisation will be halted, the trials unit
will email to confirm when this is back up and running.
Baseline – Day 1
•
The baseline period is defined as
the period from time of first
antibiotic treatment to 24 hours.
•
Moving forward data will be
captured on calendar days.
•
Daily data commences from the
calendar day following diagnosis,
meaning there may be overlap
between Baseline and Day 1
•
Documenting antibiotic treatment
Baseline variables
•
Baseline characteristics data:
–
Patient identifier, NHS number, age and gender
–
Inclusion and exclusion criteria
–
Sepsis severity
–
Admission diagnosis
–
First 24-hour sepsis care bundle treatments and interventions,
including antibiotics
–
qSOFA, SOFA and APACHE II scores
–
Cause and site of infection including diagnostic evidence
•
Causative microorganism identified for the infection causing sepsis and the
sample that each pathogen was detected in.
Intervention
Intervention – Research team
Intervention – Research team
Intervention – Research team
Intervention – Research team
Intervention - Lab
•
Trial database will act as an intermediary between lab and clinical teams
•
Lab required input is as minimal as possible – biomarker result and time of test will be
recorded
•
Lab Lead to be listed on delegation log and has the responsibility to nominate other
members of the team working with the trial database and ensuring appropriate training
•
Adequate weekend cover required to ensure samples can be processed over the weekend
Intervention - Lab
Intervention - Lab
Intervention - Lab
Intervention - Lab
Intervention - Lab
Intervention - Lab
Intervention
Intervention
•
If you think you have been unblinded please contact the trial team as soon as possible and do not discuss with
the rest of your team.
Advice
•
Standardised written advice will be automatically generated and delivered daily to local research
team
•
Advice will be sent daily via email and available on the trial database
•
Advice will be based on daily serum testing of either PCT or CRP or ‘no test’ (control group).
•
Trial assay results will
not
be returned to routine clinical practice
•
If advice not received by expected time then chase lab for samples – important that daily
sampling and advice is in place.
•
When antibiotics for initial sepsis episode are stopped, the entire intervention process will cease
and the participant will enter the follow-up phase until Day 28
Equipoise
•
Any non-trial use of PCT during the intervention phase has the potential to influence
antibiotic duration. Maintaining equipoise for the purposes of this trial involves avoiding
PCT use up to 28-days post randomisation, as this could impact on the primary outcome
(duration of antibiotics to 28 days).
•
Any non-trial use of PCT will be recorded as a protocol deviation and will be monitored
at each site by the research team.
CRP
PCT
Emergency sample processing system
•
In the event that the online system is unavailable, attempts should be made to retry the
system at a later time
•
If the system is still inaccessible the emergency procedure will be followed: the clinical
team will follow the usual care advice and the lab team will discard the blood sample
•
Note: if the database is down randomisation will be temporarily suspended
•
Once the system is restored, daily sample processing can proceed as normal
•
Protocol deviation forms should be completed to capture any participants affected by a
system failure
Emergency sample processing system
– Labs
•
Await phone call from treating clinical team before
attempting to retry the database.
•
All samples that are not able to be analysed within 24 hours
should be destroyed as per local policy
Daily data
•
Daily data is collected from the first calendar day following
diagnosis until the participant stops receiving systemic
antibiotics for initial suspected sepsis episode
•
The participant then progresses from intervention to follow-
up phase.
•
If the patient remains an inpatient, follow up data will be
collected on a daily basis until hospital discharge or 28 days
•
If patient is discharged a 28 day follow up form will be
completed from date of hospital discharge to 28 days.
Daily data
•
Daily Data Collection:
–
Survival status
–
The length of hospital stay
–
The length of critical care admission
–
Time ‘fit’ for hospital discharge
–
Day 3 and 7 SOFA scores
–
Protocol adherence
–
Suspected antibiotic adverse reactions
–
Name and dose of antibiotics (expressed as Defined Daily Dose)
–
Duration of antibiotic use (days in 24 hour periods from randomisation)
–
Re-lapse, recurrence and super-infection/new infection rates
–
Unscheduled re-admission or care escalation
Data Management
•
Daily Data Collection:
–
Daily data should be entered as soon as possible
–
All other data should be entered within 4 weeks of the expected
completion date
•
Queries will be sent out to sites on a monthly basis to
request missing data and for any data clarifications.
