Syphilis: Causes, Symptoms, and Treatment
 undefined
undefined

S
y
p
h
i
l
i
s


Causal
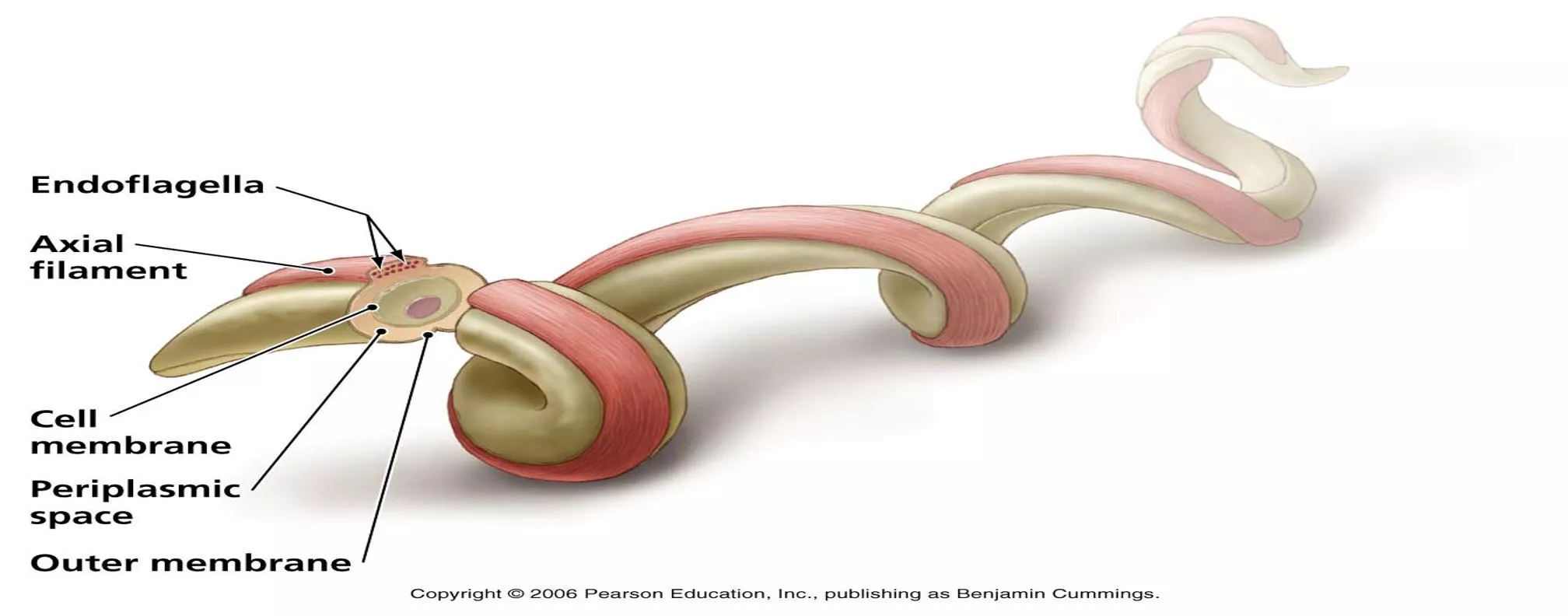
agent-Treponema pallidum
Gram- negative, spirochete with fine spirals and pointed or round ends.
~ 10 micrometers long and0.1-0.2 micrometers wide.
Not been successfully cultivated in artificial media.
T.pallidum
- endemic syphilis
T.petenue- Yaws
T.carateum- Pinta
Discovered by Schaudinn and Hoffman in 1905 in chancres and lymph nodes of syphilitic
patients.
T.pallidum
cannot be seen under the light microscope
in wet films but can be made out by negative staining
with india ink
It can be stained by silver impregnation methods.
It is possible to maintain
Treponema pallidum
in motile
and virulent form for 10-12 days in complex media
under anaerobic conditions
Virulent
T.pallidum
- maintained in serial testicular
passage in rabbits.
Nichol’s strain-isolated in 1912 is still being
propagated.
Reiter strain- non-pathogenic treponeme, widely
used as antigen in group specific tests for syphilis
diagnosis.
Treponemal infection induces atleast 3 types of
antibodies-
Reagin Antibody- used in standard or non specific test
for syphilis, in which Cardiolipin, a lipid hapten
extracted from beef heart is used as the antigen.
