Managing Radiation Accidents: Challenges and Strategies

 undefined
undefined


Intern
邱詡懷


9/9/2014
H.H. Chiu @ VGHTPE 2014
2
R
a
d
i
a
t
i
o
n
a
c
c
i
d
e
n
t
:
any
unintended event
, including operating errors, equipment failures or other
mishaps, the consequences or potential consequences of which are not
negligible
from the point of view of protection or safety
M
a
n
a
g
e
m
e
n
t
o
f
r
a
d
i
a
t
i
o
n
e
x
p
o
s
u
r
e
i
s
d
i
f
f
i
c
u
l
t
misinformation
current perceptions about the effects of exposure
International Atomic Energy Agency (IAEA)
and
WHO
to publish
guidelines on the health management of radiation accidents
9/9/2014
H.H. Chiu @ VGHTPE 2014
3
1. Dispersal of radio-substance with /without
explosives
2. Power plants/ reactors
3. Nuclear weapons
4. Medical cyclotrons
9/9/2014
H.H. Chiu @ VGHTPE 2014
4
T
e
r
r
o
r
i
s
t
-
m
e
d
i
a
t
e
d
e
x
p
o
s
u
r
e
difficult to mass expose people to large doses of radiation
from other source
A combination of
radiation with chemical and
biological agents
is possible, but synergism between
radiation and these agents is unlikely.
9/9/2014
H.H. Chiu @ VGHTPE 2014
5
Management of the
immediate effects
of chemical
and biological exposure would take priority over
management of the effects of radiation exposure.
Dispersal of radioactive substances could be
mediated
with and without the use of explosives
9/9/2014
H.H. Chiu @ VGHTPE 2014
6
Radioactive material along with explosives would be to cause additional
fear and
panic
.
Mass hysteria such as that induced by fear of radiation ‘bombs’ can lead to more
non-
radiation or non-traumatic effects
such as chaos
The extent of dispersal of radioactivity would depend on
the strength of the explosives, the physical form of the radiation source used, the site of the
event, and the atmospheric conditions.
Major health hazards would probably
be restricted to a radius of 1 km
.
The aim of the emergency response would be to calm down and control the mass
hysteria as well as monitor and control the contamination area.
9/9/2014
H.H. Chiu @ VGHTPE 2014
7
L
o
w
-
l
e
v
e
l
r
a
d
i
o
a
c
t
i
v
e
s
o
u
r
c
e
s
such as those in smoke detectors, radiopharmaceuticals (used in nuclear medicine) and
isotopes used in research may be used to cause fear and panic.
No immediate health effects
would be expected and the probability of any long-term effects
would be very low.
H
i
g
h
l
y
r
a
d
i
o
a
c
t
i
v
e
s
o
u
r
c
e
s
such as
cobalt-60, caesium-137
(used in radiotherapy machines) and
iridium-192
(used in
industrial radiographic devices) can cause serious exposure.
usually metallic and easily detectable at check-points
Serious exposure would probably involve those who have handled the sources or those with
local radiation-induced skin injuries
9/9/2014
H.H. Chiu @ VGHTPE 2014
8
9/9/2014
H.H. Chiu @ VGHTPE 2014
9
An attack on a commercial nuclear power plant is a possibility
The reactor core is encased in a thick stainless steel jacket embedded within concrete.
If an accident occurs, the reactor is designed to slow down and stop the reaction.
The
coolant system
of a reactor does contain some radioactivity and if damaged
would release radioactive iodine and noble gases.
9/9/2014
H.H. Chiu @ VGHTPE 2014
10
C
h
e
r
n
o
b
y
l
n
u
c
l
e
a
r
p
o
w
e
r
p
l
a
n
t
,
w
h
i
c
h
h
a
d
b
e
e
n
c
o
n
s
t
r
u
c
t
e
d
w
i
t
h
o
u
t
a
c
o
n
t
a
i
n
m
e
n
t
v
e
s
s
e
l
,
r
e
s
u
l
t
e
d
i
n
2
3
7
p
e
r
s
o
n
s
b
e
i
n
g
o
v
e
r
e
x
p
o
s
e
d
A
less likely scenario
.
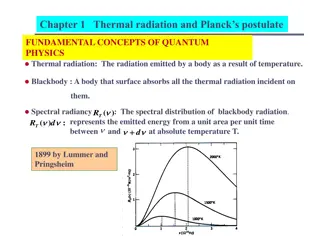
It should be noted that the destructive effects of nuclear weapons are due to
air blast
and thermal radiation
.
Uranium enriched with the
235 U isotope
is used in the nuclear industry as fuel for
nuclear reactors and nuclear bombs.
U
r
a
n
i
u
m
i
s
h
i
g
h
l
y
t
o
x
i
c
w
h
e
n
p
e
r
s
o
n
n
e
l
a
r
e
s
u
b
j
e
c
t
e
d
t
o
a
c
u
t
e
e
x
p
o
s
u
r
e
,
w
h
i
c
h
m
a
y
c
a
u
s
e
k
i
d
n
e
y
d
a
m
a
g
e
a
c
o
n
c
e
n
t
r
a
t
i
o
n
o
f
3
μ
g
u
r
a
n
i
u
m
/
g
o
f
k
i
d
n
e
y
t
i
s
s
u
e
s
h
o
u
l
d
n
o
t
b
e
e
x
c
e
e
d
e
d
,
a
n
d
t
o
t
h
i
s
e
n
d
l
e
g
i
s
l
a
t
i
o
n
r
e
s
t
r
i
c
t
s
l
o
n
g
-
t
e
r
m
(
8
h
)
w
o
r
k
p
l
a
c
e
a
i
r
c
o
n
c
e
n
t
r
a
t
i
o
n
s
o
f
s
o
l
u
b
l
e
u
r
a
n
i
u
m
t
o
0
.
