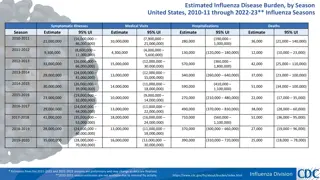
Epidemiology Update on Influenza Surveillance and Activity in Virginia
Providing insights into the influenza season in Virginia, this update highlights the importance of conducting surveillance, data sources for monitoring influenza-like illness, and comparisons of influenza activity levels over multiple seasons. By tracking influenza viruses and their impact, the goal is to establish a useful surveillance system at both local and national levels.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Epidemiology Update HEALTH AND HUMAN RESOURCES SUB-PANEL, GOVERNOR S SECURE COMMONWEALTH INITIATIVE October 16, 2017
Epidemiology Updates Influenza/Respiratory Conditions Opioid Indicators Viral Hepatitis
Influenza Influenza season is typically defined as early October to mid-May (MMWR weeks 40 to 20) 2017-2018: reporting starts October 1, 2017 Influenza activity usually peaks in January or February in Virginia Virginia conducts surveillance year-round Weekly activity level relies on three data sources: Influenza-like illness (ILI) visits to healthcare providers Viral laboratory specimens (DFA, PCR, and/or culture) Outbreaks 3
Why Conduct Influenza Surveillance? Determine which, when, and where influenza viruses are circulating Determine intensity and impact of influenza activity Detect unusual events Infection by unusual viruses Unusual syndromes caused by influenza viruses Unusually large/severe outbreaks Goal: build a system that is useful on the local level and builds up to national level surveillance 4
Data Sources Influenza-like illness (ILI) data Electronic data feeds from hospital emergency departments (ED) and urgent care (UC) facilities 157 facilities reporting data daily Uses chief complaint (free text) ILI case definition: Fever with cough and/or sore throat Laboratory reports Lab specimens collected through sentinel sites and other providers Confirmatory labs (e.g., PCR, DFA, culture) Summary counts of rapid tests Results of laboratory specimens are entered into VEDSS Electronic laboratory reports (ELRs) into VEDSS 5
Percent of Visits for Influenza-like Illness by Week, Virginia, Comparison of Five Influenza Seasons 12 10 8 Percent ILI 6 4 2 0 40 42 44 46 48 50 52 2 4 6 8 10 12 14 16 18 20 Week 2012-2013 2013-2014 2014-2015 2015-2016 2016-2017
Comparison of Weekly Influenza Activity Levels in Virginia for the 2015- 2016 and 2016-2017 Influenza Seasons 4 3 Activity Level 2 2015-2016 2016-2017 1 0 40 42 44 46 48 50 52 2 4 6 8 10 12 14 16 18 20 Week Data are presented by week, with the first Sunday to Saturday week in January as week 1 Activity Levels: 0=No Activity 1=Sporadic 2=Local 3=Regional 4=Widespread 7
Positive Laboratory Reports and ILI Visits by Week, Virginia, 2016-2017 Influenza Season 225 7 200 Number of Positive Laboratory Reports 6 175 Percent of Visits due to ILI 5 150 4 125 100 3 75 2 50 1 25 0 0 40 42 44 46 48 50 52 2 4 6 8 10 12 14 16 18 20 Week A(H3) A(H1) B A(Subtyping Not Performed) A (2009 H1N1) ILI 8
Positive Specimens by Type; A Comparison of VA and US: 2016-2017 Influenza Season Subtype Virginia US 80% 78% Influenza A 69% 97% H3N2 2% 3% 2009 H1N1 1% -- H1 28% -- Subtyping Not Performed 20% 22% Influenza B 9
Flu Near You Participatory disease surveillance system for ILI symptoms Users report their health information using a brief weekly survey Also features a Vaccine Finder tool Generate early signal of ILI Provide insights to the public and stakeholders www.flunearyou.org
Posted on VDH flu surveillance website: http://www.vdh.virginia.gov/epidemiology/influenza-flu-in-virginia/influenza-surveillance/
Novel Influenza Viruses & Terminology Novel influenza A virus infection: Human infection with any influenza A virus different from current seasonal influenza A viruses Variant influenza virus: Human infection with a swine-origin influenza virus Abbreviated with a lower case v following subtype (e.g., H3N2v, H1N1v, H1N2v) Avian influenza virus: Human infection with an avian-origin influenza A virus Only swine-origin and avian-origin influenza A viruses have been identified in humans globally Canine, equine, and other non-human animal influenza viruses have not been identified in humans 12
Avian Influenza Avian influenza (AI) is a disease of birds caused by influenza type A viruses that can infect poultry and can be found in waterfowl Designated as highly pathogenic (HPAI) or low pathogenic avian influenza (LPAI) due to ability to cause disease in chickens Although these viruses usually do not infect humans, rare cases of human infection have been reported Human infections with HPAI or LPAI viruses have resulted in a wide range of illness, from mild to fatal VDH Avian Influenza Response Plan 13
