Weighted Log-rank Tests in Survival Trials
Inference in survival trials:
Weighted log-rank tests and
some alternatives
Carl-Fredrik Burman, PhD, Assoc.Prof.
Statistical Innovation, Data Science & AI
AstraZeneca R&D, Gothenburg
29 April, 2021
2
Thanks to Dominic Magirr
for great collaboration
Back to Basics
1
What’s special with Survival Analysis?
STANDARD STATISTICAL PROBLEMS
•
Example 1: Two samples, normal distributions
•
Exampe 2: Zero-one responses
SURVIVAL ANALYSIS
1.
Responses are positive
•
May use transformation (e.g. log)
2.
We don’t have time to follow all patients (censoring)
•
Missing data, with known structure
3.
Competing risks, Treatment switching …
4
PhD advise:
Don’t complicate
things before
understanding
the basics
5
Statistical
inference
Clinical trial, comparing
New treatment, X,
versus
Standard of Care, C
What is (really) the main efficacy objective?
To ”compare” X and C
To show a (=any) difference
To show X has an efficacy benefit
Hypothesis testing
Null hypothesis
Test statistic (pre-specified)
Null distribution
6
Distributional assumptions
•
Does the
validity
of the statistical analysis require that assumptions are
correct?
•
Do we need uncertain assumptions to guarantee Type 1 Error control?
OR
•
Will assumptions only influence the power (sponsor’s risk)?
7
Two different bases for inference
showing treatment benefit
•
Distribution-based
•
E.g. ANCOVA, t-test has exactly correct Type 1 Error (only) if normal distributions +
same residual variance
•
Randomisation-based
•
Relies of nothing else than randomisation of patients
•
Any reasonable pre-specified test statistic; can handle covariates
•
In principle, randomisation test much more robust
•
In practise, distribution-based tests are often (but not always) good enough
to control Type 1 Error even if assumptions are not fully correct. Preferable
with approximate formula than simulated p-value?
8
Example dataset*
•
n=37 per arm
•
Group A: New treatment
•
Group B: Control
•
Survival time in days
•
Mice data
•
No censoring
9
* Loosely based on Xie et al (2017). Nature Communications 8:155.
Empiric CDFs and survival functions
10
Example dataset
11
Life times vs rank
12
Randomisation test (permutation test)
13
•
H
0
: Time does not depend on arm
•
That is, the highest observed time
could equally well have been on A
as B.
•
Same for next highest etc.
•
We can generate a null distribution
by keeping all observation fixed
but re-randomize … and repeat
e.g. one million times.
Randomisation test
14
•
We can generate a null distribution
by keeping all observation fixed
but re-randomize … and repeat
e.g. one million times.
p-value = 0.6%
All p-values 1-sided, as we want to show B better than A
Distribution-based inference: Z-test
•
Assumptions
•
I.i.d. Normal in each arm
•
Same known variance (taken equal to estimate)
•
p-value = 1.0%
•
P-value happens to be
higher than p
rand
=0.6%
•
Asymptotic Relative Efficiency of randomisation test vs Z-test is exactly 100% if Z-test
assumptions are OK
•
Z-test is approximately correct in many situations. Problems if few observations have
lrge impact on variance: outliers, heavy tails, …
•
(NB! All p-values are one-sided as we want to show B is better than A.)
15
N-distribution has
poor fit to data
T-test
•
Assumptions
•
I.i.d. Normal in each arm (Questionable assumption)
•
Same variance, estimated from data
•
p
T
=1.1%
•
Cf. p
Z
=1.0%, p
rand
=0.6%
•
T-test reflects change in null distribution due to random estimate of SD
•
Asymptotically t-test = Z-test
16
Lognormal test
17
Original
Log of data
•
With positive data, lognormal is sometimes better than normal
•
Not in this example
•
Recall: Test should be pre-specified
•
Log scale is dangerous if some life span is close to zero
•
NB! Tests are scale-and location-invariant
Transformations
•
Log transform, x
i
=log(t
i
)
•
Any monotone function f gives valid test based on x
i
=f(t
i
)
•
Randomisation test or – if distributional assumptions are appropriate – t-test, ANCOVA
etc based on transformed observations x
i
18
Estimands
•
The estimand framework can help us think,
structure discussions
•
But there are several contradicting dimensions
•
The best test to show treatment benefit may not
directly correspond to an easily understandable,
clinically attractive estimand
•
Average Hazard Ratio may not be the most natural
estimand (especially if HR varies greatly over time).