Group specific antigen
Species specific antigen- polysacharide in nature. The
antibodies to this demonstrated by the specific
T.
pallidum
tests that are positive only in the sera of
patients infected with pathogenic treponemes.
Natural infection with T. pallidum occurs only in human
beings.
Monkeys, Chimpanzees, Rabbits- experimental models.
S
y
p
h
i
l
i
s
-
P
a
t
h
o
g
e
n
e
s
i
s
Venereal syphilis is acquired by sexual contact whereas
endemic syphilis is transmitted non-venereally.
Entry through minute abrasions on the mucosa and skin.
Infectivity maximun during first two years of the disease.
Transplacental transmission can take place at any stage of
pregnancy.
Lesions of congenital syphilis develop only after the fourth
month of gestation.
As few as 60 treponemes are capable of infecting 50% of
human volunteers.
Generation time- 30-33 hours.
Incubation period- 10-90 days.
Clinical manifestations fall into 3 stages-
Primary syphilis, Secondary syphilis, Tertiary syphilis
P
R
I
M
A
R
Y
S
Y
P
H
I
L
I
S
P
r
i
m
a
r
y
l
e
s
i
o
n
d
e
v
e
l
o
p
s
a
t
s
i
t
e
o
f
c
o
n
t
a
c
t
/
i
n
o
c
u
l
a
t
i
o
n
.
C
l
a
s
s
i
c
a
l
l
y
:
s
i
n
g
l
e
,
p
a
i
n
l
e
s
s
,
c
l
e
a
n
-
b
a
s
e
d
,
i
n
d
u
r
a
t
e
d
u
l
c
e
r
,
w
i
t
h
f
i
r
m
,
r
a
i
s
e
d
b
o
r
d
e
r
s
c
a
l
l
e
d
c
h
a
n
c
r
e
.
M
o
s
t
l
y
a
n
o
g
e
n
i
t
a
l
,
b
u
t
m
a
y
o
c
c
u
r
a
t
a
n
y
s
i
t
e
.
C
o
v
e
r
e
d
b
y
a
t
h
i
c
k
,
g
l
a
i
r
y
e
x
u
d
a
t
e
r
i
c
h
i
n
s
p
i
r
o
c
h
e
t
s
.
R
e
g
i
o
n
a
l
l
y
m
p
h
n
o
d
e
s
a
r
e
s
w
o
l
l
e
n
a
n
d
d
i
s
c
r
e
t
e
.
,
r
u
b
b
e
r
y
a
n
d
n
o
n
-
t
e
n
d
e
r
.
V
e
r
y
i
n
f
e
c
t
i
o
u
s
.
M
a
y
b
e
d
a
r
k
f
i
e
l
d
p
o
s
i
t
i
v
e
b
u
t
s
e
r
o
l
o
g
i
c
a
l
l
y
n
e
g
a
t
i
v
e
.
U
n
t
r
e
a
t
e
d
,
h
e
a
l
s
i
n
1
0
-
4
0
d
a
y
s
,
l
e
a
v
i
n
g
a
f
a
i
n
t
s
c
a
r
.
S
E
C
O
N
D
A
R
Y
S
Y
P
H
I
L
I
S
S
e
e
n
6
w
e
e
k
s
t
o
6
m
o
n
t
h
s
a
f
t
e
r
p
r
i
m
a
r
y
c
h
a
n
c
r
e
U
s
u
a
l
l
y
w
i
t
h
a
d
i
f
f
u
s
e
n
o
n
-
p
r
u
r
i
t
i
c
,
i
n
d
u
r
a
t
e
d
r
a
s
h
,
i
n
c
l
u
d
i
n
g
p
a
l
m
s
&
s
o
l
e
s
.
M
a
y
a
l
s
o
c
a
u
s
e
:
F
e
v
e
r
,
m
a
l
a
i
s
e
,
h
e
a
d
a
c
h
e
,
s
o
r
e
t
h
r
o
a
t
,
m
y
a
l
g
i
a
,
a
r
t
h
r
a
l
g
i
a
,
g
e
n
e
r
a
l
i
z
e
d
l
y
m
p
h
a
d
e
n
o
p
a
t
h
y
H
e
p
a
t
i
t
i
s
(
1
0
%
)
T
h
e
r
e
m
a
y
a
l
s
o
b
e
o
p
h
t
h
a
l
m
i
c
a
n
d
m
e
n
i
n
g
e
a
l
d
e
v
e
l
o
p
m
e
n
t
.