Avian Influenza (H5N2) Update Avian influenza (H5N2) detected in wild mallard duck in Montana in January 2017 Part of on-going, routine surveillance for avian influenza viruses No human infections or mortality among domestic poultry associated with this finding This strain is similar to the H5N2 strain associated with the multistate outbreak of HPAI in the U.S. in 2014-15 This was the first state to report HPAI in 2017 The risk to the public from these H5 HPAI infections is low; no human infections have occurred in the U.S.
Avian Influenza (H7N9) Update March 5, 2017 USDA/APHIS reported detection of highly pathogenic avian influenza (HPAI) A virus in commercial chicken flock in Lincoln County, Tennessee Identified as H7N9, but not the same as the China H7N9 virus Low-pathogenic H7N9 found on second Tennessee farm and other southeastern states (AL, GA, KY) No human illnesses in US; no avian cases in VA Possible exposures can occur during depopulation, disposal, decontamination activities Medical monitoring for 10 days post-exposure Antivirals may be used VDH subject matter expert: Dr. Karen Gruszynski http://www.cdc.gov/flu/avianflu/guidance-exposed-persons.htm 15
H3N2v Update On May 5, 2017, CDC reported a human infection with a novel influenza virus Occurred in child in Texas who was not hospitalized; recovered Exposure to swine was reported at an agricultural event in week preceding illness onset September 2017: H3N2v detected in Maryland residents who reported close contacts with pigs at agricultural fairs As of October 4, 2017 : 40 presumptive positive and confirmed cases in this Maryland cluster Since August 2011: 365 cases identified in U.S. 3 cases in 2015 (MI, MN, NJ) 18 cases in 2016 (MI, OH) 1 case in 2017 (TX) 1 case with VA exposure in 2013 Associated with exposure to swine at agricultural fairs Case Counts: http://www.cdc.gov/flu/swineflu/variant-cases-us.htm
Take home message Influenza surveillance Importance of provider awareness and prompt reporting Adherence to prevention strategies Vaccination! Stay home when you re sick Wash your hands Adherence to infection control
MERS-CoV Camel Flu 18
Middle East Respiratory Syndrome (MERS-CoV) Viral respiratory illness First reported in Saudi Arabia in 2012 Linked to countries in and near the Arabian Peninsula Caused by a coronavirus Severe acute respiratory illness Fever, cough, sore throat, chest pain, and shortness of breath Approximately 30-40% of patients with confirmed MERS-CoV infection have died Two imported cases identified in U.S. Travel history to Saudi Arabia Two cases not linked Indiana, Florida 19
MERS-CoV Testing Criteria Severe illness: Fever AND pneumonia or acute respiratory distress syndrome (based on clinical or radiological evidence) with history of any of the following exposures Travel to Arabian Peninsula within 14 days of symptom onset or close contact with symptomatic traveler History of being in a healthcare facility in the Republic of Korea within 14 days of symptom onset Member of a cluster of patients with severe acute respiratory illness (e.g. fever and pneumonia requiring hospitalization) of unknown etiology in which MERS-CoV is being evaluated Mild illness: Fever AND symptoms of respiratory illness with history of being in a healthcare facility in the Arabian Peninsula within 14 days Fever OR symptoms of respiratory illness with history of close contact with a MERS case 20
Opioid Indicators and Viral Hepatitis
Opioid Indicators Dashboard 2017 Governor s Technology Award Initially created in response to the Comprehensive Harm Reduction Legislation A platform for the public and health professionals to find data related to the opioid epidemic Data included in the dashboard: HIV, HCV, Neonatal Abstinence Syndrome (NAS), Overdose data, EMS Narcan administration and Emergency Department data. Trends by year and age group State, Region, District, and Locality level data Opioid Addiction Indicators Dashboard Link
Rates of Newly Reported Acute and Past or Present HCV, by County, Virginia, 2010 and 2016
Incidence of Chronic HBV and HCV Infections Virginia, 2010-2016
Percentage of Past or Present HCV Cases by Age Group, Virginia, 2010-2016
Percentage of Past or Present HCV Cases by Age Group, Virginia, 2010-2016 18-29 Years 18 16.9 16.4 16 15.89 15.5 14 13.5 12 Percentage 10.7 10 9.2 8.9 8 8.2 8 8 6 4 2 0 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Percentage of Past and Present HCV Cases, Persons 18-29 Years of Age, Appalachian* vs. non-Appalachian, 2010-2016 *based on event date *Alleghany, Bath, Bland, Botetourt, Buchanan, Carroll, Craig, Dickenson, Floyd, Giles, Grayson, Henry, Highland, Lee, Montgomery, Patrick, Pulaski, Rockbridge, Russell, Scott, Smyth, Tazewell, Washington, Wise, Wythe, Bristol city, Buena Vista city, Covington city, Galax city, Lexington city, Martinsville city, Norton city, Radford city)