2
m
g
/
m
a
n
d
s
h
o
r
t
-
t
e
r
m
a
i
r
c
o
n
c
e
n
t
r
a
t
i
o
n
s
(
1
5
m
i
n
)
t
o
0
.
6
m
g
/
m
9/9/2014
H.H. Chiu @ VGHTPE 2014
11
The cyclotron is the most widely used particle accelerator for producing
medically important radionuclides.
Cyclotron radiation surveys are an integral part of the overall radiation
safety in the cyclotron facility
Individuals who work in cyclotron facilities should be guided by the
IAEA recommendations regarding dose limits
9/9/2014
H.H. Chiu @ VGHTPE 2014
12
9/9/2014
H.H. Chiu @ VGHTPE 2014
13
The types of casualty expected of any blast include injuries due
to flying
fragments and collapsing buildings, flash burns and radiation effects.
S
t
a
t
i
s
t
i
c
s
f
r
o
m
t
h
e
b
l
a
s
t
s
i
n
J
a
p
a
n
s
h
o
w
t
h
a
t
8
5
%
o
f
i
n
j
u
r
i
e
s
s
u
s
t
a
i
n
e
d
w
e
r
e
d
u
e
t
o
t
r
a
u
m
a
a
n
d
b
u
r
n
s
:
r
a
d
i
a
t
i
o
n
a
c
c
o
u
n
t
e
d
f
o
r
o
n
l
y
1
5
%
.
Burns may be classified as flash burns and thermal burns
Flash burns :
Infrared and ultraviolet rays of very high intensity over a short
period. The range of flash burns is up to about 3650 m
Radiation sickness, Psychological trauma
9/9/2014
H.H. Chiu @ VGHTPE 2014
14
Individuals who have
been overexposed
or are suspected of overexposure, and who
present with signs of injuries such as trauma, burn and chemical contamination.
managed as in any medical emergency.
specific emergency tests (blood cell counts, blood sampling for cytogenetic studies and HLA
typing)
Individuals who have been
exposed
externally and have suffered external and internal
contamination or are suspected of having been exposed.
Go to centre where they can undergo secondary triage into three subcategories:
(a) Exposure of the whole body
(b) Local exposure of parts of the body
(c) Contamination with radionuclides
Individuals who have received
low doses
and are free from any other injury.
outpatients for a few days.
9/9/2014
H.H. Chiu @ VGHTPE 2014
15
Individuals contaminated either externally or internally should be identified and
treatment should be started
immediately and specifically
.
Medical treatment should be delivered in accordance with the type of
trauma
and the
urgency
of each case.
T
h
e
n
e
e
d
f
o
r
e
m
e
r
g
e
n
c
y
t
r
e
a
t
m
e
n
t
i
s
d
e
t
e
r
m
i
n
e
d
i
n
i
t
i
a
l
l
y
b
y
t
h
e
p
r
e
s
e
n
c
e
o
f
c
o
n
v
e
n
t
i
o
n
a
l
i
n
j
u
r
i
e
s
s
u
c
h
a
s
t
r
a
u
m
a
,
w
o
u
n
d
s
a
n
d
t
h
e
r
m
a
l
o
r
c
h
e
m
i
c
a
l
b
u
r
n
s
.
Early clinical symptoms are very helpful for triage and decision making on medical
care.
nausea, vomiting, diarrhoea, and skin and mucosal erythema.
The decision on hospitalization in cases of whole-body exposure or local exposure
depends on the presence of particular early clinical signs
9/9/2014
H.H. Chiu @ VGHTPE 2014
16
9/9/2014
H.H. Chiu @ VGHTPE 2014
17
Radiation protection personnel, medical physics experts and preferably nuclear
medicine physicians must be informed.
T
h
e
r
a
d
i
a
t
i
o
n
a
d
v
i
s
o
r
e
s
t
a
b
l
i
s
h
e
s
a
r
a
d
i
a
t
i
o
n
c
o
n
t
a
m
i
n
a
t
i
o
n
c
o
n
t
r
o
l
l
i
n
e
.
Decontamination supplies should be made available
C
o
n
t
a
m
i
n
a
t
e
d
c
l
o
t
h
i
n
g
s
h
o
u
l
d
b
e
r
e
m
o
v
e
d
,
i
f
f
e
a
s
i
b
l
e
,
a
t
t
h
e
s
i
t
e
.
Also, the injured person should be wrapped in a clean sheet to prevent the possible spread
of contamination.
Other than the removal of contaminated clothing, no other type of decontamination should be
performed on a seriously injured person.
9/9/2014
H.H. Chiu @ VGHTPE 2014
18
T
h
e
r
e
a
r
e
t
w
o
m
e
t
h
o
d
s
o
f
m
o
n
i
t
o
r
i
n
g
f
o
r
b
o
d
y
s
u
r
f
a
c
e
c
o
n
t
a
m
i
n
a
t
i
o
n
,
D
i
r
e
c
t
a
n
d
I
n
d
i
r
e
c
t
D
i
r
e
c
t
m
e
t
h
o
d
simplest and most convenient, entails positioning the instrument probe directly over the
contaminated area.