Still, that in itself may not disqualify using a
(perhaps weighted) logrank test
•
Tradeoff: Transformations can be useful but …
Don’t make it unnecessarily complicated
19
Simple and meaningful
•
What is clinically (most) important?
•
What is easy?
EXAMPLES
•
Mean survival
•
Proportion cured. Proxy: 5-year survival?
•
But easy and important may not mean statistically sensitive (/efficient)
20
Rank tests
2
Dichotomisation (landmark analysis)
22
Original
Score=1 if surviving
2.5 years
•
General rule: Dichotomisation loose power
•
Often: Very large power loss
•
Test statistic: Proportion surviving > y years
•
Fisher’s exact test, or e.g. normal approximation to Binomial dist
Rank test: Wilcoxon-Mann-Whitney
23
Original
Rank scores
•
Robust test
•
Asymptotic Relative Efficiency is 3/
=95% vs Z-test if Normal assuption is true
•
p=1.0%
Normal scores
24
Original
Normal scores
•
Robust
•
The worst and best responses get higher importance than in Wilcoxon
•
Asymptotic Relative Efficiency is 100% vs Z-test if Normal assumption is true
Log-rank test
3
Logrank test
26
Logrank test: Relation between # at risk & earlier deaths
27
Logrank test: Finding the scores
28
Logrank scores
(translated)
29
Original
Logrank scores
•
De-emphasising early deaths
•
Very high emphasis on the longest survivors
•
One reason that logrank is ”never” used when there is no censoring
•
Less extreme when long life times are censored
Hazard ratios
Logrank is the best rank-preserving test IF the hazard
ratio is constant over time
It is valid even if HR(t) is varying
•
That is, Type 1 Error control is guaranteed
But the power is not guaranteed
Should we (ever) believe in proportional hazards?
•
Clinical models
•
As with the t-test etc., the logrank test will serve well in
many cases … if reality isn’t too far from assumptions
30
Weighted
log-rank tests
4
Weighted logrank tests
32
Can we use
any
scores?
33
Are any weights OK?
34
Weighted logrank test & Scores
35
Weighted logrank scores if first 20 weights are zero
36
Original
WLRT scores
BAD!
Fleming-Harrington(0,1) scores
37
Original
FH(0,1) scores
BAD!
38
FH(0,1) and Max Combo
do not control
under H0: Survival is never better for New than Control
(but
is controlled if survival is identical for all t)
In fact, Type 1 Error
100% if N
infinity
How to defend a
test that thinks
early deaths
are better?
39
Lines of defense (1)
”We only test the null hypothesis of exactly equal survival
curves, for all times”
•
OK, so you prove that IO is not the same as chemo!??
•
Don’t you think regulators would like to see proof of any
positive effect?
”By looking at the Kaplan-Meier curves, you’ll obviously see
that the new drug is better after some time”
•
Hypothesis tests are there to avoid misunderstanding
noisy data
•
Take a look at the following example:
40
1-sided vs 2-sided test
•
It doesn’t matter … in the school book example
•
It makes all the difference in reality
•
A new drug should be
demonstrated to be better,
not just ”different”
from standard-of-care
41
Lines of defense (2)
”By looking at the Kaplan-Meier curves, you’ll obviously see
that the new drug is better after some time”
•
Hypothesis tests are there to avoid misunderstanding
noisy data
•
Take a look at the following example:
42
Weighted logrank may be severely misleading
T
R
U
E
O
B
S
E
R
V
E
D
E
x
p
e
r
i
m
e
n
t
a
l
i
s
a
l
w
a
y
s
w
o
r
s
e
Is it always easy to ”see” which drug is best? NO!