Follow-up
Follow-up
•
Daily Follow-up Data Collection:
–
Survival status
–
The length of hospital stay
–
The length of critical care admission
–
Time ‘fit’ for hospital discharge
–
Day 3 and 7 SOFA scores
–
Suspected antibiotic adverse reactions
–
Name and dose of antibiotics (expressed as Defined Daily Dose)
–
Duration of antibiotic use (days in 24 hour periods from randomisation)
–
Re-lapse, recurrence and super-infection/new infection rates
–
Unscheduled re-admission or care escalation
Follow-up
•
28 Day Follow-up Data Collection:
–
Survival status
–
Suspected antibiotic adverse reactions
–
Name and dose of antibiotics (expressed as Defined Daily Dose)
–
Duration of antibiotic use (days in 24 hour periods from
randomisation)
–
Re-lapse, recurrence and super-infection/new infection rates
–
Unscheduled re-admission or care escalation
Follow up – 90 days
•
WCTU will collect all-cause mortality via data linkage
•
No input required from site teams
Clinically Relevant
Antibiotic Related Events
•
Defined as:
–
Anaphylaxis
–
Gastrointestinal
–
Haematological
–
Hepatobiliary
–
Renal
–
Neurological
–
Dermatological
–
Cardiac
–
Muscular
–
C.diff diarrhoeal infection
–
Multi-drug resistant organism
–
Other
Collecting as part of
daily data, daily data
follow-up and 28 day
follow-up
SAE Reporting
•
SAE’s must be reported to WCTU as soon as possible - within
24 hours of becoming aware
•
SAE’s should always be completed on paper CRFs and faxed
through to the safe haven fax machine or emailed, if
anonymised, to the WCTU QA team
(
wctuqa@warwick.ac.uk
)
•
SAE’s will be reported from the time of randomisation until
28 Days post-randomisation
SAE Reporting
•
Death is captured as a trial outcome. Only deaths where the site
investigator believes there may be an association between the death
and participation in the trial require reporting as an SAE.
•
The following SAEs are exempt from reporting:
–
Death related to sepsis
–
Cardiovascular failure, including the need for vasopressors / inotropes
–
Respiratory failure, including mechanical ventilation and acute lung injury
–
Hepatic failure
–
Renal failure, including the need for renal replacement therapy
–
Haematological / coagulation failure, including thrombocytopaenia
–
Neurological failure
Patient Group - Withdrawal
•
Participant or their consultee free to withdraw participant at
any time without giving a reason, but collect one if possible
•
Other reasons that a participant may be withdrawn include
clinical team decision, antibiotics stopped due to futility and
participant requiring long term antibiotics (≥21 days).
•
Data collected up until that point will automatically be used
unless participant specifically requests otherwise
•
Unless a participant explicitly withdraws their consent, they
will be followed-up wherever possible and data collected as
per the protocol until the end of the trial.
Co-enrolment
•
As with many trials in the critical care setting we will be co-
enrolling. Current co-enrolling trials include:
–
The 65 Trial
–
REST
–
STRESS-L
–
BLING III PQIP
–
A-Stop
–
A2B
–
PQIP
•
Please phone WCTU 02476 151 386 or email
adaptsepsistrial@warwick.ac.uk
with any queries
PI Responsibilities
•
Compliance with protocol (& SOPs), GCP and regulatory requirements
•
Maintain a list of staff & delegated duties
•
Provide Pre-Trial Documents
•
All trial related medical decisions
•
Obtaining Informed Consent
•
Maintain subject confidentiality
•
Keep source documents
•
Hospital records, prescriptions, CRF worksheets, details of any verbal consultations/actions
•
Maintain Site File
•
Adverse Event Reporting
•
Protocol Deviations
•
Permit monitoring, audit & inspection
•
Archiving
Study oversight
•
Each site will be provided with a:
–
Investigator Site File (ISF)
–
Lab Site File (LSF)
•
It will be the sites responsibility to maintain the site files
•
The ISF contains all trial records kept at the site:
–
Protocol, paper CRF worksheets
–
REC approved study documents
–
Main HRA/REC Approvals and Trust confirmation of C&C MHRA approval
–
Delegation of Responsibility Log
–
Signed ICFs
–
Screening / Enrolment logs
–
Adverse Event Reporting
–
Investigator CVs
–
Investigator Meeting & Initiation Visit Reports
–
Trial Report
–
Monitoring Records
Monitoring
•
Sites will be monitored by WCTU within 2 months of
recruiting their first patient.