This method allows the contamination level to be calculated in
Bq/cm 2
, and the
measurements can be related to the derived working limit for surface contamination.
I
n
d
i
r
e
c
t
m
e
t
h
o
d
measure the degree of loose contamination or to monitor contamination in an area of high
radiation background,
smears are taken that can be monitored outside the affected area.
In this method a filter paper is wiped over a known surface area (usually 0.01 m^2 ), placed
in a polythene envelope to avoid cross-contamination and then taken to an area of low
radiation background
9/9/2014
H.H. Chiu @ VGHTPE 2014
19
T
h
e
b
i
o
l
o
g
i
c
a
l
a
n
d
p
o
s
s
i
b
l
e
h
e
a
l
t
h
c
o
n
s
e
q
u
e
n
c
e
s
o
f
r
a
d
i
o
a
c
t
i
v
e
c
o
n
t
a
m
i
n
a
t
i
o
n
d
e
p
e
n
d
o
n
t
h
e
f
o
l
l
o
w
i
n
g
:
mode of entry, pattern of distribution, sites of deposition of radionuclides in organs, nature of the
radiation emission from the contaminating radionuclide, amount of radioactivity o
F
i
x
e
d
c
o
n
t
a
m
i
n
a
t
i
o
n
,
the radioactivity cannot be transmitted to personnel
the hazard is consequently that of
external
radiation in the body
L
o
o
s
e
c
o
n
t
a
m
i
n
a
t
i
o
n
becomes an internal radiation hazard
into the body through the mouth or skin or through inhalation of contaminated air.
Once the radioactive substance has been taken into the body, it will continue to irradiate
the body until either the activity has decayed or normal biological excretion has occurred.
T
h
e
r
e
m
a
y
b
e
a
c
o
m
b
i
n
a
t
i
o
n
o
f
f
i
x
e
d
a
n
d
l
o
o
s
e
c
o
n
t
a
m
i
n
a
t
i
o
n
w
i
t
h
o
r
w
i
t
h
o
u
t
i
n
j
u
r
i
e
s
9/9/2014
H.H. Chiu @ VGHTPE 2014
20
The purpose of contamination diagnosis is to obtain information
on the time of intake,
the nature of the radionuclides involved and the distribution of the radionuclides on the
surface of and within the organism.
C
l
a
s
s
i
f
i
e
d
u
n
d
e
r
t
h
r
e
e
h
e
a
d
i
n
g
s
:
s
o
l
u
b
l
e
(
i
o
n
i
c
)
,
p
a
r
t
i
c
u
l
a
t
e
a
n
d
c
o
l
l
o
i
d
a
l
.
The soluble (ionic) contaminants are normally associated with the surface of the
substrate by physical absorption or by ion exchange with the reactive groups (usually
acidic) present on the surface of most nonmetallic materials.
cations are attracted to the acidic surface, and in favourable conditions, particularly at low
concentrations
m
o
s
t
f
i
s
s
i
o
n
p
r
o
d
u
c
t
s
a
n
d
a
l
l
t
h
e
h
e
a
v
y
n
a
t
u
r
a
l
r
a
d
i
o
a
c
t
i
v
e
e
l
e
m
e
n
t
s
f
a
l
l
i
n
t
o
t
h
i
s
c
a
t
e
g
o
r
y
9/9/2014
H.H. Chiu @ VGHTPE 2014
21
U
r
a
n
i
u
m
i
s
r
e
a
b
s
o
r
b
e
d
a
s
u
r
a
n
y
l
i
o
n
a
n
d
i
n
t
h
e
b
l
o
o
d
i
s
b
o
u
n
d
a
s
a
c
o
m
p
l
e
x
c
o
m
p
o
u
n
d
w
i
t
h
p
r
o
t
e
i
n
a
n
d
b
i
c
a
r
b
o
n
a
t
e
s
i
n
t
h
e
c
e
l
l
w
a
l
l
,
a
n
d
,
i
n
s
t
e
a
d
o
f
c
y
l
i
n
d
r
i
c
a
l
c
e
l
l
s
,
c
u
b
i
c
c
e
l
l
s
a
r
e
c
r
e
a
t
e
d
,
w
h
i
c
h
a
r
e
n
o
t
c
a
p
a
b
l
e
o
f
n
o
r
m
a
l
f
u
n
c
t
i
o
n
.
M
a
n
y
c
a
s
e
s
o
f
l
u
n
g
c
a
n
c
e
r
a
n
d
k
i
d
n
e
y
d
i
s
o
r
d
e
r
h
a
v
e
b
e
e
n
r
e
p
o
r
t
e
d
i
n
u
r
a
n
i
u
m
w
o
r
k
e
r
s
.
Uranium is deposited in the following manner in the body:
22% is deposited in the
skeleton, 12.5% in kidneys and 12.2% in other soft tissue.
20% of uranium entering the body is retained in bone with a half-time of 20 days; and (b) 2%
is retained with a half-time of 5000 days.
12% of uranium is assumed to be deposited in soft tissue with a 6-day half-time and 0.5%
with a 1500-day half-time.
