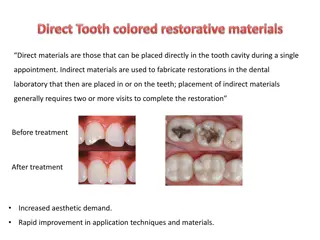
Understanding Cementum in Dental Anatomy

Cementum is a vital component of the tooth root, forming a protective layer. It is a calcified tissue with specific constituents and chemical composition. Cementogenesis involves a complex process of differentiation and mineralization, regulated by key molecular factors. Cells like cementoblasts and cementocytes play essential roles in cementum formation and maintenance.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
CEMENTUM DR. K. LAKSHMIKANTH, PROFESSOR 1 SIBAR INSTITUTE OF DENTAL SCIENCES DEPARTMENT OF PERIODONTICS
DEFINITION: Cementum is a calcified, avascular, mesenchymal tissue that forms the outer covering of the anatomic root. 2
CONSTITUENTS Collagen fibrils Interfibrillar matrix. 3
CHEMICALCOMPOSITION: Inorganic content:- 40 -50% Organic material and water:50-55% 4
CEMENTOGENESIS Cementum formation is preceded by deposition of dentin along the inner aspect of hertwig s epithelial root sheath. Once the dentin formation is underway, break occurs in the epithelial root sheath allowing the newly formed dentin to come in direct contact with connective tissue of the dental follicle. Cells derived from this connective tissue are responsible for cementum formation. 5
Soon after HER breaks up, undifferentiated mesenchymal cells from adjacent connective tissue differentiate into cementoblasts. Cementoblasts synthesize organic matrix(cementoid). It produces a compatible environment for cementoblasts . Then the mineralization begins . Calcium and phosphate ions present in the tissue fluids are deposited in the matrix and are arranged as unit cells of hydroxyapatite. 6
Mineralization begins in the depth of the cementoid. Fine hydroxyapatite crystals deposited initially between and later on within the collagen fibrils. 7
Key molecular factors regulating cementogenesis:- 1.TGF super family 2.PDGF & insulin like growth factors 3.FGF 4.Adhesion molecules 5.Enamel proteins 6.Collagens 8
CELLSOFCEMENTUM:- A. Cementoblasts:- Lines the cementoid tissue. 9
B. Cementocytes: Present in the cellular cementum. Lies in the space designated as lacunae. It has numerous canaliculi radiating from its cell body. These processes anastamose with those of harbouring cell. 10
C. Cementoclasts:- They are responsible for extensive root resorption which leads to primary teeth exfoliation Origin is unknown. 11
CEMENTOENAMEL JUNCTION- Three types of relationships involving the cementum may exist at the CEJ. In approximately 60% of the teeth, cementum overlaps the cervical end of the enamel for a short distance. In approximately 30% of all teeth cementum meets the cervical end of enamel in a relatively sharp line. In about 10% of the teeth , enamel and cementum do not meet. 12
CEMENTODENTINAL JUNCTION:- Relatively smooth in permanent teeth. In deciduous teeth, however, it is scalloped sometimes. The cemental fibers intermingle with the dentinal fibers at the CDJ more in cellular cementum than in acellular cementum and aid in attachment of cementum to the dentin. 14
CLASSIFICATION OF CEMENTUM Schroeder in 1986 gave the classification of cementum: Acellular afibrillar cementum(AAC) Acellular extrinsic fiber cementum(AEFC) Cellular mixed stratified cementum(CMSC) Cellular intrinsic fiber cementum(CIFC) Intermediate cementum 15
ACELLULAR CEMENTUM AND CELLULAR CEMENTUM: Acellular cementum:- First formed cementum. Cover approximately cervical third or of the root. Does not contain cells. Formed before tooth reaches occlusal plane. Thickness 30-230 micrometers. Sharpeys s fibers makes up the most of the portion of the structure of acellular cementum. Play principal role in supporting tooth. These sharpey s fibers are completely calcified. 16
Cellular cementum:- Formed after tooth reaches the occlusal plane. Present at the apical 1/3rd of the root. Contains cells (cementocytes). Sharpey s fibers forms small portion. Less calcified than the acellular cementum. It is thicker than acellular cementum. Histological microscopic view 17
Acellular afibrillar cementum: 1. Contains neither cells nor fibers. 2. Contains only mineralized ground substance. 3. Product of cementoblasts. 4. Thickness 1-15 m. 5.The lack of collagen fibers in this cementum indicates that this cementum variety has no function in tooth attachment. 18
ACELLULAREXTRINSICFIBERCEMENTUM:- It is the first formed cementum & is present at the cervical 1/3rd of the root. It s formation commences shortly after crown formation is completed. Thickness 30-230 m. Product of fibroblasts and cementoblasts. 19
CELLULAR MIXED STRATIFIED CEMENTUM: Contains extrinsic and intrinsic fibers and may contain cells. Co-product of fibroblast and cementoblasts. Thickness is 100-1000 . It is present in the apical 1/3rd of roots and furcation areas It consists of bulk of secondary cementum 20