82.9% has more than
6 months improvement
in median
•
WLRT corresponds to an estimate of HR.
When Z
w
>1.96, always HR
est
<1
•
When Z
w
>1.96,
observed
median is often improved
(while
true
median is
worse)
An adjuvant trial example
Adjuvant
setting. We try to prolong the lives
of the non-cured (but we don’t know who is
cured or not).
•
2 arms with 200 patients each
•
70% cure rate on both treatments
•
Given non-cure, life span is exponentially
distributed with
•
Expected life time being 1 year on new
treatment, 2 years on placebo. (That is,
the
treatment is killing off patients much
faster
.)
Type I error ~30% (nominal 2.5%)
With 1000 per arm, type I error ~90%
Lines of defense (3)
”Do you have a better proposal than MaxCombo?”
46
Longer life is always better
47
Original
Modestly weighted logrank test scores
48
Original
Modestly scores
•
Constant scores when no efficacy
•
Cf. Landmark analysis
•
Logrank scores thereafter
•
as logrank is optimal if HR are constant
•
Even better with cutoff somewhat earlier
The best we can do:
Constant scores when we
don’t think we have a benefit
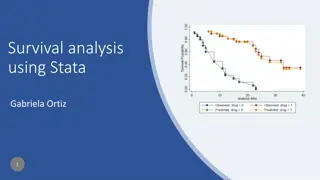
Summary Z-scores for OS
Modestly test is better than logrank test in all IO examples
Not very sensitive in cutoff time for equal scores. Here 12 months.
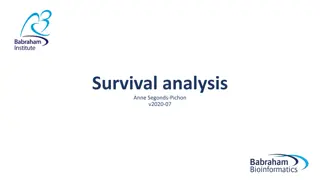
Censoring
50
Conclusions
5
Recommendations when expecting efficacy delay
52
•
Consider using the ”Modestly” test
•
Clearly better power than standard logrank
•
S
trong a control (unlike Max Combo, many weighted logrank tests)
•
A
dd a variety of efficacy estimates
•
Kaplan-Meier curves (always!), directly corresponding to …
•
… Landmark rates, Quantile estimates (median not always useful)
•
(Truncated) mean survival makes clinical sense (but test is inefficient)
•
Modestly test corresponds to an HR estimate …
•
… but all average estimates of HR can be misleading
•
Estimated HR(t) should be interpreted with care
References
•
Magirr & Burman (2019). ”Modestly weighted logrank tests.”
Statistics in Medicine
38:3782-3790.
•
Gregson, Sharples, Stone, Burman, Öhrn & Pocock (2019). "Nonproportional hazards for
time-to-event outcomes in clinical trials."
J Am Coll Cardiol
74:2102.
•
Bartlett, Morris, Stensrud, Daniel, Vansteelandt & Burman (2020). “The Hazards of
Period Specific and Weighted Hazard Ratios.”
Statistics in Biopharmaceutical Research
12:518-519.
•
Magirr (2020). “Non‐proportional hazards in immuno‐oncology: Is an old perspective
needed?” Pharmaceutical Statistics (early view).
•
Magirr & Jimenez (2021). “Designing group sequential clinical trials when a delayed
effect is anticipated: A practical guidance.”
https://arxiv.org/abs/2102.05535
•
Leton, Zuluaga (2001). Equivalence between score and weighted tests for survival
curves.
Commun Stat Theory Methods
30:591-608.