9/9/2014
H.H. Chiu @ VGHTPE 2014
22
Following accidental internal contamination with uranium (inhalation or
ingestion),
93.97% is eliminated from the body within 7 months of exposure
6.02% is ‘buried’ in bones, kidney and soft tissues (for up to 41 years in soft tissues
and up to 137 years in bones) and cannot be removed from the body by any means.
In the case of internal contamination, through inhalation, ingestion or
wounded or apparently undamaged skin, physical measurement
includes
thyroid
monitoring,
whole-body counting
,
gamma camera
measurement
, and analysis of blood and excreta.
all blood, urine and faecal samples have to be collected and labelled to record the
time of sampling.
9/9/2014
H.H. Chiu @ VGHTPE 2014
23
The severity of the injury
depends
on the dose level incurred, the dose rate, the radio-
sensitivity of the tissues involved, the area of the body exposed and the extent of
exposure suffered by the organ system.
The severity of the injury is greater when the whole body is exposed; partial body
exposure to the same dose has less impact on health.
A
n
a
b
s
o
r
b
e
d
r
a
d
i
a
t
i
o
n
d
o
s
e
o
f
a
b
o
u
t
3
.
5
G
y
i
s
g
e
n
e
r
a
l
l
y
e
x
p
e
c
t
e
d
t
o
r
e
s
u
l
t
i
n
t
h
e
d
e
a
t
h
o
f
5
0
%
o
f
t
h
e
e
x
p
o
s
e
d
p
o
p
u
l
a
t
i
o
n
g
r
o
u
p
w
i
t
h
i
n
2
m
o
n
t
h
s
i
f
t
h
e
r
e
i
s
n
o
m
e
d
i
c
a
l
t
r
e
a
t
m
e
n
t
.
This LD 50/60value can be increased to about
5.0–6.0 Gy
with sufficient medical
treatment
9/9/2014
H.H. Chiu @ VGHTPE 2014
24
A
v
e
r
y
e
a
r
l
y
c
l
a
s
s
i
f
i
c
a
t
i
o
n
w
i
l
l
b
e
b
a
s
e
d
o
n
c
l
i
n
i
c
a
l
s
y
m
p
t
o
m
s
s
u
c
h
a
s
n
a
u
s
e
a
,
v
o
m
i
t
i
n
g
,
d
i
a
r
r
h
o
e
a
,
e
r
y
t
h
e
m
a
a
n
d
f
e
v
e
r
.
a
s
w
e
l
l
a
s
t
h
e
t
i
m
e
o
f
t
h
e
i
r
a
p
p
e
a
r
a
n
c
e
T
h
i
s
p
e
r
m
i
t
s
t
h
e
c
l
a
s
s
i
f
i
c
a
t
i
o
n
o
f
v
i
c
t
i
m
s
i
n
t
o
t
w
o
c
a
t
e
g
o
r
i
e
s
a
c
c
o
r
d
i
n
g
t
o
w
h
e
t
h
e
r
t
h
e
a
b
s
o
r
b
e
d
d
o
s
e
i
s
g
r
e
a
t
e
r
o
r
l
e
s
s
t
h
a
n
2
G
y
Multidisciplinary team to identify the stage and extent of radiation injury by the end of
the first week.
Data provided by MRI, computerized tomography, vascular scintigraphy, histochemical and
immunocytochemical studies of biopsy material, as well as topographic dosimetry, including
in-depth distribution of the doses, and clinical evolution should all be taken into consideration
by a
9/9/2014
H.H. Chiu @ VGHTPE 2014
25
9/9/2014
H.H. Chiu @ VGHTPE 2014
26
A
m
u
l
t
i
d
i
s
c
i
p
l
i
n
a
r
y
t
e
a
m
a
p
p
r
o
a
c
h
i
s
r
e
q
u
i
r
e
d
,
i
n
v
o
l
v
i
n
g
m
e
d
i
c
a
l
p
h
y
s
i
c
i
a
n
s
,
n
u
c
l
e
a
r
m
e
d
i
c
i
n
e
p
h
y
s
i
c
i
a
n
s
,
r
a
d
i
a
t
i
o
n
p
r
o
t
e
c
t
i
o
n
o
f
f
i
c
e
r
s
,
p
l
a
s
t
i
c
a
n
d
r
e
c
o
n
s
t
r
u
c
t
i
v
e
s
u
r
g
e
o
n
s
,
m
e
d
i
c
a
l
o
n
c
o
l
o
g
i
s
t
s
a
n
d
h
a
e
m
a
t
o
l
o
g
i
s
t
s
.
Treatment has to be individualized according to the nature and grade of the combined
injuries.
E
x
p
e
r
t
a
d
v
i
c
e
f
r
o
m
e
x
t
e
r
n
a
l
o
r
g
a
n
i
z
a
t
i
o
n
s
s
u
c
h
a
s
I
A
E
A
,
P
u
b
l
i
c
H
e
a
l
t
h
E
n
g
l
a
n
d
o
r
a
s
i
m
i
l
a
r
b
o
d
y
i
n
i
n
d
i
v
i
d
u
a
l
c
o
u
n
t
r
i
e
s
s
h
o
u
l
d
b
e
s
o
u
g
h
t
.
As radiation injury is characterized by a
latent period
, all important treatments of the
nonradiation components of combined radiation injury should be carried out during the
first 2–3 weeks.