CELLULAR INTRINSIC FIBER CEMENTUM: Contains cells, but no extrinsic collagen fibers. In humans it fills resorption lacunae. Product of cementoblasts. It also considered to be a form of reparative cementum. 21
INTERMEDIATE CEMENTUM: Thin, non cellular, amorphous layer of hard tissue of approximately 10 m thick. It is a poorly defined zone near the CDJ of certain teeth . Contains cellular remnants of HERS embedded in calcified ground substance. 22
TYPE,DISTRIBUTION& FUNCTION TYPE ORIGIN OF FIBERS Extrinsic LOCATION FUNCTION Acellular(primar y) From cervical margin to the apical 1/3rd anchorage Cellular(seconda ry) Intrinsic Middle to apical 1/3rd and furcations Adaptation & repair. Mixed Intrinsic and extrinsic Apical portion and furcation Adaptation Acellular afibrillar _ Spurs over enamel and dentin No known function along the CEJ 23
FUNCTIONS OF CEMENTUM: Anchorage: The primary function of Cementum is to furnish a medium for the attachment of collagen fibers that bind to tooth to alveolar bone The exfoliated teeth are characterized by an almost total absence of cementum. 24
Adaptation: Cementum is the tissue that makes functional adaptation of teeth possible. For eg:- Deposition of cementum at apical area- compensate for loss of tooth substance from occlusal wear. 25
Repair: Cementum serves as the major reparative tissue for root surfaces. The cementum formed during repair resembles cellular cementum because, It forms faster has a wide cementoid zone the apatite crystals are smaller. 26
INCREMENTALLINES: Incremental lines:-Both cellular and acellular cementum are arranged in lamellae separated by incremental lines parallel to the long axis of the tooth. These lines represent the rest periods in cementum and are more mineralized than the adjacent cementum. In acellular cementum, these lines tend to be close together, thin and even. In the more rapidly formed cellular cementum, these are farther apart, thicker and more regular. Histological microscopic view 27
AGECHANGESINCEMENTUM: The relatively smooth surface of the cementum becomes more irregular. Continuous increase in the apical zone may obstruct the apical canal. Cementum resorption is one of the characteristic of aging cementum. The permeability of cementum decreases with age. 28
Exposure of cementum to oral cavity: It occurs in cases of gingival recession and pocket formation. The cementum is sufficiently permeable to organic substances, inorganic ions and bacteria in these cases. Bacterial invasion of the cementum occurs frequently in periodontal disease. Cementum caries can develop in these cases. 30
CLNICAL PICTURE EXPOSURE OF CEMENTUM TO ORAL CAVITY 31
CLNICAL PICTURE 32 ROOT CARIES
Ankylosis: Fusion of cementum and alveolar bone with obliteration of the PDL is termed ankylosis. This condition is frequently uncommon and occurs most frequently in the primary dentition. It results in the resorption of the root and it s gradual replacement by bone tissue. For this reason, reimplanted teeth that ankylose will lose their roots after 4-5 years and will be exfoliated. 33
ANKYLOSIS 34
HYPERCEMENTOSIS :- Refers to the prominent thickening of the cementum. It is largely an age related phenomenon. May be localized or generalized. It occurs as a nodular enlargement of the apical 1/3rd of the root or spike like excrescence. 35
HYPERCEMENTOSIS RADIOGRAPHIC VIEW CLNICAL PICTURE 36
HYPOCEMENTOSIS:- Also known as acementosis. Rare developmental anomaly of tooth. Prevents normal development of periodontal attachment & dentin formation. Premature loss of all deciduous & permanent teeth may occur. 37
Cementicles: A cementicle is a calcified ovoid, or round nodule found in the PDL. They may develop from Calcified epithelial rests CLINICAL PICTURE From calcified sharpey s fibers Calcified thrombosed vessels within the PDL. They may lie free in the PDL, or attached / embedded in the cementum. This may impart a roughened globular out line to the root surface. 38
Cemental tears: Some times small spicules of cementum may be torn from the root surface. If they lie free in the PDL and may resemble cementicles Cemental tears may be formed as a result of traumatic injury. 39
Cementopathia: One of the clinical sign of hypophosphatasia. Some children with childhood periodontitis could have mild forms of hypophosphatasia with no other clinical signs of the disease than premature loss of deciduous teeth. 40
Concrescence: It is usually a form of fusion which occurs after root formation is completed. In this condition two adjacent teeth are united by cementum alone without confluence of underlying dentin. It is thought to arise as a result of traumatic injury or crowding of the tooth with resorption of interdental bone so that the two roots are in close approximation and become fused by the deposition of cementum between them. Frequently seen in posterior maxillary area. 41
CONCRESCENCE CLINICAL AND RADIOGRAPHIC PICTURES 42