54
Weighted log-rank tests and alternative methods in survival trials are discussed by Carl-Fredrik Burman, PhD, focusing on the basics, special considerations in survival analysis, clinical trial objectives, distributional assumptions, and different bases for inference.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Inference in survival trials: Weighted log-rank tests and some alternatives Carl-Fredrik Burman, PhD, Assoc.Prof. Statistical Innovation, Data Science & AI AstraZeneca R&D, Gothenburg 29 April, 2021
Thanks to Dominic Magirr for great collaboration 2
1 Back to Basics
Whats special with Survival Analysis? STANDARD STATISTICAL PROBLEMS Example 1: Two samples, normal distributions Exampe 2: Zero-one responses SURVIVAL ANALYSIS 1. Responses are positive May use transformation (e.g. log) 2. We don t have time to follow all patients (censoring) Missing data, with known structure 3. Competing risks, Treatment switching 4
PhD advise: Don t complicate things before understanding the basics 5
Clinical trial, comparing New treatment, X, versus Standard of Care, C What is (really) the main efficacy objective? To compare X and C To show a (=any) difference To show X has an efficacy benefit Hypothesis testing Null hypothesis Test statistic (pre-specified) Null distribution Statistical inference 6
Distributional assumptions Does the validity of the statistical analysis require that assumptions are correct? Do we need uncertain assumptions to guarantee Type 1 Error control? OR Will assumptions only influence the power (sponsor s risk)? 7
Two different bases for inference showing treatment benefit Distribution-based E.g. ANCOVA, t-test has exactly correct Type 1 Error (only) if normal distributions + same residual variance Randomisation-based Relies of nothing else than randomisation of patients Any reasonable pre-specified test statistic; can handle covariates In principle, randomisation test much more robust In practise, distribution-based tests are often (but not always) good enough to control Type 1 Error even if assumptions are not fully correct. Preferable with approximate formula than simulated p-value? 8
Example dataset* n=37 per arm Group A: New treatment Group B: Control Survival time in days Mice data No censoring 9* Loosely based on Xie et al (2017). Nature Communications 8:155.
Randomisation test (permutation test) H0: Time does not depend on arm That is, the highest observed time could equally well have been on A as B. 1 ? ? ??? Test statistic ? = That is, average observed life time in group A Same for next highest etc. We can generate a null distribution by keeping all observation fixed but re-randomize and repeat e.g. one million times. Observed ????= 814.4 (whereas average in arm B was 919.0) 13
Randomisation test We can generate a null distribution by keeping all observation fixed but re-randomize and repeat e.g. one million times. Observed ????= 814.4 (whereas average in arm B was 919.0) p-value = 0.6% ????= 814.4 All p-values 1-sided, as we want to show B better than A 14
Distribution-based inference: Z-test Assumptions N-distribution has poor fit to data I.i.d. Normal in each arm Same known variance (taken equal to estimate) p-value = 1.0% P-value happens to be higher than prand=0.6% Asymptotic Relative Efficiency of randomisation test vs Z-test is exactly 100% if Z-test assumptions are OK Z-test is approximately correct in many situations. Problems if few observations have lrge impact on variance: outliers, heavy tails, (NB! All p-values are one-sided as we want to show B is better than A.) 15
T-test Assumptions I.i.d. Normal in each arm (Questionable assumption) Same variance, estimated from data pT=1.1% Cf. pZ=1.0%, prand=0.6% T-test reflects change in null distribution due to random estimate of SD Asymptotically t-test = Z-test 16
Lognormal test Original Log of data With positive data, lognormal is sometimes better than normal Not in this example Recall: Test should be pre-specified Log scale is dangerous if some life span is close to zero NB! Tests are scale-and location-invariant 17