L
a
t
e
r
e
f
f
o
r
t
s
w
i
l
l
b
e
n
e
c
e
s
s
a
r
y
f
o
r
t
h
e
t
r
e
a
t
m
e
n
t
o
f
b
o
n
e
m
a
r
r
o
w
a
n
d
s
k
i
n
r
a
d
i
a
t
i
o
n
i
n
j
u
r
i
e
s
.
9/9/2014
H.H. Chiu @ VGHTPE 2014
27
S
o
a
p
w
a
s
h
s
h
o
u
l
d
s
u
f
f
i
c
e
.
for heavier contamination, care should be taken not to cause skin abrasion due to excessive
washing, and other decontamination agents should be used.
In the radiopharmaceutical industry a freshly reconstituted mixture
250 ml water with a powder containing 1.25 g natrii laurysulfas (soap and chelating agent), 1.25 g
amylum tritici (chelating agent for iodine, not iodide), 1.25 g natrii edetas (a strong chelating agent for
dissolved metals) and8.75 g sodium bicarbonate (regulation of pH) is used.
This is effective if used soon (within few hours) after contamination for the
decontamination of most regular radiopharmaceuticals (99m Tc based) and similar
agents (e.g. 131 I).
C
o
m
m
e
r
c
i
a
l
d
e
c
o
n
t
a
m
i
n
a
n
t
s
s
u
c
h
a
s
R
a
d
i
a
c
w
a
s
h
T
o
w
e
l
e
t
t
s
(
B
i
o
d
e
x
M
e
d
i
c
a
l
S
y
s
t
e
m
s
I
n
c
.
,
S
h
i
r
l
e
y
,
N
Y
,
U
S
A
)
a
r
e
u
s
e
d
e
x
t
e
n
s
i
v
e
l
y
i
n
h
o
s
p
i
t
a
l
s
9/9/2014
H.H. Chiu @ VGHTPE 2014
28
Deposition of radioactive particles in the
sinuses and lungs
is one of the more
common types of accidental exposures.
Insoluble particles, once inhaled into the lungs, may be mobilized and translocated to
other organs at a low rate over many months or years
Irrigation of the nasal passage
gently with saline solution or water using a catheter or
syringe is required. The subject’s head should be bent over a basin with mouth open
during this process.
In rare cases,
trachea–bronchial lavage
may be required.
9/9/2014
H.H. Chiu @ VGHTPE 2014
29
Occur from the dispersal of powdered,
liquid or gaseous
radioactive
material.
The material may enter the body by
inhalation or ingestion
, through
intact skin or through wounds or burns
.
There are several general approaches to the treatment of internal
contamination :
(1) Mobilization as a means of elimination from tissue
(2) Chelating
(3) Reduction of absorption
(4) Dilution, blockage
(5) Displacement by nonradioactive materials
9/9/2014
H.H. Chiu @ VGHTPE 2014
30
9/9/2014
H.H. Chiu @ VGHTPE 2014
31
Elimination by extracorporeal treatment :
Haemodialysis
Lavage :
Lavage of the tracheobronchial tree,
only in patients exposed to high doses to prevent acute or subacute effects such as
radiation
pneumonitis or fibrosis.
Thyroid blocking : radio-iodine
Bone marrow transplantation(BMT) :
accidental whole-body irradiation when the dose is sufficiently high to make spontaneous
bone marrow recovery impossible
Haematopoietic growth factors :
granulocyte-colony stimulating factors and granulocyte macrophage colony stimulating
factors
9/9/2014
H.H. Chiu @ VGHTPE 2014
32
I
f
t
h
e
l
y
m
p
h
o
c
y
t
e
c
o
u
n
t
d
u
r
i
n
g
t
h
e
f
i
r
s
t
w
e
e
k
i
s
w
i
t
h
i
n
t
h
e
r
a
n
g
e
o
f
0
.
2
–
0
.
5
g
/
l
(
2
0
0
–
5
0
0
c
e
l
l
s
/
μ
l
)
,
s
p
o
n
t
a
n
e
o
u
s
r
e
c
o
v
e
r
y
i
s
p
o
s
s
i
b
l
e
.
Therapy comprises isolation, antibiotics and supportive treatment, including platelet
infusion. Growth factors can be used.
If the lymphocyte count in the first week is lower than
0.2 g/l,
the stem
cells are probably irreversibly damaged.
Treatments are as above. Additional growth factor therapy is a method of choice.
If the lymphocyte count within the first week is less than
0.1 g/l
,
treatment with growth factors and BMT has to be considered
9/9/2014
H.H. Chiu @ VGHTPE 2014
33
N
u
c
l
e
a
r
m
e
d
i
c
i
n
e
p
h
y
s
i
c
i
a
n
s
h
a
v
e
t
o
b
e
w
e
l
l
o
r
g
a
n
i
z
e
d
i
n
o
r
d
e
r
t
o
d
e
l
i
v
e
r
s
u
i
t
a
b
l
e
m
a
n
a
g
e
m
e
n
t
i
n
a
n
y
k
i
n
d
o
f
r
a
d
i
a
t
i
o
n
a
c
c
i
d
e
n
t
,
w
h
i
c
h
i
n
c
l
u
d
e
s
f
a
s
t
t
r
i
a
g
e
o
f
i
n
j
u
r
e
d
p
e
r
s
o
n
s
,
p
r
o
m
p
t
d
i
a
g
n
o
s
i
s
o
f
r
a
d
i
a
t
i
o
n
c
a
s
u
a
l
t
i
e
s
a
n
d
u
r
g
e
n
t
i
n
i
t
i
a
t
i
o
n
o
f
s
p
e
c
i
f
i
c
t
r
e
a
t
m
e
n
t
p
r
o
c
e
d
u
r
e
s
.