H
i
g
h
l
y
v
a
r
i
a
b
l
e
i
n
i
n
t
e
n
s
i
t
y
,
d
i
s
t
r
i
b
u
t
i
o
n
a
n
d
h
e
a
l
i
n
g
.
U
n
d
e
r
g
o
s
p
o
n
t
a
n
e
o
u
s
h
e
a
l
i
n
g
,
b
u
t
i
n
s
o
m
e
i
n
s
t
a
n
c
e
s
t
a
k
e
s
a
s
l
o
n
g
a
s
4
-
5
y
e
a
r
s
.
T
h
e
s
k
i
n
r
a
s
h
:
Diffuse,
often with a superficial scale (papulosquamous).
May leave residual pigmentation or depigmentation.
C
o
n
d
y
l
o
m
a
t
a
L
a
t
a
:
Formed by coalescence of large, pale, flat-topped
papules.
Occur in warm, moist areas.
Highly infectious.
M
u
c
o
s
a
l
l
e
s
i
o
n
s
:
~ 30% of secondary syphilis patients develop mucous
patch (slightly raised, oval area covered by a grayish
white membrane, with a pink base that does not
bleed).
Highly infectious
L
A
T
E
S
Y
P
H
I
L
I
S
‘
T
e
r
t
i
a
r
y
S
y
p
h
i
l
i
s
’
D
i
a
g
n
o
s
i
s
i
n
l
a
t
e
n
t
p
h
a
s
e
–
o
n
l
y
t
h
r
o
u
g
h
s
e
r
o
l
o
g
y
I
s
t
h
e
d
e
s
t
r
u
c
t
i
v
e
s
t
a
g
e
o
f
t
h
e
d
i
s
e
a
s
e
.
L
e
s
i
o
n
s
d
e
v
e
l
o
p
i
n
s
k
i
n
,
b
o
n
e
,
&
v
i
s
c
e
r
a
l
o
r
g
a
n
s
(
a
n
y
o
r
g
a
n
)
.
C
o
n
t
a
i
n
f
e
w
s
p
i
r
o
c
h
e
t
e
s
.
T
h
e
m
a
i
n
t
y
p
e
s
a
r
e
:
C
h
r
o
n
i
c
g
r
a
n
u
l
o
m
a
t
o
u
s
(
g
u
m
m
a
t
o
u
s
)
o
r
g
u
m
m
a
s
C
a
r
d
i
o
v
a
s
c
u
l
a
r
N
e
u
r
o
s
y
p
h
i
l
i
s
C
a
n
b
e
c
r
i
p
p
l
i
n
g
a
n
d
l
i
f
e
t
h
r
e
a
t
e
n
i
n
g
B
l
i
n
d
n
e
s
s
,
d
e
a
f
n
e
s
s
,
d
e
f
o
r
m
i
t
y
,
l
a
c
k
o
f
c
o
o
r
d
i
n
a
t
i
o
n
,
p
a
r
a
l
y
s
i
s
,
d
e
m
e
n
t
i
a
m
a
y
o
c
c
u
r
.
I
t
i
s
u
s
u
a
l
l
y
v
e
r
y
s
l
o
w
l
y
p
r
o
g
r
e
s
s
i
n
g
.
L
a
t
e
s
y
p
h
i
l
i
s
i
s
n
o
n
i
n
f
e
c
t
i
o
u
s
.
D
i
a
g
n
o
s
i
s
Dark field Microscopy
T. pallidum
is identified by it slender spiral structure and
slow movement. Negative results do not exclude the
diagnosis of syphilis as a treponemal concentration of
104 per ml is required for positive result.
Direct Fluorescent Antibody (DFA)
Better and safer method.
Smears of exudate are fixed with acetone and DFA is
done by using fluorescent tagged anti-
T.pallidum
antiserum.
VDRL (venereal disease research laboratory) Test
1.
In the VDRL test the inactivated (heated just enough to inactivate
pathogen in it) serum is mixed with cardiolipin antigen on a special slide
and is rotated for four minutes.
2.
Cardiolipin forms visible clumps on combining with reagin antibody. The
reaction is read under a low power microscope.
3.
The VDRL test can be used for testing CSF also, but not plasma.
RPR test
RPR Test is a modification of the VDRL test and is known as Rapid
Plasma Reagin (RPR) Test.
1.
The RPR test uses the VDRL antigen containing fine carbon particles,
which make the result more clear and evident to the naked eye.