Transformations Log transform, xi=log(ti) Any monotone function f gives valid test based on xi=f(ti) Randomisation test or if distributional assumptions are appropriate t-test, ANCOVA etc based on transformed observations xi 18
The estimand framework can help us think, structure discussions But there are several contradicting dimensions The best test to show treatment benefit may not directly correspond to an easily understandable, clinically attractive estimand Average Hazard Ratio may not be the most natural estimand (especially if HR varies greatly over time). Still, that in itself may not disqualify using a (perhaps weighted) logrank test Tradeoff: Transformations can be useful but Don t make it unnecessarily complicated Estimands 19
Simple and meaningful What is clinically (most) important? What is easy? EXAMPLES Mean survival Proportion cured. Proxy: 5-year survival? But easy and important may not mean statistically sensitive (/efficient) 20
2 Rank tests
Dichotomisation (landmark analysis) Original Score=1 if surviving 2.5 years General rule: Dichotomisation loose power Often: Very large power loss Test statistic: Proportion surviving > y years Fisher s exact test, or e.g. normal approximation to Binomial dist 22
Rank test: Wilcoxon-Mann-Whitney Original Rank scores Robust test Asymptotic Relative Efficiency is 3/ =95% vs Z-test if Normal assuption is true p=1.0% 23
Normal scores Original Normal scores Robust The worst and best responses get higher importance than in Wilcoxon Asymptotic Relative Efficiency is 100% vs Z-test if Normal assumption is true 24
3 Log-rank test
Logrank test The logrank test is a non-parametric score test (like Wilcoxon, Normal Scores, etc.) Can be formulated in different ways. The test statistic may be defined as ?? ? = ?? ??+ ?? ? Where ??= 1 if the k:th death is on Arm A, and ??= 0if it s on arm B; ?? and ??are the numbers at risk in arm A and B, respectively, just before the k: death. We start with ?1and ?1as the sample sizes per arm. Note that ?2= ?1 ?1, that is the number at risk in arm A is unchanged if 1st death on B; it is reduced by one if 1st death in arm A With this idea, the logrank test statistics can be rewritten as a sum of scores 26
Logrank test: Relation between # at risk & earlier deaths ?? ? = ?? ??+ ?? ? Where ??= 1 if the k:th death is on Arm A ?? and ??are the numbers at risk in arm A and B. Total # at risk is decreased by 1 for every death: ??+ ??= ? + ? (? 1) # at risk in Arm A is decreased by 1 for every time the death indicator is 1: ??= ? ?1 ?? 1 Inserting these two expressions, we can re-write the logrank test statistic: ? ? ?1 ?+? 1+ ?3 ? ?1 ?2 ?+? 2+ + ??+? ? ?1 ?2 ??+? 1 ? = ?1 ?+?+ ?2 ?+? (?+? 1) 27
Logrank test: Finding the scores ? ? ?1 ? + ? 1 + ?3 ? ?1 ?2 ? + ? 2 + + ??+? ? ?1 ?2 ??+? 1 ? + ? (? + ? 1) ? = ?1 + ?2 ? + ? Note that e.g. ?1 occurs in several places: Partly as a direct contribution to the 1st term, corresponding to the 1st death But also modifying the # at risk in Arm A for all future events We can collect all terms involving ?1, and all terms for ?2, ?3, etc. We get ?+? 1 ? = ???? ? + ? (? 1) ? ?=1 where the scores are ?+? 1 1 ??= 1 + ? + ? ? ?=? 28
Logrank scores (translated) Original Logrank scores De-emphasising early deaths Very high emphasis on the longest survivors One reason that logrank is never used when there is no censoring Less extreme when long life times are censored 29
Logrank is the best rank-preserving test IF the hazard ratio is constant over time It is valid even if HR(t) is varying That is, Type 1 Error control is guaranteed But the power is not guaranteed Should we (ever) believe in proportional hazards? Clinical models As with the t-test etc., the logrank test will serve well in many cases if reality isn t too far from assumptions Hazard ratios 30
4 Weighted log-rank tests
Weighted logrank tests ?? Logrank test ? = 1? ??+?? ?? Weighted logrank test ??= ?? 1? ??+?? Idea: Prespecify lower weights when drug efficacy is low (or negative) 32
Can we use any scores? 33