9/9/2014
H.H. Chiu @ VGHTPE 2014
34
Thanks for your attention
Have a nice day
9/9/2014
H.H. Chiu @ VGHTPE 2014
35
Radiation accidents present significant challenges in terms of managing exposure and mitigating consequences. International organizations like the IAEA and WHO provide guidelines for handling such incidents. Possible scenarios include dispersal of radioactive substances in various contexts, such as terrorist-mediated exposure or accidents in power plants. Strategies for managing these scenarios involve prioritizing immediate effects and controlling mass hysteria. Effective management requires a multi-faceted approach that addresses both the physical and psychological impacts of radiation accidents.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Radiation accidents and their managements Intern
2 H.H. Chiu @ VGHTPE 2014 9/9/2014
Introduction Radiation accident : any unintended event, including operating errors, equipment failures or other mishaps, the consequences or potential consequences of which are not negligible from the point of view of protection or safety Management of radiation exposure is difficult misinformation current perceptions about the effects of exposure International Atomic Energy Agency (IAEA) and WHO to publish guidelines on the health management of radiation accidents 3 H.H. Chiu @ VGHTPE 2014 9/9/2014
Possible accident scenarios 1. Dispersal of radio-substance with /without explosives 2. Power plants/ reactors 3. Nuclear weapons 4. Medical cyclotrons 4 H.H. Chiu @ VGHTPE 2014 9/9/2014
Dispersal of radio-substance -I Terrorist-mediated exposure difficult to mass expose people to large doses of radiation from other source A combination of radiation with chemical and biological agents is possible, but synergism between radiation and these agents is unlikely. 5 H.H. Chiu @ VGHTPE 2014 9/9/2014
Dispersal of radio-substance II Management of the immediate effects of chemical and biological exposure would take priority over management of the effects of radiation exposure. Dispersal of radioactive substances could be mediated with and without the use of explosives 6 H.H. Chiu @ VGHTPE 2014 9/9/2014
Dispersal with explosives Radioactive material along with explosives would be to cause additional fear and panic. Mass hysteria such as that induced by fear of radiation bombs can lead to more non- radiation or non-traumatic effects such as chaos The extent of dispersal of radioactivity would depend on the strength of the explosives, the physical form of the radiation source used, the site of the event, and the atmospheric conditions. Major health hazards would probably be restricted to a radius of 1 km. The aim of the emergency response would be to calm down and control the mass hysteria as well as monitor and control the contamination area. 7 H.H. Chiu @ VGHTPE 2014 9/9/2014
Dispersal without explosives Low-level radioactive sources such as those in smoke detectors, radiopharmaceuticals (used in nuclear medicine) and isotopes used in research may be used to cause fear and panic. No immediate health effects would be expected and the probability of any long-term effects would be very low. Highly radioactive sources such as cobalt-60, caesium-137 (used in radiotherapy machines) and iridium-192(used in industrial radiographic devices) can cause serious exposure. usually metallic and easily detectable at check-points Serious exposure would probably involve those who have handled the sources or those with local radiation-induced skin injuries 8 H.H. Chiu @ VGHTPE 2014 9/9/2014
9 H.H. Chiu @ VGHTPE 2014 9/9/2014
Power plants/ reactors An attack on a commercial nuclear power plant is a possibility The reactor core is encased in a thick stainless steel jacket embedded within concrete. If an accident occurs, the reactor is designed to slow down and stop the reaction. The coolant system of a reactor does contain some radioactivity and if damaged would release radioactive iodine and noble gases. Chernobyl nuclear power plant, which had been constructed without a containment vessel, resulted in 237 persons being overexposed 10 H.H. Chiu @ VGHTPE 2014 9/9/2014
Nuclear weapons A less likely scenario. It should be noted that the destructive effects of nuclear weapons are due to air blast and thermal radiation. Uranium enriched with the 235 U isotope is used in the nuclear industry as fuel for nuclear reactors and nuclear bombs. Uranium is highly toxic when personnel are subjected to acute exposure, which may cause kidney damage a concentration of 3 g uranium/g of kidney tissue should not be exceeded, and to this end legislation restricts long-term (8 h) workplace air concentrations of soluble uranium to 0.2 mg/m and short-term air concentrations (15 min) to 0.6 mg/m 11 H.H. Chiu @ VGHTPE 2014 9/9/2014
Medical cyclotrons The cyclotron is the most widely used particle accelerator for producing medically important radionuclides. Cyclotron radiation surveys are an integral part of the overall radiation safety in the cyclotron facility Individuals who work in cyclotron facilities should be guided by the IAEA recommendations regarding dose limits 12 H.H. Chiu @ VGHTPE 2014 9/9/2014
13 H.H. Chiu @ VGHTPE 2014 9/9/2014
Types of casulty The types of casualty expected of any blast include injuries due to flying fragments and collapsing buildings, flash burns and radiation effects. Statistics from the blasts in Japan show that 85% of injuries sustained were due to trauma and burns: radiation accounted for only 15%. Burns may be classified as flash burns and thermal burns Flash burns : Infrared and ultraviolet rays of very high intensity over a short period. The range of flash burns is up to about 3650 m Radiation sickness, Psychological trauma 14 H.H. Chiu @ VGHTPE 2014 9/9/2014