•
The lab will also be monitored as part of this visit
•
Risk proportionate monitoring will be undertaken and this
may include a second visit during the main stage of the trial.
•
Additional visits may be triggered, for example in response
to SAE reporting
Monitoring continued
•
Main site visit
–
Informed consent procedure
–
Informed Consent Form review
–
Eligibility
–
Source data verification – prescriptions, readmissions, SAEs and
evidence of unblinding
–
Investigator Site File
•
Lab visit
–
Transcription errors – sample request form
–
Lab Site File
Training
•
CVs and GCP certificates for PI
•
New staff – WCTU will provide up-to-date SIV slides, contact
adaptsepsistrial@warwick.ac.uk
with any queries
•
Further training may be available following substantial
amendments or at the request of site
•
Lab team (including all new starters) must read and
acknowledge (by signing and dating) the lab manual –
documentation in Lab Site File
Thank you…any questions?
This research focuses on evaluating the safety and efficacy of a biomarker-guided approach to determine the duration of antibiotic treatment in hospitalized adult patients with sepsis. The study involves a multi-centre randomized controlled trial to assess if a treatment protocol based on monitoring CRP or PCT levels can lead to a reduction in the number of days patients receive antibiotics. The trial aims to enroll 2760 patients over 30 months, targeting reductions in adverse events, healthcare resource utilization, and potential benefits for antimicrobial resistance.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
BiomArker-guided Duration of Antibiotic treatment in hospitalised PaTients with Sepsis
Main Contacts Chief Investigator: Paul Dark Warwick Clinical Trials Unit: Scott Regan (Senior Project Manager) Nicola McGowan (Trial Manager) Johnny Guck, Maddy Flawn & Uzma Manazar (Trial Coordinators) Salford Royal NHS Contractor Sponsor: University of Manchester Funder: NIHR Contact adaptsepsistrial@warwick.ac.uk with any queries
Background BRIEF: NIHR Health Technology Assessment Programme commissioned call Shorter courses of antibiotics associated with reductions in AEs, reductions in healthcare resource utilisation, wider downstream benefits for antimicrobial resistance Does a treatment protocol based on serial monitoring of CRP or PCT safely allow reduction in duration of antibiotic therapy in hospitalised patients with sepsis?
Summary Design: Multi-centre 3-arm randomised controlled trial with internal pilot Population: Hospitalised adults who have been commenced on intravenous antibiotics for sepsis Intervention: CRP or PCT-guided antibiotic duration Outcome: Reduction in number of days patients receive antibiotics Sample size: 2760 over 30 months
Patient Group Eligibility Inclusion criteria Hospitalised adult patients at least 18 years of age Up to 24 hours of initiation of empiric intravenous antibiotic treatments for a suspicion of sepsis Sepsis: acute organ dysfunction associated with suspected infection Likely to remain hospitalised and receiving intravenous antibiotic treatment for at least the next 72 hours Requirement for Critical Care
Patient Group Eligibility Main exclusion criteria More than 24 hours since receiving first empiric intravenous antibiotic treatments for a suspicion of sepsis Prolonged (greater than 21 days) antimicrobial therapy mandated (e.g. for tuberculosis, osteomyelitis) Severely immunocompromised (e.g. neutropenia, less than 500 neutrophils/microliter) All treatment for suspected sepsis likely to be stopped within 24 hours of its initiation because of futility Consent declined Previously enrolled in the trial
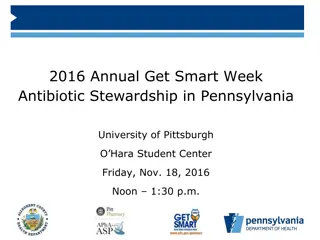
