Case Presentation on Ovarian Malignancy at St. Philomena's Hospital, Bengaluru
Mrs. X, a 42-year-old housewife, presented with irregular menses and lower abdominal pain. She had a history of weight loss, weakness, and decreased appetite over three years. No other significant complaints reported. Past history includes HbsAg positivity and iron deficiency anemia. Personal history shows a normal lifestyle. General physical examination revealed a conscious, oriented patient with a BMI of 20 kg/m2.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
case presentation On OVARIAN MALIGNANCY Dr. Pooja Koli Dr. Afreen Syed St. Philomena s hospital, Bengaluru
Name -Mrs X Age -42 yrs OCCUPATION: HOUSE WIFE Wife Of Mr Y Education -Studied upto 10 th class Socio economic status class 4 (modified Kuppuswamy classification) Residence Ulsoor
CHIEF irregular menses since 2 months pain in lower abdomen since 2 days COMPLAINTS
HISTORY OF PRESENTING ILLNESS Patient was apparently normal 2 days back c/o pain in lower abdomen insidious, dull aching , associated with lower backache increased on turning to sides from lying down position. irregular menses since 2 months- 6-7 days/ 10- 15 days, 5-6 pads/day, increased flow associated with clots/ no dysmenorrhea. H/o generalized weakness since 3 years with moderate work. H/o weight loss 20 kgs over 3 years H/o decreased appetite since 3 years No c/o breathlessness No c/o abdominal distention No c/o swelling of legs No c/o urinary / bowel disturbances No c/o vomiting / fever/ hemoptysis/ hemetemesis No c/o evening rise of temperature No c/o abnormal discharge p/v
Attained menarche at age of 13 yrs Irregular cycles x 2 months as mentioned above MENSTRUAL HISTORY LMP- 09/11/2022 Previous menstrual cycles regular , 4-5 days/ 28-30 days, average flow, no dysmenorrhea OBSTETRIC HISTORY
CONTRACEPTIV E HISTORY
PASTHISTORY FAMILY HISTORY K/C/O HbsAg positive since 2018 started on Tab. Entecavir 0.5mg od. H/o 2 pint PRBC transfusion i/v/o iron deficiency anemia 3 years back. No h/o Hypertension/ diabetes mellitus /thyroid disorders/ epilepsy / asthma /TB /breast disease/allergy/cardiac disease. No h/o Hypertension/ diabetes mellitus epilepsy / asthma /TB /breast disease/allergy/ thyroid disorders/cardiac disease in family No h/o breast cancer, endometrial carcinoma, ovarian or colorectal cancer history in family
PERSONALHISTORY Consumes mixed diet Normal sleep pattern Normal bowel and bladder habits No h/o drug addiction/ not an alcoholic / smoker
GENERALPHYSICALEXAMINATION Patient conscious , oriented , moderately built and poorly nourished. Height 163 cm , weight 53 kg ,BMI 20 kg / m2 Afebrile. Pulse rate 86 bpm , regular in rhythm , normal volume. Blood pressure 120 / 70 mmHg Respiratory rate 18 cycles / minute pallor- grade 2 No icterus/ cyanosis / clubbing / pedal edema / significant lymphadenopathy Breast /thyroid/ Spine normal
SYSTEMICEXAMINATION Central nervous system - no focal neurological deficit Cardiovascular examination NAD Respiratory system - decreased air entry B/L lower lobe RT>LT , no added sounds.
PER ABDOMENEXAMINATION INSPECTION Distension of lower abdomen noted in the center Umbilicus mid position and everted All quadrants move equally with respiration Tubectomy scar noted No visible pulsations/ engorged veins , no sinus. Hernial orifices free
PALPATION mass felt in lower abdomen extending upto umbilicus, mild tenderness +, no guarding Surface appears smooth with well defined upper and lateral borders, Lower border not felt, variegated consistency ( firm towards right side, cystic consistency towards left side). restricted vertical and transverse mobility - mass is not freely mobile. No hepatomegaly / splenomegaly Inguinal lymph nodes not palpable
PERCUSSION AUSCULTATION dullness over the mass present No bruit over the mass. resonance present in the flanks Normal bowel sounds heard. No shifting dullness /fluid thrill
LOCALEXAMINATION External genitalia appeared normal PERSPECULUMEXAMINATION Cervix, vagina healthy. No discharge noted. BIMANUAL EXAMINATION uterus could not be assessed separately from mass, anterior forniceal fullness + , mild tenderness +, mass felt upto umbilicus, parametrium free. PER RECTAL EXAMINATION mass felt anteriorly, no nodules felt in pouch of Douglas, rectal mucosa free.
SUMMARY 42 years lady ,P2L2 with HBsAg positive, c/o abdominal pain since 2 days, irregular periods since 2 months, generalized weakness on moderate work since 3 years, significant weight loss of 20 kg in 3 years with abdominopelvic mass extending upto umbilicus, variegated consistency, regular borders and restricted vertical and transverse mobility probably ovarian neoplasm for evaluation.
DIAGNOSIS 42 Years lady P2L2 with HBsAg positive status with abdominopelvic mass -?ovarian neoplasm
INVESTIGATIONS Complete hemogram Hb 6.7 g/dl, TC 7800 LFT , RFT, Coagulation profile NORMAL CA 125 192 U/ml AFP- 5 ng/ml LDH- 464 U/L Chest x ray B/L minimal pleural effusion ECG Normal Echo mild pericardial effusion, left ventricular diastolic dysfunction grade II, IVC mildly dilated and partially collapsing
ULTRASOUNDABDOMENANDPELVIS CT ABDOMENANDPELVIS Uterus normal size, AV,left ovary appears normal size , shape and echopattern, large right ovarian complex cyst measuring 21x 13 x 17 cms volume- 2250cc, with thick septations with min debris and mural nodule shoeing mild internal vascularity on doppler study.no signs of torsion noted, Min fluid in POD noted. Uterus normal size, large multiseptated cyst mass 20.2 x 18x 12 cm in lower abdomen and pelvis with nodular outline of septations showing homogenous enhancement, multiple mural nodules / soft tissue also noted, largest measure- 5x 4 cms, in upper anterior wall, right ovary not seen separately, left ovary normal. Bowel and mesentery displaced around the lesion, anteriorly abutting ant abdominal wall -? Right ovarian cystadenocarcinoma. ? Mild hepatitis , mild splenomegaly - ? Portal hypertension. Minimal Right pleural effusion noted. Mild ascites , mild spleenomegaly with dilated portal and splenic veins. Large complex right ovarian mucinous cystadenoma.
SURGERY Bowel preparation , prior liquid diet , peglec previous day ,iv fluids Mid line vertical incision Inspect Frozen section staging laparotomy
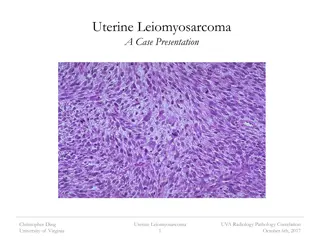
Frozen Section Poorly differentiated papillary carcinoma.