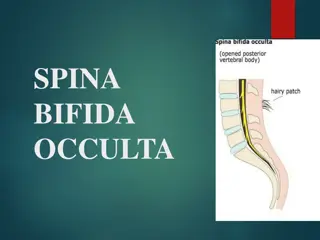
Urticaria and Angioedema: Symptoms, Causes, and Treatment
Urticaria, commonly known as hives, and angioedema are skin conditions characterized by red, raised welts and swelling. Urticaria typically lasts less than 24 hours and can occur anywhere on the body, while angioedema involves episodic swelling of subcutaneous or submucosal tissues. Causes include infections, allergic reactions, physical stimuli, and systemic diseases. Antibiotic allergies in children may be overdiagnosed. Sinusitis can be a common cause of chronic hives. Treatment may involve antihistamines, corticosteroids, and identifying triggers through allergy testing.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Urticaria and Angioedema Jim Harris, MD Allergy and Immunology South Bend Clinic
Definition Urticaria (hives, welts, whelps ) Area of redness and swelling of various sizes, with flare, raised , +/- central pallor Itching (pruritis) Time course <24 hrs, skin returns to normal Can occur anywhere on body Angioedema episodic submucosal or subcutaneous swelling Skin normal color Affects extremities- hands, feet, face, genitals Lasts hours to several days Painful, numb, or tingling, rather than itching Acute urticaria - < six weeks duration Chronic spontaneous urticaria-AKA chronic idiopathic urticaria Greater than 6 weeks duration 50% hives only 40% hives and angioedema 10% mostly angioedema
Causes Idiopathic- 90% of chronic cases Infections- most acute cases IgE mediated allergic reactions Direct mast cell activation Nonsteroidal anti-inflammatories (NSAID s) Physical stimuli Systemic Diseases
Causes Infections Viral, parasitic, bacterial; antibiotics Up to 80% in pediatrics Study: 88 peds seen in ER w/ infection, on B-lactam antibiotics (penicillins/cephalosporins) and rash, 47/88 hives; on later challenge with same antibiotic, only 4/88 reacted Conclusion: allergy to antibiotics overdiagnosed in children
Infection Sinusitis; acute and chronic Most common identifiable cause of chronic hives in children Can be subtle Xrays can be helpful; esp CT Hives may persist even after treatment Often need abx for 2-4 weeks, even surgery, to clear
IgE mediated reactions Medications- antibiotics, etc. Stinging insects Foods and food additives Latex Contact with allergens Transfusions
IgE mediated Medications Virtually all, but especially antibiotics Penicillins and cephalosporins most common; may be labeled for life! 98% of PEN reactions resolve over 10 years Skin testing confirms, even w/ hx anaphylaxis, that allergy resolved May further confirm with oral challenge; single dose vs 10d course Cost effective to R/O penicillin allergy, especially pre surg and IV abx
IgE- Foods Usually within 30 of ingestion Can cause chronic sxs Children: milk, egg, peanut, tree nuts, seeds; many resolve Adults: shellfish, peanut, tree nuts; milk, egg Food additives: Yellow dye #5 (tartrazine) Red dye #4 and #40- ADHD in kids
Direct Mast Cell Activation Cause histamine release Narcotics- codeine, morphine Muscle relaxants- perioperative Vancomycin- Red man syndrome Certain foods- tomatoes, strawberries Radiocontrast media- can block with meds
Physical Stimuli Cold or heat induced Vibration Pressure Exercise- 2 types: Cholinergic urticaria Exercise induced anaphylaxis Solar (vs polymorphous light eruption) Aquagenic- contact with water! Stress?
Dermatographism AKA Dermographism Induced by stroking the skin Often have chronic itch even if no hives Differential: Dry skin Neurodermatitis (anxiety)
Systemic Causes Infections Sinusitis, prostatitis Hepatitis Autoimmune- lupus, RA Renal disease Cancer- lymphoma, myeloma Thyroid disease Hormonal- often cyclical Mast Cell Disorders
Mast Cell Disorders Mastocytosis- Abnormal number of mast cells Mast Cell Activation Syndrome- recent phenomena- 2007 Normal cells, abnl histamine release Hives, usually chronic Chronic rhinitis Autonomic dysfunction Irritable bowel, cystitis Headaches, sleep dysfunction Fibromyalgia Ehlers-Danlos/ hyperflexible Anaphylaxis
Evaluation History- events at or before onset May be complex and detailed Physical exam be sure they have hives! Sinuses, HSM, nodes Tests- limited, based on hx Systemic: CBC, ESR, CRP, CMP, TSH; ANA, RA Tryptase, +/- 24 hr urine studies Xray- chest (lymphoma), sinus Foods: for IgE reactions only Skin tests; most sensitive Blood tests; more expensive, less sensitive
Skin Biopsy ? When? Lesions last >24 hrs Painful not pruritic Respond only to steroids What? Often non-specific Eos, neutrophils, lymphocytes Immuno tests for vasculitis; deposition of complement and antibodies Best done by dermatology
Treatment Antihistamines H1 antagonists Second generation preferred- Allegra, Zyrtec (to 4/d) at least BID First generation- more sedating, but may be more effective; hydroxyzine up to 100 bid Benedryl- most sedating, short half life H2; ranitidine out, famotidine first choice, 20 bid; less effective Leukotriene antagonists Montelukast (Singulair); short half life though 1x/d Zafirlukast (Accolate); dosing bid
Treatment Prednisone/ systemic steroids Do not block mast cell degranulation, but Do reduce inflammatory mediators Many ways to dose Cyclosporin/ Dapsone- H pylori? Thyroid antibodies? Diet- no change, except MCAS Biologics Xolair (omalizumab) Others pending
Xolair (omalizumab) Refractory hives (also asthma) Monoclonal antibody Binds to free IgE, not IgE bound to mast cells Injections 150 or 300 mg every 2- 4 weeks; well tolerated 0.1% risk of anaphylaxis; Epipen. In 12 week study 44% complete resolution of hives 66% reduction in itching Cancer Risk? Minimal
Angioedema Less Common Rule out hereditary angioedema C1 esterase deficiency If tests (+), many new drugs If tests (-), treatment same as hives; preventive antihistamines, but steroids first line therapy Workup and evaluation same
Questions? Thank you for your attention Thanks to Beacon and Jenai Happy Holidays!!!




















")