Triage of injured persons Individuals who have been overexposed or are suspected of overexposure, and who present with signs of injuries such as trauma, burn and chemical contamination. managed as in any medical emergency. specific emergency tests (blood cell counts, blood sampling for cytogenetic studies and HLA typing) Individuals who have been exposed externally and have suffered external and internal contamination or are suspected of having been exposed. Go to centre where they can undergo secondary triage into three subcategories: (a) Exposure of the whole body (b) Local exposure of parts of the body (c) Contamination with radionuclides Individuals who have received low doses and are free from any other injury. outpatients for a few days. 15 H.H. Chiu @ VGHTPE 2014 9/9/2014
Medical management of individuals Individuals contaminated either externally or internally should be identified and treatment should be started immediately and specifically. Medical treatment should be delivered in accordance with the type of trauma and the urgency of each case. The need for emergency treatment is determined initially by the presence of conventional injuries such as trauma, wounds and thermal or chemical burns. Early clinical symptoms are very helpful for triage and decision making on medical care. nausea, vomiting, diarrhoea, and skin and mucosal erythema. The decision on hospitalization in cases of whole-body exposure or local exposure depends on the presence of particular early clinical signs 16 H.H. Chiu @ VGHTPE 2014 9/9/2014
17 H.H. Chiu @ VGHTPE 2014 9/9/2014
Management at the scene Radiation protection personnel, medical physics experts and preferably nuclear medicine physicians must be informed. The radiation advisor establishes a radiation contamination control line. Decontamination supplies should be made available Contaminated clothing should be removed, if feasible, at the site. Also, the injured person should be wrapped in a clean sheet to prevent the possible spread of contamination. Other than the removal of contaminated clothing, no other type of decontamination should be performed on a seriously injured person. 18 H.H. Chiu @ VGHTPE 2014 9/9/2014
Monitoring for surface contamination There are two methods of monitoring for body surface contamination, Direct and Indirect Direct method simplest and most convenient, entails positioning the instrument probe directly over the contaminated area. This method allows the contamination level to be calculated in Bq/cm 2 , and the measurements can be related to the derived working limit for surface contamination. Indirect method measure the degree of loose contamination or to monitor contamination in an area of high radiation background, smears are taken that can be monitored outside the affected area. In this method a filter paper is wiped over a known surface area (usually 0.01 m^2 ), placed in a polythene envelope to avoid cross-contamination and then taken to an area of low radiation background 19 H.H. Chiu @ VGHTPE 2014 9/9/2014
Diagnosis The biological and possible health consequences of radioactive contamination depend on the following: mode of entry, pattern of distribution, sites of deposition of radionuclides in organs, nature of the radiation emission from the contaminating radionuclide, amount of radioactivity o Fixed contamination, the radioactivity cannot be transmitted to personnel the hazard is consequently that of external radiation in the body Loose contamination becomes an internal radiation hazard into the body through the mouth or skin or through inhalation of contaminated air. Once the radioactive substance has been taken into the body, it will continue to irradiate the body until either the activity has decayed or normal biological excretion has occurred. There may be a combination of fixed and loose contamination with or without injuries 20 H.H. Chiu @ VGHTPE 2014 9/9/2014
Removing the contaminants The purpose of contamination diagnosis is to obtain information on the time of intake, the nature of the radionuclides involved and the distribution of the radionuclides on the surface of and within the organism. Classified under three headings: soluble (ionic), particulate and colloidal. The soluble (ionic) contaminants are normally associated with the surface of the substrate by physical absorption or by ion exchange with the reactive groups (usually acidic) present on the surface of most nonmetallic materials. cations are attracted to the acidic surface, and in favourable conditions, particularly at low concentrations most fission products and all the heavy natural radioactive elements fall into this category 21 H.H. Chiu @ VGHTPE 2014 9/9/2014
Uranium Uranium is reabsorbed as uranyl ion and in the blood is bound as a complex compound with protein and bicarbonates in the cell wall, and, instead of cylindrical cells, cubic cells are created, which are not capable of normal function. Many cases of lung cancer and kidney disorder have been reported in uranium workers. Uranium is deposited in the following manner in the body: 22% is deposited in the skeleton, 12.5% in kidneys and 12.2% in other soft tissue. 20% of uranium entering the body is retained in bone with a half-time of 20 days; and (b) 2% is retained with a half-time of 5000 days. 12% of uranium is assumed to be deposited in soft tissue with a 6-day half-time and 0.5% with a 1500-day half-time. 22 H.H. Chiu @ VGHTPE 2014 9/9/2014
Uranium- internal vs external contamination Following accidental internal contamination with uranium (inhalation or ingestion), 93.97% is eliminated from the body within 7 months of exposure 6.02% is buried in bones, kidney and soft tissues (for up to 41 years in soft tissues and up to 137 years in bones) and cannot be removed from the body by any means. In the case of internal contamination, through inhalation, ingestion or wounded or apparently undamaged skin, physical measurement includes thyroid monitoring, whole-body counting, gamma camera measurement, and analysis of blood and excreta. all blood, urine and faecal samples have to be collected and labelled to record the time of sampling. 23 H.H. Chiu @ VGHTPE 2014 9/9/2014
