Understanding Acute Otitis Media and Otitis Media with Effusion
Learn to diagnose and treat acute suppurative otitis media and otitis media with effusion, understand influencing factors for recurrent cases, differentiate between categories, specify predisposing factors, and recognize responsible microorganisms. Explore bacteriology, clinical features, and treatment options for these ear conditions.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
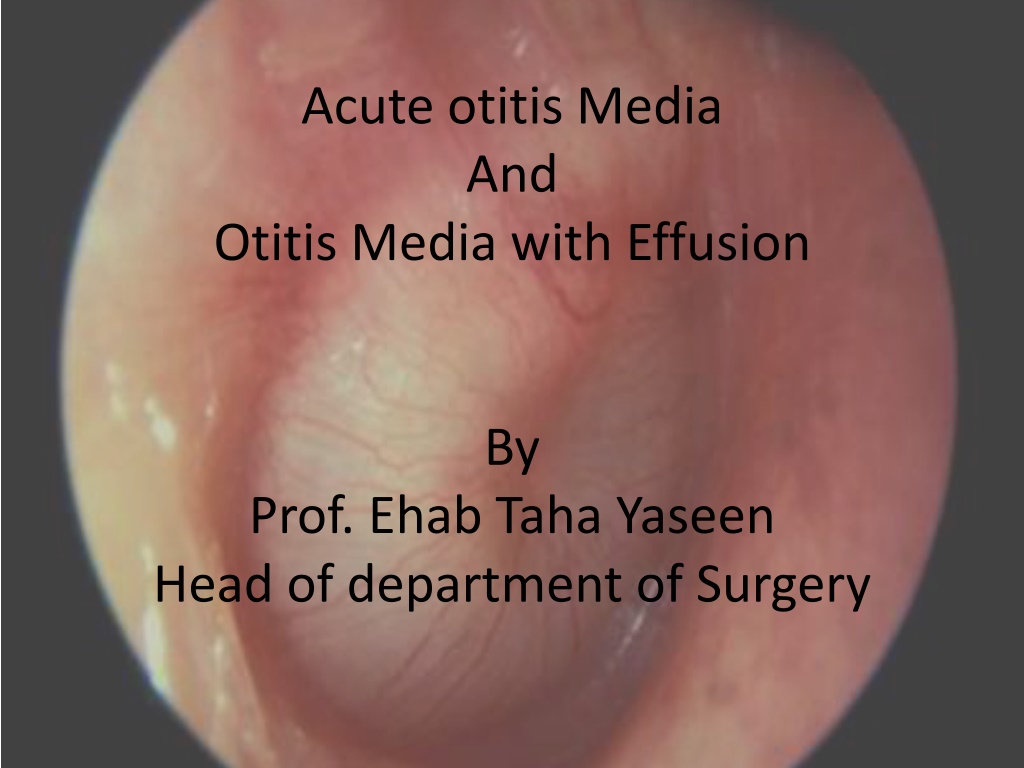
Acute otitis Media And Otitis Media with Effusion By Prof. Ehab Taha Yaseen Head of department of Surgery
Objectives 1. Will able to diagnose and treat both acute suppurative otitis media and otitis media with effusion 2. To know the influencing factors for recurrent acute otitis media 3. To know how to differentiate between these categories 4. To specify their predisposing factors 5. To recognize the responsible microorganisms
Acute otitis media Definition: Collection of purulent fluid in the middle ear cleft for less than 3 weeks. Define the middle ear cleft ((Home work)) Sources of infection: 1. Upper airway Slide 11, Slide 12 2. Exanthemas 3. Perforation of the tympanic membraneSlide 13
Bacteriology Haemolytic streptococcus, strep pneumonia, Haemophilus influenzae and Branhamella cattaralis. Pathology 1 - Tubal occlusion 2 - Engorgement and edema of the lining 3 - Exudation, serous then become purulent. This fluid results in bulging of the tympanic membrane which may cause rupture of the tympanic membrane by pressure necrosis usually posteroinferiorly. Slide 14
Clinical features: Phase I: Acute tubal obstruction (acute salpingitis) Fullness in the ear with conductive deafness. Phase II: Acute infection of the tympanic cavity (acute tympanitis) -- Before perforation: deafness increases, bubbling sounds are heared, otalgia and general symptoms especially seen in children and present as fever and malaise. On examination by otoscope: there are dilated vessels around the handle of the malleus and periphery of the tympanic membrane. This increases till the whole membrane is red, lusterless and bulging. -- After perforation: Otorrhea which may be serous, bloodstained, mucopurulent or purulent. The pain and tenderness are relieved immediately. Phase III: Retention of pus in the mastoid (acute mastoiditis rarely seen today) pain and tenderness over the mastoid region with edema of the posterosuperior wall of the deep meatus (a sign called sagging of meatal wall) with increase in the general symptoms. DD* ((Home work))
Treatment: Symptomatic: rest, sedation, analgesia and local heat. Medical: - Antibiotics amoxicillin, amoxicillin-calvulonic acid, cephalosporin (2ndand 3rdgeneration), macrolides as azithromycin, and clarithromycin - Nasal vasoconstrictor (xylometazolin drops, oral pesudoephedrin preparations) - Local treatment: - Before perforation of the TM myringotomy!! -When there is perforation Surgical: - Myringotomy {site}
Recurrent Acute Otitis Media Definition: is recurrent acute otitis media (5-6 times per year or 3-4 times per 6 months) and in between there is complete resolution of symptoms and signs Predisposing factor: Anatomical characteristics of the Eustachian tube Bottle fed baby vs. breast fed Parental smoking Low socioeconomic Crowded homes Poor nutrition Day care attendance Low immunity Nasal and postnasal problems (adenoid, allergy, polyps etc ) Perforated tympanic membrane
Non-Suppurative Otitis Media (Otitis Media with Effusion)
Definition It is a clinical condition that is characterized by the presence of non- purulent fluid in the middle ear cleft. Acute vs. Chronic (duration, type of fluid) Aetiology 1. Obstruction of the Eustachian tube 2. Unresolved acute suppurative Otitis media. 3. Viral Otitis media 4. Allergy as hay fever 5. Cleft palate and its repair.
Clinical Features - Conductive deafness, - Otalgia - Otoscopic findings: Dull and retracted TM Handle of the malleus is prominent, foreshortened and more horizontal. Slide 16 The color of the TM is pale yellow, sometime grey or even blue. Sometime fluid level (hair line) or air bubbles are seen. The fluid is usually clear, yellow, serous and sterile (no bacteria or inactive bacteria).
Diagnosis History and examination PTA shows conductive deafness. Slide 21 Tympanometry (acoustic impedance measurements) show reduction in compliance and negative middle ear pressure). ((Home work))
Treatment Medical treatment Nasal decongestant Antihistamines e.g. triprolidine and pseudoephedrine Oral antibiotics: amoxicillin-calvulonic acid Duration of treatment for up to one month. Surgical treatment: indicated when there is failure of medical treatment and may include Myringotomy to restart ventilation of the middle ear. Slide 18 Myringotomy and grommet Surgery for the cause like adenoidectomy. END
F:\Fifth year\ENT instruments\tests-hearing-audiogram-cond-loss-l.gif