Mental Health Continuum and Stress Management Strategies
Explore the various aspects of mental illness as a continuum, including psychosis and depression, along with optimal stress management techniques. Learn about the positive and negative effects of stress, symptoms of psychosis, and strategies for maintaining mental well-being.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Mental Illness as a Continuum Psychosis confusion reigns Beliefs without fixed beliefs consumed by fixed ideas / evidence inflexible dysfunction/confusion Over-active speedy & pushy chaotic, volatile, Workaholic hard to relate to Manic depression negative high voltage destructive Poetic Personality Depression lovelessness withdrawn/ dropped persistent melancholy out/ hopelessness Social use reliance when stressed constant state of for anxiety or depressed & enjoyment AOD abuse master not slave intoxication/ dropped out
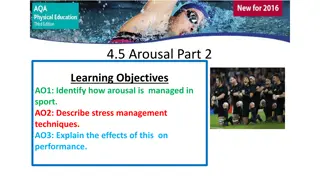
Optimal Stress Individual stress threshold and.. Biological and psychological vulnerability and.. Multiple stressors or triggers Optimal Distraction Inattention Attention Arousal
Stress The positive effects of stress include growth reprioritization of goals increased self-esteem expanded or strengthened networks The negative effects include, initially, heightened arousal, anxiety and psychosis withdrawal, apathy, depression and diminished sense of self-worth and self-efficacy The absence of meaningful stimulation can be stressful as well; too little stress can lead to boredom and anergia
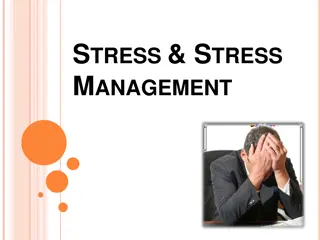
Psychosis -Psychoeducation Hallucinations Hearing voices or Hearing voices or seeing visions visions seeing Delusions False beliefs or False beliefs or marked suspicions of others suspicions of others marked Disorganized thinking Jumbled thoughts, Jumbled thoughts, difficulty concentrating concentrating difficulty Depression at the point of recovery Realisation Realisation of situation of situation 50% have only 1 episode 50% have only 1 episode Only 25% go on the chronic problems Only 25% go on the chronic problems Multiple episodes reduce the positive prognosis. Multiple episodes reduce the positive prognosis. F Florid symptoms are more associated with trauma lorid symptoms are more associated with trauma- - negative symptoms are more associated with chronic biological conditions. symptoms are more associated with chronic biological conditions. negative
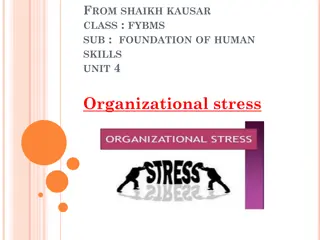
Be Bilingual Disturbed Disturbed Arousal and Attention Arousal and Attention Restless, can t concentrate , its too much , Too loud , its hard to sleep/ I can t sit still Thought Disorder/ Cognitive Thought Disorder/ Cognitive Disorganisation Disorganisation Confusion : scrambled newspaper Feeling overwhelmed : There s too much going on I can t read or concentrate My head is racing all the time or noisy Special ideas/knowledge stuck on something It feels like the world is depending on me I know what s going on Delusions Delusions Sensitive : I can taste and hear everything I m super-sensitive . I can see things others can t Hallucinations Hallucinations Paranoia Paranoia Its not safe there s ears everywhere Withdrawal/ Withdrawal/ Loss of motivation Loss of motivation I have no interest. I don t want to see anyone. I like being in my room I don t like people
Psychosis Psychoeducation Useful Methods of dealing with hallucinations and intrusive thoughts Engagement in activities Interpersonal contact Physical stimulation Relaxation Improved self esteem Aversion therapy Dismissal Ignoring voices Vocal activity Challenging reasoning Self monitoring Auditory stimulation
Psychosis Psychoeducation Main family factors which promote relapse Negative view of medical therapy and compliance Critical communication by family members Intrusiveness of family members Family Advice Family members to talk about fears and experiences (privately) and defuse self or patient blame Re-establish simple small family routines Allow space for the patient- they are easily overwhelmed Be patient and promote successful activities Discuss warning signs (when the patient is well) amongst trusted family members
Depression Psychoed Patient Advice Go slow- build assumption that recovery will take time Eating, sleeping and small amounts of exercise (yoga stretching is great) Encourage a match of feelings with situations- Encourage emotional stimulation & expression (depression becomes an emotional dead zone)-don t fear sadness Reduce alcohol and sedative use Family Advice Try to adjust to patient s mood (don t overdo cheerfulness or problem-solving) Reduce critical communication & demands (that is what the patient is doing to themselves already) Reduce patient s isolation in the family (return to being a person not a patient) Re-establish small family activities
Bipolar/ Manic Depression- Psychoeducation Central Issues Disrupted relationships due to manic/ depressive behaviour The patient s Cool approach to life (musicians & comedians) Grandiosity and inability to listen to others Reluctance to use medication Patient Advice Disrupted sleep patterns (re-establish/ avoid all- nighters) Alcohol & drug use (wind back) Impulsiveness (stop and think, wait one day) Excessive goal seeking (encourage holistic living and balance) Try the position of the patient being the best they can be Family advice- connect with the patient and positively ... Discourage alcohol use in home environment Encourage routines and sleep cycles Don t take things personally & view poor behaviour as temporary Take a positive approach to medication as needed
Drugs and Alcohol Biggest issues Motivation (they already know its wrong) Facilitating environments (drug use is often about social groups) The cool other side of the tracks lifestyle Depression and anxiety (especially in chronic drinkers) Patient Psychoeducation Its easier to move toward being a better person, a better lifestyle, a hopeful future than to STOP something. Foster ideas and greater goals & lifestyles. Ask about previous life stages or 2 years from now Inform about temporary side effects of withdrawal especially in the first 2 weeks (depression, anxiety and sleep disturbance) and reassure Provide information about alcohol & drugs fostering depression and anxiety rather than curing them Take position of informed and interested observer (rather than taking charge) to establish patient s responsibility/ explore consequences Get the family involved- it makes a huge difference for persistent recovery