HCV Cases* per 100,000 Persons Aged 18-29 by County (Appalachia** vs. Non- Appalachia), Virginia 2006-2015 Appalachia (rate per 100,000) Non-Appalachia (rate per 100,000) Univariate Rate Ratio (95% CI) Year 2006-2010 48.0 8.2 5.79 (5.04-6.65) 2011-2015 96.1 21.6 4.44 (4.04-4.87) 2006-2015 72.1 14.9 4.81 (4.45-5.20) *Excludes persons institutionalized at the time of diagnosis **Alleghany, Bath, Bland, Botetourt, Buchanan, Carroll, Craig, Dickenson, Floyd, Giles, Grayson, Henry, Highland, Lee, Montgomery, Patrick, Pulaski, Rockbridge, Russell, Scott, Smyth, Tazewell, Washington, Wise, Wythe, Bristol city, Buena Vista city, Covington city, Galax city, Lexington city, Martinsville city, Norton city, Radford city)
Acknowledgements Division of Surveillance and Investigation Sarah Fenno (former Influenza Surveillance Coordinator) Division of Disease Prevention VDH Addiction/Opioid Data Workgroup
Influenza A (H3N2) Variant Virus September 2017: H3N2v detected in Maryland residents who reported close contacts with pigs at agricultural fairs As of October 4, 2017 : 40 presumptive positive and confirmed cases
Sentinel Influenza Surveillance Participating providers are asked to send up to 5 specimens/week to DCLS for viral isolation. Provides data to: Help characterize the level of Influenza-like Illness (ILI) activity Track the strains of influenza virus circulating in the state Measure the impact of influenza on morbidity and mortality in our communities
Results of Sentinel Surveillance 61 sentinel surveillance sites recruited to collect viral specimens during the 2016-2017 season Represented 25 health districts Goal: up to 5 specimens per week from each sentinel site 14 sites did not submit any specimens during the season 745 sentinel specimens received 40
Asian H7N9 Bird Flu in China Human infections with avian influenza A(H7N9) viruses were first reported in China in March 2013 Annual increases in the number of human infections in China have occurred each winter since 2013 and are called epidemics Most reported poultry exposure; no sustained person-to-person transmission Cumulative number of human infections with Asian H7N9 viruses reported by WHO between 2013 and present: 1,486
H7N9 in China Update H7N9 Mainland China Smaller numbers in travelers from Hong Kong, Taiwan, Malaysia, Canada Most hospitalized Most reported poultry contact No sustained person-to-person transmission No cases detected in U.S. 43
H7N9 Testing Criteria New onset of severe acute respiratory infection requiring hospitalization Recent travel (within <10 days of illness onset) to areas where human cases of avian influenza A (H7N9) are present or to areas where avian influenza A (H7N9) viruses are known to be circulating in animals (China) Preferred specimen: NP swab; nasal aspirate or nasal wash are suitable alternatives For patients with lower respiratory tract illness, a lower respiratory tract specimen (e.g., an endotracheal aspirate or bronchoalveolar lavage) is preferred 44
Feline Influenza (H7N2) in NYC Over 100 cats tested positive for H7N2 across all NYC animals shelters Only one confirmed human infection was identified in the more than 300 individuals screened Veterinarian with close and prolonged contact with sick cats Illness was very mild and the individual recovered completely This was the first reported case due to exposure from an infected cat Only two other H7N2 human cases (due to exposure from infected turkeys/chickens) Risk to humans very low and no evidence that the outbreak affected Virginia in any way
H3N2v Testing Criteria ILI Recent (within 7 days of illness onset) contact with swine or recent attendance at an event (such as an agricultural fair) where swine were present Contact with swine may be direct contact (i.e., touching or handling a pig) or indirect contact (coming within about 6 feet (2 meters) of a pig without known direct contact). Preferred specimen: NP swab; nasal aspirate or nasal wash are suitable alternatives 46
MERS Person Under Investigation: Specimen Collection and Testing Collect multiple specimens from different sites at different times after symptom onset, if possible. Testing for MERS-CoV: Lower respiratory tract specimen (sputum, tracheal aspirate, bronchoalveolar lavage, or pleural fluid), This is a priority specimen Upper respiratory tract specimen (combined NP/OP swab), AND Blood/serum are required Collect respiratory specimens as soon as possible after symptoms begin Ideally within 7 days and before antiviral medications are administered Use appropriate infection control precautions Consult with DSI and DCLS prior to specimen submission Outbreak ID: RES989MERSCOV17 http://www.dgs.state.va.us/DivisionofConsolidatedLaboratoryServices/Ho tTopics/tabid/1531/Default.aspx 47













 Update")
 Update")



")


















 Variant Virus")






 in NYC")



![Preventing Influenza at [Name of Critical Access Hospital]](/thumb/233818/preventing-influenza-at-name-of-critical-access-hospital.jpg)