2.
RPR test can be done with unheated serum plasma but is not suitable for
testing CSF.
•
FTA Test
1.
The fluorescent treponemal antibody (FTA) test is an
indirect immunofluorescence test using as antigen,
smears prepared on slides with Nichol’s strain of
T.
Pallidum.
•
TPHA Test
1.
The
T. pallidum
hemagglutination Assay (TPHA) uses
tanned erythrocytes sensitised with a sonicated extract
of
T.pallidum
, as antigen.
E
p
i
d
e
m
i
o
l
o
g
y
Venereal syphilis is worldwide in distribution.
The disease has undergone much variation In its
natural history and clinical features since its discovery.
The advent of AIDS pandemic has had an impact on
syphilis. Syphilis increases the risk of both transmitting
and getting infected by HIV.
Concurrent infection with syphilis and HIV is common
and may lead to neurosyphilis.
P
r
o
p
h
y
l
a
x
i
s
Avoidance of sexual contact with an infected individual.
Use of physical barriers- condoms
Chemical- potassium permanganate
Antibiotics as prophylactic measure.
Penicillin as a prophylactic drug may suppress the
primary lesion without eliminating the infection.
No vaccines are available yet.
Congenital syphilis can be prevented by giving adequate
treatment to the mother before the fourth month of
gestation starts.
T
r
e
a
t
m
e
n
t
Penicillin is uniformly effective in syphilis. A uniform and
adequate dosage is important.
Early syphilis- 2.4 million units of benzathine penicillin G.
Late syphilis-
Benzathine
penicillin G 2.4 million units at
one week intervals x 3 doses
P
e
n
i
c
i
l
l
i
n
a
l
l
e
r
g
y
*
Doxycycline 100 mg orally twice daily x 28 days
or
Tetracycline 500 mg orally four times daily x 28days
Neurosyphilis- Ceftriaxone 2 gm daily IM/IV for 10-14
days.
Syphilis is a sexually transmitted infection caused by Treponema pallidum. This spirochete bacteria can lead to various stages of syphilis, including primary, secondary, and tertiary. The infection is primarily acquired through sexual contact but can also be transmitted non-venereally. Recognizing the symptoms and seeking prompt treatment is crucial to prevent complications. Diagnosis involves specific tests to detect antibodies, and treatment usually consists of antibiotics. Understanding the pathogenesis and clinical manifestations of syphilis is essential for effective management.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Causal agent-Treponema pallidum Gram- negative, spirochete with fine spirals and pointed or round ends. ~ 10 micrometers long and0.1-0.2 micrometers wide. Not been successfully cultivated in artificial media. T.pallidum- endemic syphilis T.petenue- Yaws T.carateum- Pinta Discovered by Schaudinn and Hoffman in 1905 in chancres and lymph nodes of syphilitic patients.
T.pallidum cannot be seen under the light microscope in wet films but can be made out by negative staining with india ink It can be stained by silver impregnation methods. It is possible to maintain Treponema pallidum in motile and virulent form for 10-12 days in complex media under anaerobic conditions Virulent T.pallidum- maintained in serial testicular passage in rabbits. Nichol s strain-isolated in 1912 is still being propagated. Reiter strain- non-pathogenic treponeme, widely used as antigen in group specific tests for syphilis diagnosis.
Treponemal infection induces atleast 3 types of antibodies- Reagin Antibody- used in standard or non specific test for syphilis, in which Cardiolipin, a lipid hapten extracted from beef heart is used as the antigen. Group specific antigen Species specific antigen- polysacharide in nature. The antibodies to this demonstrated by the specific T. pallidum tests that are positive only in the sera of patients infected with pathogenic treponemes. Natural infection with T. pallidum occurs only in human beings. Monkeys, Chimpanzees, Rabbits- experimental models.
Syphilis- Pathogenesis Venereal syphilis is acquired by sexual contact whereas endemic syphilis is transmitted non-venereally. Entry through minute abrasions on the mucosa and skin. Infectivity maximun during first two years of the disease. Transplacental transmission can take place at any stage of pregnancy. Lesions of congenital syphilis develop only after the fourth month of gestation. As few as 60 treponemes are capable of infecting 50% of human volunteers. Generation time- 30-33 hours. Incubation period- 10-90 days. Clinical manifestations fall into 3 stages- Primary syphilis, Secondary syphilis, Tertiary syphilis
PRIMARY SYPHILIS Primary lesion develops at site of contact/inoculation. Classically: single, painless, clean-based, indurated ulcer, with firm, raised borders called chancre. Mostly anogenital, but may occur at any site. Covered by a thick, glairy exudate rich in spirochets. Regional lymph nodes are swollen and discrete., rubbery and non-tender. Very infectious. May be darkfield positive but serologically negative. Untreated, heals in 10-40 days, leaving a faint scar.