Recruitment Stratification factors: - Site - Sepsis severity - Surgery within last 72 hours Assessed for Eligibility Hospitalised patients on IV antibiotics for sepsis ENROLMENT Randomised (No of patients = 2760) Allocated to Standard Care Allocated to PCT-guided antibiotic discontinuation protocol No of patient = 920 Hospitalised patients on IV antibiotics for sepsis Allocated to CRP-guided antibiotic discontinuation protocol No of patient = 920 Hospitalised patients on IV antibiotics for sepsis ALLOCATION No of patient = 920 Hospitalised patients on IV antibiotics for sepsis
Recruitment Receive standard care for sepsis and antibiotic stewardship and serum laboratory measured CRP Receive standard care for sepsis and antibiotic stewardship Receive standard care for sepsis and antibiotic stewardship and serum laboratory measured PCT FOLLOW UP -28 days follow up and outcome measurements -90 day follow up all cause mortality -28 days follow up and outcome measurements -90 day follow up all cause mortality -28 days follow up and outcome measurements -90 day follow up all cause mortality Primary Outcomes: Analysed Duration of antibiotics during 28 days and safety outcome Primary Outcomes: Analysed Duration of antibiotics during 28 days and safety outcome Primary Outcomes: Analysed Duration of antibiotics during 28 days and safety outcome ANALYSIS
Consent procedures Patient gives informed consent Patient has capacity (Patient Information Sheet and Consent form) Patient approached as soon as they have been identified to critical care for admission Seek advice from personal consultee (Consultee Information Sheet and Declaration form) Patient lacks capacity If attempts to meet a Personal Consultee fail, a professional unconnected to the conduct of the trial may act as a Trust Nominated Consultee (Consultee Information Sheet and Declaration form) Patient consent and lack of objection by Personal or Trust Nominated Consultee will be monitored throughout antibiotic treatment If a patient regains capacity by time of hospital discharge or by 28 days post- randomisation, retrospective Patient Information will be given and consent sought
Recruitment plan Target for sites 1 patient per week ADAPT-Sepsis Recruitment 3000 2000 NUMBER OF PATIENTS 1000 0
Web based randomisation Group allocation will be concealed from the participant and their friends/relatives, the treating clinical teams, local research staff and main trial team Laboratory staff will have access to the allocation relating to a sample number but will not be able to identify the patient
Emergency randomisation procedure In the event of system outage affecting the web-based system, the emergency randomisation procedure will be followed, this can be found in ISF A telephone randomisation service will be operational 9am 5pm, Monday to Friday The research team will be allocated a trial number for a participant Note telephone randomisation will only be available if the randomisation section of the database is unavailable. If the whole database is not available randomisation will be halted, the trials unit will email to confirm when this is back up and running.
Baseline Day 1 The baseline period is defined as the period from time of first antibiotic treatment to 24 hours. Moving forward data will be captured on calendar days. Daily data commences from the calendar day following diagnosis, meaning there may be overlap between Baseline and Day 1 Documenting antibiotic treatment
Baseline variables Baseline characteristics data: Patient identifier, NHS number, age and gender Inclusion and exclusion criteria Sepsis severity Admission diagnosis First 24-hour sepsis care bundle treatments and interventions, including antibiotics qSOFA, SOFA and APACHE II scores Cause and site of infection including diagnostic evidence Causative microorganism identified for the infection causing sepsis and the sample that each pathogen was detected in.