Severity of the injury The severity of the injury depends on the dose level incurred, the dose rate, the radio- sensitivity of the tissues involved, the area of the body exposed and the extent of exposure suffered by the organ system. The severity of the injury is greater when the whole body is exposed; partial body exposure to the same dose has less impact on health. An absorbed radiation dose of about 3.5 Gy is generally expected to result in the death of 50% of the exposed population group within 2 months if there is no medical treatment. This LD 50/60value can be increased to about 5.0 6.0 Gy with sufficient medical treatment 24 H.H. Chiu @ VGHTPE 2014 9/9/2014
Classification of clinical symptoms A very early classification will be based on clinical symptoms such as nausea, vomiting, diarrhoea, erythema and fever. as well as the time of their appearance This permits the classification of victims into two categories according to whether the absorbed dose is greater or less than 2 Gy Multidisciplinary team to identify the stage and extent of radiation injury by the end of the first week. Data provided by MRI, computerized tomography, vascular scintigraphy, histochemical and immunocytochemical studies of biopsy material, as well as topographic dosimetry, including in-depth distribution of the doses, and clinical evolution should all be taken into consideration by a 25 H.H. Chiu @ VGHTPE 2014 9/9/2014
26 H.H. Chiu @ VGHTPE 2014 9/9/2014
Treatment A multidisciplinary team approach is required, involving medical physicians, nuclear medicine physicians, radiation protection officers, plastic and reconstructive surgeons, medical oncologists and haematologists. Treatment has to be individualized according to the nature and grade of the combined injuries. Expert advice from external organizations such as IAEA, Public Health England or a similar body in individual countries should be sought. As radiation injury is characterized by a latent period, all important treatments of the nonradiation components of combined radiation injury should be carried out during the first 2 3 weeks. Later efforts will be necessary for the treatment of bone marrow and skin radiation injuries. 27 H.H. Chiu @ VGHTPE 2014 9/9/2014
Skin contamination Soap wash should suffice. for heavier contamination, care should be taken not to cause skin abrasion due to excessive washing, and other decontamination agents should be used. In the radiopharmaceutical industry a freshly reconstituted mixture 250 ml water with a powder containing 1.25 g natrii laurysulfas (soap and chelating agent), 1.25 g amylum tritici (chelating agent for iodine, not iodide), 1.25 g natrii edetas (a strong chelating agent for dissolved metals) and8.75 g sodium bicarbonate (regulation of pH) is used. This is effective if used soon (within few hours) after contamination for the decontamination of most regular radiopharmaceuticals (99m Tc based) and similar agents (e.g. 131 I). Commercial decontaminants such as Radiacwash Toweletts (Biodex Medical Systems Inc., Shirley, NY, USA) are used extensively in hospitals 28 H.H. Chiu @ VGHTPE 2014 9/9/2014
Respiratory tract contamination Deposition of radioactive particles in the sinuses and lungs is one of the more common types of accidental exposures. Insoluble particles, once inhaled into the lungs, may be mobilized and translocated to other organs at a low rate over many months or years Irrigation of the nasal passage gently with saline solution or water using a catheter or syringe is required. The subject s head should be bent over a basin with mouth open during this process. In rare cases, trachea bronchial lavage may be required. 29 H.H. Chiu @ VGHTPE 2014 9/9/2014
Internal contamination Occur from the dispersal of powdered, liquid or gaseous radioactive material. The material may enter the body by inhalation or ingestion, through intact skin or through wounds or burns. There are several general approaches to the treatment of internal contamination : (1) Mobilization as a means of elimination from tissue (2) Chelating (3) Reduction of absorption (4) Dilution, blockage (5) Displacement by nonradioactive materials 30 H.H. Chiu @ VGHTPE 2014 9/9/2014
31 H.H. Chiu @ VGHTPE 2014 9/9/2014
Other treatment Elimination by extracorporeal treatment : Haemodialysis Lavage : Lavage of the tracheobronchial tree, only in patients exposed to high doses to prevent acute or subacute effects such as radiation pneumonitis or fibrosis. Thyroid blocking : radio-iodine Bone marrow transplantation(BMT) : accidental whole-body irradiation when the dose is sufficiently high to make spontaneous bone marrow recovery impossible Haematopoietic growth factors : granulocyte-colony stimulating factors and granulocyte macrophage colony stimulating factors 32 H.H. Chiu @ VGHTPE 2014 9/9/2014
Criteria for choice of therapy If the lymphocyte count during the first week is within the range of 0.2 0.5 g/l (200 500 cells/ l),spontaneous recovery is possible. Therapy comprises isolation, antibiotics and supportive treatment, including platelet infusion. Growth factors can be used. If the lymphocyte count in the first week is lower than 0.2 g/l, the stem cells are probably irreversibly damaged. Treatments are as above. Additional growth factor therapy is a method of choice. If the lymphocyte count within the first week is less than 0.1 g/l, treatment with growth factors and BMT has to be considered 33 H.H. Chiu @ VGHTPE 2014 9/9/2014
Conclusion Nuclear medicine physicians have to be well organized in order to deliver suitable management in any kind of radiation accident, which includes fast triage of injured persons, prompt diagnosis of radiation casualties and urgent initiation of specific treatment procedures. 34 H.H. Chiu @ VGHTPE 2014 9/9/2014
Thanks for your attention Have a nice day 35 H.H. Chiu @ VGHTPE 2014 9/9/2014