Managing Antiretroviral Therapy Switches: Clinical Cases and Considerations
Explore clinical cases and considerations for switching antiretroviral therapy (ART) in patients with HIV. Topics include strategies for viral suppression, long-acting ART options, and managing virologic failure. Case presentations illustrate decision-making processes for optimizing ART regimens based on individual patient factors and treatment outcomes.

Uploaded on Nov 26, 2024 | 0 Views
Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
When and How To Switch Clara Lehmann, MD German Center For Infectious Research University of Cologne Cologne, Germany
Financial Relationships With Ineligible Companies (Formerly Described as Commercial Interests by the ACCME) Within the Last 2 Years: Dr Lehmann has no relevant financial relationships with ineligible companies to disclose. (Updated 12/14/22) Slide 2
Learning Objectives After attending this presentation, learners will be able to: Switch antiretroviral therapy (ART) in the setting of viral suppression Switch ART to long-acting cabotegravir and rilpivirine Switch ART for virologic failure Slide 3
Case 1 Man, 53 Years ART History: May 2015: Summer 2021 Diagnosed HIV infection HIV encephalopathy (multiple cerebral seizures at initial diagnosis) Nicotine abuse Arterial hypertension Hypercholesterolemia STEMI of the posterior wall with acute coronary syndrome. Recanalization, stent implantation Start: DTG/3TC/ABC Good tolerability Very good HIV surrogate parameters HIV-RNA < 20 cop/ml CD4 250/ l (16%) CD4 nadir 200/ l (12%), HIV: 850,000 cop/ml. Slide 5
ARS Question 1: What would you do? A. Continue his current ART B. Change his ABC/3TC to TAF / FTC containing regimen C. Change to DTG/3TC D. Some other option Slide 6
Can I switch patients with viral suppression in the setting of M184V or K65R mutations Slide 7
Case 2 Woman, 42 years Winter 2019: Resistance- Testing: Surrogate Parameters: Diagnosed HIV infection cerebral Toxoplasmosis Late Presenter NRTI: M184V NNRTI: none PI: none InSTI: none HIV-RNA < 20 cop/ml CD4 400/ l (35%) Initial: CD4 nadir 150/ l (15%) HIV: 650,000 cop/ml Start ART 2019: TAF/ FTC/ DRV/r Slide 8
ARS Question 2: What would you propose? A. TDF / 3TC/DOR B. FTC/TAF/BIC C. FTC/TAF/DRV/c D. TAF/FTC/DTG E. Other option Slide 9
High Efficacy of Switching to Bictegravir/FTC/TAF with Suppressed HIV and pre-existing M184V/I HIV RNA <50 (LOCF)(at last visit) 100% 100% Pooled data from 6 trials in which PWH and virologic suppression switched to B/F/TAF (n=1825 with baseline data) Preexisting M184V/I identified in 182 participants (10%) 98% of participants with pre- existing M184V/I maintained viral suppression 99% 99% 98% 100 80 Patients (%) 60 40 20 0 All All Patients* (n=1825) +PI-R (n=58) +NNRTI-R (n=97) +INSTI-R (n=4) (n=182) M184V/I LOCF: last observation carried forward. *Patients with baseline data. Sax PE, et al. AIDS. 2022 Slide 10
Should I switch to Long-acting Cabotegravir and Rilpivirine? Slide 11
CASE 3 AR, WOMEN 59 YEARS, KENYA ART History: May 2002: Concomitant-Medication: 03/05-08/05: AZT/3TC +CCR5 (Study) 08/05-03/10: ART break 03/10-05/15: EFV/TDF/FTC 05/15-09/16: TDF/FTC/RPV Since 09/16: FTC/TAF/RPV Diagnosed HIV infection Cured hepatitis B Arterial hypertension Hypercholesterolemia Candesartan 8 mg 1-0-0 Atorvastatin 20mg 1-0-0 Spring-Summer 2021: Complaints about taking medication every day Good tolerability Very good HIV surrogate parameters (09/21) HIV-RNA < 20 cop/ml CD4 400/ l (35%) Slide 12
ARS Question 3: At this point what would you propose? A. Talk to her and keep her on her current Rx (FTC/TAF/RPV) B. Resistance analysis on proviral HIV level C. CAB / RPV i.m. D. Some other option Slide 13