Intervention Research team Take research sample and log into trial database Complete sample request card with sample number Take sample to lab team and indicate via database Database status will update to advice pending
Intervention Research team Take research sample and log into trial database Complete sample request card with sample number Take sample to lab team and indicate via database Database status will update to advice pending
Intervention Research team Take research sample and log into trial database Complete sample request card with sample number Take sample to lab team and indicate via database Database status will update to advice pending
Intervention Research team Take research sample and log into trial database Complete sample request card with sample number Take sample to lab team and indicate via database Database status will update to advice pending
Intervention - Lab Trial database will act as an intermediary between lab and clinical teams Lab required input is as minimal as possible biomarker result and time of test will be recorded Lab Lead to be listed on delegation log and has the responsibility to nominate other members of the team working with the trial database and ensuring appropriate training Adequate weekend cover required to ensure samples can be processed over the weekend
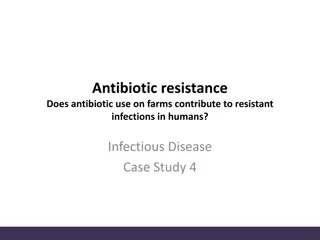
Intervention PCT protocol CRP protocol Standard care + daily serum PCT measurement until antibiotic discontinuation Standard care + daily serum CRP measurement until antibiotic discontinuation Advice for both PCT and CRP groups delivered daily to treating clinician Control group advice delivered daily to treating clinician Protocol STRONGLY supports stopping antibiotics Protocol supports usual care PCT < 0.25 g/l CRP < 25mg/l PCT fall by >80% from baseline or PCT > 0.25 & < 0.50 g/l CRP fall by 50% from baseline Protocol suggests stopping antibiotics Protocol supports usual care Protocol supports usual care PCT does not meet above criteria CRP does not meet above criteria Protocol supports usual care
Intervention If you think you have been unblinded please contact the trial team as soon as possible and do not discuss with the rest of your team.
Advice Standardised written advice will be automatically generated and delivered daily to local research team Advice will be sent daily via email and available on the trial database Advice will be based on daily serum testing of either PCT or CRP or no test (control group). Trial assay results will not be returned to routine clinical practice If advice not received by expected time then chase lab for samples important that daily sampling and advice is in place. When antibiotics for initial sepsis episode are stopped, the entire intervention process will cease and the participant will enter the follow-up phase until Day 28
Equipoise CRP PCT Any non-trial use of PCT during the intervention phase has the potential to influence antibiotic duration. Maintaining equipoise for the purposes of this trial involves avoiding PCT use up to 28-days post randomisation, as this could impact on the primary outcome (duration of antibiotics to 28 days). Any non-trial use of PCT will be recorded as a protocol deviation and will be monitored at each site by the research team.
Emergency sample processing system In the event that the online system is unavailable, attempts should be made to retry the system at a later time If the system is still inaccessible the emergency procedure will be followed: the clinical team will follow the usual care advice and the lab team will discard the blood sample Note: if the database is down randomisation will be temporarily suspended Once the system is restored, daily sample processing can proceed as normal Protocol deviation forms should be completed to capture any participants affected by a system failure
Emergency sample processing system Labs Await phone call from treating clinical team before attempting to retry the database. All samples that are not able to be analysed within 24 hours should be destroyed as per local policy
Daily data Daily data is collected from the first calendar day following diagnosis until the participant stops receiving systemic antibiotics for initial suspected sepsis episode The participant then progresses from intervention to follow- up phase. If the patient remains an inpatient, follow up data will be collected on a daily basis until hospital discharge or 28 days If patient is discharged a 28 day follow up form will be completed from date of hospital discharge to 28 days.
Daily data Daily Data Collection: Survival status The length of hospital stay The length of critical care admission Time fit for hospital discharge Day 3 and 7 SOFA scores Protocol adherence Suspected antibiotic adverse reactions Name and dose of antibiotics (expressed as Defined Daily Dose) Duration of antibiotic use (days in 24 hour periods from randomisation) Re-lapse, recurrence and super-infection/new infection rates Unscheduled re-admission or care escalation
Data Management Daily Data Collection: Daily data should be entered as soon as possible All other data should be entered within 4 weeks of the expected completion date Queries will be sent out to sites on a monthly basis to request missing data and for any data clarifications.