Are any weights OK? Could we take ??= 0 for k=1, ,K? No! We would then ignore all the first K deaths. A drug killing frail patients early could then look good! ?? ??= ?? 1? ??+ ?? 34
Weighted logrank test & Scores ?? ? = ?? ?? ??+ ?? ? ? ? + ?1 ? + ? 1 + +??+? ??+? ? + ?1+ ?2+ + ??+? 1 ? + ? (? + ? 1) ? = ?1 ?1 +?2 ?2 ? + ? We can collect all terms involving ?1, and all terms for ?2, ?3, etc. We get ?+? ?? ? = ???? ? + ? (? 1) ? ?=1 where the scores are ?+? ?? ??= ??+ ? + ? (? 1) ?=?+1 35
Weighted logrank scores if first 20 weights are zero Original WLRT scores BAD! Weighted logrank test with ??= 0 ??= 1 You get bonus points if the patient dies early Do not accept decreasing weights! if ? 20 otherwise (Alternatively, if ? ?) 36
Fleming-Harrington(0,1) scores Original FH(0,1) scores BAD! Weighted logrank test: Fleming-Harrington(0,1) ?1= 0 ?? linearly increasing 37
FH(0,1) and Max Combo do not control under H0: Survival is never better for New than Control (but is controlled if survival is identical for all t) In fact, Type 1 Error 100% if N infinity 38
How to defend a test that thinks early deaths are better? 39
Lines of defense (1) We only test the null hypothesis of exactly equal survival curves, for all times OK, so you prove that IO is not the same as chemo!?? Don t you think regulators would like to see proof of any positive effect? By looking at the Kaplan-Meier curves, you ll obviously see that the new drug is better after some time Hypothesis tests are there to avoid misunderstanding noisy data Take a look at the following example: 40
1-sided vs 2-sided test It doesn t matter in the school book example It makes all the difference in reality A new drug should be demonstrated to be better, not just different from standard-of-care 41
Lines of defense (2) By looking at the Kaplan-Meier curves, you ll obviously see that the new drug is better after some time Hypothesis tests are there to avoid misunderstanding noisy data Take a look at the following example: 42
Weighted logrank may be severely misleading TRUE OBSERVED Experimental is always worse Test Logrank FH(0,1) Z-score 1.45 2.70 p-value 14.8% 0.7%
Is it always easy to see which drug is best? NO! WLRT corresponds to an estimate of HR. When Zw>1.96, always HRest<1 When Zw>1.96, observed median is often improved (while true median is worse) 82.9% has more than 6 months improvement in median
An adjuvant trial example Adjuvant setting. We try to prolong the lives of the non-cured (but we don t know who is cured or not). 2 arms with 200 patients each 70% cure rate on both treatments Given non-cure, life span is exponentially distributed with Expected life time being 1 year on new treatment, 2 years on placebo. (That is, the treatment is killing off patients much faster.) Type I error ~30% (nominal 2.5%) With 1000 per arm, type I error ~90%
Lines of defense (3) Do you have a better proposal than MaxCombo? 46
Longer life is always better Original May transform life times Based on ??or its rank but the transformation has to be monotonely increasing 47
Modestly weighted logrank test scores Modestly scores Original The best we can do: Constant scores when we don t think we have a benefit Constant scores when no efficacy Cf. Landmark analysis Logrank scores thereafter as logrank is optimal if HR are constant Even better with cutoff somewhat earlier 48
Summary Z-scores for OS Logrank 5.11 2.35 2.64 2.82 2.81 2.94 3.72 2.89 2.49 3.77 2.20 1.14 3.07 4.35 2.13 Modestly 5.48 2.88 3.01 3.22 3.41 3.39 3.84 3.71 2.50 3.89 2.83 2.02 3.24 4.70 2.43 Modestly test is better than logrank test in all IO examples Not very sensitive in cutoff time for equal scores. Here 12 months.
Dedicated survival analysis tests include how to handle censoring when data are analysed before some patients have had events The Modestly Weighted Logrank Test handles censoring just like the unweighted logrank test Other tests may be adapted to survival settings Parametric tests may e.g. use a likelihood function of the form ? = i has event?(??) i censored?(??) Censoring 50










")








")





")






 scores")
 and Max Combo")

")

")



")