LONG ACTING CABOTEGRAVIR (CAB) AND RILPIVIRINE ( RPV) Indication Approved for treatment only in combination in patients Who are currently virologically suppressed on a stable antiretroviral regimen (HIV-1 RNA < 50 copies/mL) Without current or historically documented resistance to the NNRTI or INI class of drugs Without a history of virologic failure to NNRTI- and INI-class agents. Contraindications Active HBV infection unless also receiving an oral HBV active regimen Pregnancy or plans to become pregnant Receiving medications with significant drug interactions with CAB or RPV Slide 14
DOSING 8 Weeks 4 Weeks 4 Weeks Depot i.m. Depot i.m. Oral Lead in Etc. CAB LA 600 mg RPV LA 900 mg CAB LA 600 mg RPV LA 900 mg CAB 30 mg 1-0-0 RPV 25 mg 1-0-0 Depot injectionaccordingto the scheme (weeks) 0 - 4 - 8 etc. In case of termination/interruption of therapy, an oral suppressive regimen must be taken 4 weeks after the first injection or 8 weeks after the second/later injection. Slide 15
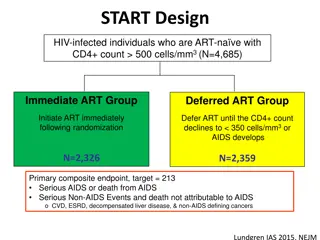
EFFICACY- ATLAS: Switch to LA CAB + RPV vs Continued 3-Drug ART in Virologically Suppressed Adults Adjusted Treatment Difference (95% CI) Virologic Outcomes at Wk 48 Continued ART LA CAB + LA RPV 92.595. 100 5 6% NI margin LA CAB + LA RPV (n = 308) 80 Primary Endpoint (HIV-1 RNA 50 copies/mL) LA CAB + LA RPV noninferior to continued BL ART 0.6 Patients (%) -1.2 2.5 60 Continued ART (n = 308) -10 -8 -6 -4 -2 Difference (%) 0 2 4 6 8 10 40 20 LA CAB + LA RPV Continued ART 5. 8 3. 6 1.6 Virologic Nonresponse ( 50 c/mL) 1. 0 0 Virologic Success (<50 c/mL) No Virologic Data Key Secondary Endpoint (HIV-1 RNA <50 copies/mL) LA CAB + LA RPV noninferior to continued BL ART -3.0 -10% NI margin 0.7 -6.7 -10 -8 -6 -4 -2 0 2 4 6 8 10 Difference (%) Swindells. NEJM. 2020;382:1112. Slide 16
Herbst 2021: How do I manage virologic failure ? Slide 17
Case 4 Man 46 Years, Nigeria ART History: May 2018: Fall 2021 Start: TDF / FTC / EFV Diagnosed HIV infection HIV-RNA 12.000 cop/ml CD4 / l 270 (16%) Good tolerability Very good HIV surrogate parameters Initial: CD4 nadir 250/ l (15%), HIV: 450,000 cop/ml (wild type) Resistance- Testing: Spring 2019 NRTI: M184V HIV-RNA < 40 cop/ml CD4 450/ l (21%) NNRTI Resistenz PI InSTI Slide 18
ARS Question 4: At this point which regimen would you choose? A. TDF / 3TC / DTG B. ABC/ 3TC / DTG C. TDF / 3TC / DRV/r D. FTC/TAF/BIC E. Some other option Slide 19
NADIA: 2nd-Line ART after NNRTI Failure HIV RNA <400 Copies/mL (ITT, week 96) 100 P=0.02 P=NS 92% 90 % 87 % 85 % Participants with virologic failure on TDF/3TC/NNRTI (n=464) 80 Randomized to switch to DTG or DRV/r with either TDF/3TC or AZT/3TC Participants (%) 60 Study participants: CD4 <200: 51%; VL >100,000: 28% Resistance: K65R/N: 50%; M184V: 86% 40 DTG + 2 NRTIs non-inferior to DRV/r + 2 NRTIs High rate of suppression even when no NRTIs predicted to be active! 20 0 Continuing TDF/3TC superior to switch to AZT/3TC TDF (n=233) ZDV (n=231) Darunavir/r (n=229) Dolutegravir (n=235) 9 participants (4%) in DTG group developed resistance; no resistance in the DRV/r group Paton N, Lancet, 2022 Slide 20
Conclusions Persons with suppressed virus and no history of transmitted or acquired HIV drug resistance can generally switch therapy to any of the recommended initial regimens (BIC/TAF/FTC, DTG plus TXF/XTC or DTG/3TC ) and maintain viral suppression. In persons with viral suppression switching to DTG plus 2 nRTIs or BIC/FTC/TAF, even in the setting of likely or proven nRTI resistance (M184V and K65R mutations) is safe. 2-drug regimens (DTG/3TCor DTG/RPV): unless there is documented or suspected history of treatment failure, proviral resistance testing is not required prior to switching to 2-drug therapy, even if there is no available pretreatment resistance test result (evidence rating: BII) Long-acting CAB + RPV is safe and effective ART for PLWH with proven viral suppression for at least 3 months and no history of treatment failure and no known or suspected resistance to CAB or RPV Slide 21