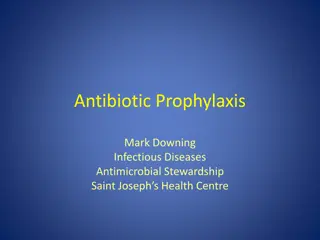
Follow-up Day 0 Day 28 Intervention Phase Follow-Up Phase 1. Antibiotics Daily Follow-up 2. Antibiotics Daily Follow-up 28 Day Follow-up Hospital Discharge 3. Antibiotics Daily Follow-up Readmission = Daily Follow-up Hospital Discharge
Follow-up Daily Follow-up Data Collection: Survival status The length of hospital stay The length of critical care admission Time fit for hospital discharge Day 3 and 7 SOFA scores Suspected antibiotic adverse reactions Name and dose of antibiotics (expressed as Defined Daily Dose) Duration of antibiotic use (days in 24 hour periods from randomisation) Re-lapse, recurrence and super-infection/new infection rates Unscheduled re-admission or care escalation
Follow-up 28 Day Follow-up Data Collection: Survival status Suspected antibiotic adverse reactions Name and dose of antibiotics (expressed as Defined Daily Dose) Duration of antibiotic use (days in 24 hour periods from randomisation) Re-lapse, recurrence and super-infection/new infection rates Unscheduled re-admission or care escalation
Follow up 90 days WCTU will collect all-cause mortality via data linkage No input required from site teams
Clinically Relevant Antibiotic Related Events Defined as: Anaphylaxis Gastrointestinal Haematological Hepatobiliary Renal Neurological Dermatological Cardiac Muscular C.diff diarrhoeal infection Multi-drug resistant organism Other Collecting as part of daily data, daily data follow-up and 28 day follow-up
SAE Reporting SAE s must be reported to WCTU as soon as possible - within 24 hours of becoming aware SAE s should always be completed on paper CRFs and faxed through to the safe haven fax machine or emailed, if anonymised, to the WCTU QA team (wctuqa@warwick.ac.uk) SAE s will be reported from the time of randomisation until 28 Days post-randomisation
SAE Reporting Death is captured as a trial outcome. Only deaths where the site investigator believes there may be an association between the death and participation in the trial require reporting as an SAE. The following SAEs are exempt from reporting: Death related to sepsis Cardiovascular failure, including the need for vasopressors / inotropes Respiratory failure, including mechanical ventilation and acute lung injury Hepatic failure Renal failure, including the need for renal replacement therapy Haematological / coagulation failure, including thrombocytopaenia Neurological failure
Patient Group - Withdrawal Participant or their consultee free to withdraw participant at any time without giving a reason, but collect one if possible Other reasons that a participant may be withdrawn include clinical team decision, antibiotics stopped due to futility and participant requiring long term antibiotics ( 21 days). Data collected up until that point will automatically be used unless participant specifically requests otherwise Unless a participant explicitly withdraws their consent, they will be followed-up wherever possible and data collected as per the protocol until the end of the trial.
Co-enrolment As with many trials in the critical care setting we will be co- enrolling. Current co-enrolling trials include: The 65 Trial REST STRESS-L BLING III PQIP A-Stop A2B PQIP Please phone WCTU 02476 151 386 or email adaptsepsistrial@warwick.ac.uk with any queries
PI Responsibilities Compliance with protocol (& SOPs), GCP and regulatory requirements Maintain a list of staff & delegated duties Provide Pre-Trial Documents All trial related medical decisions Obtaining Informed Consent Maintain subject confidentiality Keep source documents Hospital records, prescriptions, CRF worksheets, details of any verbal consultations/actions Maintain Site File Adverse Event Reporting Protocol Deviations Permit monitoring, audit & inspection Archiving
Study oversight Each site will be provided with a: Investigator Site File (ISF) Lab Site File (LSF) It will be the sites responsibility to maintain the site files The ISF contains all trial records kept at the site: Protocol, paper CRF worksheets REC approved study documents Main HRA/REC Approvals and Trust confirmation of C&C MHRA approval Delegation of Responsibility Log Signed ICFs Screening / Enrolment logs Adverse Event Reporting Investigator CVs Investigator Meeting & Initiation Visit Reports Trial Report Monitoring Records
Monitoring Sites will be monitored by WCTU within 2 months of recruiting their first patient. The lab will also be monitored as part of this visit Risk proportionate monitoring will be undertaken and this may include a second visit during the main stage of the trial. Additional visits may be triggered, for example in response to SAE reporting