SECONDARY SYPHILIS Seen 6 weeks to 6 months after primary chancre Usually with a diffuse non-pruritic, indurated rash, including palms & soles. May also cause: Fever, malaise, headache, sore throat, myalgia, arthralgia, generalized lymphadenopathy Hepatitis (10%) There may also be ophthalmic and meningeal development. Highly variable in intensity, distribution and healing. Undergo spontaneous healing, but in some instances takes as long as 4-5 years.
The skin rash: Diffuse, often with a superficial scale (papulosquamous). May leave residual pigmentation or depigmentation. Condylomata Lata: Formed by coalescence of large, pale, flat-topped papules. Occur in warm, moist areas. Highly infectious. Mucosal lesions: ~ 30% of secondary syphilis patients develop mucous patch (slightly raised, oval area covered by a grayish white membrane, with a pink base that does not bleed). Highly infectious
LATE SYPHILIS Tertiary Syphilis Diagnosis in latent phase only through serology Is the destructive stage of the disease. Lesions develop in skin, bone, & visceral organs (any organ). Contain few spirochetes. The main types are: Chronic granulomatous (gummatous) or gummas Cardiovascular Neurosyphilis Can be crippling and life threatening Blindness, deafness, deformity, lack of coordination, paralysis, dementia may occur. It is usually very slowly progressing. Late syphilis is noninfectious.
Diagnosis Dark field Microscopy T. pallidum is identified by it slender spiral structure and slow movement. Negative results do not exclude the diagnosis of syphilis as a treponemal concentration of 104 per ml is required for positive result. Direct Fluorescent Antibody (DFA) Better and safer method. Smears of exudate are fixed with acetone and DFA is done by using fluorescent tagged anti- T.pallidum antiserum.
VDRL (venereal disease research laboratory) Test In the VDRL test the inactivated (heated just enough to inactivate pathogen in it) serum is mixed with cardiolipin antigen on a special slide and is rotated for four minutes. Cardiolipin forms visible clumps on combining with reagin antibody. The reaction is read under a low power microscope. The VDRL test can be used for testing CSF also, but not plasma. RPR test RPR Test is a modification of the VDRL test and is known as Rapid Plasma Reagin (RPR) Test. The RPR test uses the VDRL antigen containing fine carbon particles, which make the result more clear and evident to the naked eye. RPR test can be done with unheated serum plasma but is not suitable for testing CSF. 1. 2. 3. 1. 2.
FTA Test The fluorescent treponemal antibody (FTA) test is an indirect immunofluorescence test using as antigen, smears prepared on slides with Nichol s strain of T. Pallidum. 1. TPHA Test The T. pallidum hemagglutination Assay (TPHA) uses tanned erythrocytes sensitised with a sonicated extract of T.pallidum, as antigen. 1.
Epidemiology Venereal syphilis is worldwide in distribution. The disease has undergone much variation In its natural history and clinical features since its discovery. The advent of AIDS pandemic has had an impact on syphilis. Syphilis increases the risk of both transmitting and getting infected by HIV. Concurrent infection with syphilis and HIV is common and may lead to neurosyphilis.
Prophylaxis Avoidance of sexual contact with an infected individual. Use of physical barriers- condoms Chemical- potassium permanganate Antibiotics as prophylactic measure. Penicillin as a prophylactic drug may suppress the primary lesion without eliminating the infection. No vaccines are available yet. Congenital syphilis can be prevented by giving adequate treatment to the mother before the fourth month of gestation starts.
Treatment Penicillin is uniformly effective in syphilis. A uniform and adequate dosage is important. Early syphilis- 2.4 million units of benzathine penicillin G. Late syphilis- Benzathine penicillin G 2.4 million units at one week intervals x 3 doses Penicillin allergy* Doxycycline 100 mg orally twice daily x 28 days Tetracycline 500 mg orally four times daily x 28days or Neurosyphilis- Ceftriaxone 2 gm daily IM/IV for 10-14 days.











 Test")