infant infant


S
l
e
e
p
d
i
s
o
r
d
e
r
s
i
n
c
h
i
l
d
r
e
n
a
n
d
i
n
f
a
n
t
Soroor Inaloo
Pediatric Neurologist, Shiraz University of Medical Science, 2022



ب
س
م
الله
ا
ل
ر
ح
م
ن
ا
ل
ر
ح
ی
م

S
l
e
e
p
d
i
s
o
r
d
e
r
s
•
Up to 50% of
children will experience a sleep problem
•
Early identification
of sleep problems may prevent negative
consequences, such as daytime sleepiness, irritability, behavioral
problems, learning difficulties, motor vehicle crashes in teenagers,
and poor academic performance
•
Obstructive sleep apnea occurs in 1% to 5% of children
•
Parasomnias are common in childhood
; sleepwalking, sleep talking,
confusional arousals, and sleep terrors tend to occur in the first half
of the night, whereas nightmares are more common in the second
half of the night
S
l
e
e
p
d
i
s
o
r
d
e
r
s
•
Sleep disorders in children are very common and can impair academic
function and daytime behavior
•
Clinicians should incorporate questions about sleep into their routine
health assessment of children
•
High risk groups
: children with neurodevelopmental problems,
learning problem, or behavior problems
•
Children with sleep disorders may present with
different symptoms
than do adults, and, within the pediatric age group, the clinical
manifestations of sleep problems may vary by
age and developmental
level
S
l
e
e
p
r
e
q
u
i
r
e
m
e
n
t
f
o
r
c
h
i
l
d
r
e
n
a
n
d
t
e
e
n
a
g
e
r
s
•
Infants 4 to 12 months – 12 to 16 hours (including naps)
•
Toddlers 1 to 2 years – 11 to 14 hours (including naps)
•
3- to 5-year-old children – 10 to 13 hours (including naps)
•
6- to 12-year-old children – 9 to 12 hours
•
Teens 13 to 18 years – 8 to 10 hours
S
c
r
e
e
n
i
n
g
t
e
s
t
•
A variety of checklists and questionnaires are available and may
supplement the history. As an example, BEARS is a screening acronym
that prompts a clinician to inquire about five sleep areas
•
B – Bedtime issues
•
E – Excessive daytime sleepiness
•
A – Awakenings during the night
•
R – Regularity and duration of sleep
•
S – Sleep-disordered breathing (or Snoring )
C
h
i
e
f
s
l
e
e
p
c
o
m
p
l
a
i
n
t
•
Despite the many ways children may experience sleep problems,
most complaints can be distilled into one (or more) of four
categories :
•
Difficulty initiating or maintaining sleep
•
Excessive daytime sleepiness
•
Snoring or other breathing problems during sleep
•
Abnormal movements or behaviors before or during sleep
A
d
d
i
t
i
o
n
a
l
s
l
e
e
p
h
i
s
t
o
r
y
Once the chief sleep complaint is identified, the history can focus on details
that distinguish among disorders in that category. The history should include:
● Sleep-wake schedule
● Duration and frequency of the problem, temporal profile of onset (abrupt,
gradual, intermittent), and degree of variability from night to night
● Interventions or strategies that have been tried, including any medications
used for sleep (either over-the-counter, prescription or herbal medications)
● Daytime symptoms that may be related to insufficient or disrupted sleep,
including sleepiness, hyperactivity, inattentiveness, or irritability
U
s
e
f
u
l
t
o
o
l
s
i
n
c
l
u
d
e
•
Sleep logs
•
Questionnaires
•
Video recordings
S
l
e
e
p
l
o
g
s
•
Completion of a sleep log (sleep diary) during the two weeks prior to evaluation
may provide important information regarding the sleep-wake pattern and
nocturnal events
•
Bed time and rise time
•
Time of sleep onset and awakenings
•
Other nocturnal events
•
Perceived quality of sleep
•
Naps
•
Eating/feeding pattern
•
Degree of alertness or sleepiness during the day
•
Observations regarding nocturnal events and medical or psychological stressors
C
o
n
c
o
m
i
t
a
n
t
m
e
d
i
c
a
l
p
r
o
b
l
e
m
s
•
Reactive airways disease, gastro-esophageal reflux, congenital heart
disease, arthritis, and other causes of chronic pain
•
Altered craniofacial anatomy
•
Neurologic disorders such as cerebral palsy, intellectual disability,
autism spectrum disorder and related disorders, and blindness
•
Attention deficit hyperactivity disorder (ADHD), in which the
association with sleep disorders is probably
bidirectional
•
Anxiety or depression, which may cause or exacerbate sleep problems
such as difficulty initiating or maintaining sleep (insomnia)
•
Medications, caffeine and alcohol
P
H
Y
S
I
C
A
L
E
X
A
M
I
N
A
T
I
O
N
•
General physical examination
:
•
General
– Observations include the child's level of alertness during the
examination
•
Repetitive yawning, droopy eyelids, blank facial expression, frequent changes in
position, overactivity, and irritability may indicate excessive sleepiness
•
Persistent mouth breathing or noisy breathing may suggest nasal obstruction
•
Growth
– Excessive weight gain and obesity > obstructive sleep apnea (OSA)
•
Failure to thrive > consequence of OSA, or of an underlying chronic medical
disorder
•
Dysmorphic features
– Several syndromes or anomalies are associated with OSA
•
-Down syndrome or Prader-Willi syndrome
•
-Craniofacial anomalies, such as macrocephaly, microcephaly, micrognathia, or
Pierre Robin syndrome
•
Clubbing, cyanosis, or edema may suggest heart failure
•
Lung examination may suggest chronic lung disease or reactive airways disease
P
H
Y
S
I
C
A
L
E
X
A
M
I
N
A
T
I
O
N
•
Oropharynx/airway examination
:
•
Oropharyngeal features associated with OSA include tonsillar or adenoidal
hypertrophy, abnormally small upper airway, mandibular hypoplasia,
micrognathia, retrognathia, high-arched hard palate, adenoidal facies
(elongated face, mouth breathing )
•
Absent gag reflex, poor movement of the soft palate, or swallowing
problems suggest bulbar dysfunction, which is associated with OSA
•
Neurologic examination:
•
Evaluate for signs of neuromuscular disease, including scoliosis and
weakness
•
Assess developmental milestones and cognitive function
S
l
e
e
p
d
i
s
o
r
d
e
r
s
Work up
P
o
l
y
s
o
m
n
o
g
r
a
p
h
y
Polysomnography (PSG) typically consists of an all-night recording performed in the
sleep laboratory to characterize sleep architecture and sleep pathology
•
Indications :
•
Assessment for a sleep-related breathing disorder (eg, obstructive sleep apnea
[OSA])
•
Assessment for narcolepsy (in conjunction with a multiple sleep latency test [MSLT])
•
Assessment for periodic limb movement disorder (PLMD)
•
Titration of continuous positive airway pressure (CPAP)
•
Patients with neuromuscular disorders and sleep-related symptoms
•
Parasomnia with clinical suspicion for a sleep-related breathing disorder or PLMD
•
Selected children with suspected restless legs syndrome (RLS) who require
supportive data for the diagnosis
P
o
l
y
s
o
m
n
o
g
r
a
p
h
y
w
i
t
h
E
E
G
PSG with an expanded electroencephalography (EEG montage; typically
16-channels) may be indicated for :
•
Patients with suspected sleep-related epilepsy when the initial clinical
evaluation and standard EEG are inconclusive, to help distinguish the
disorder from a parasomnia
•
Patients with an atypical or potentially injurious parasomnia, to
confirm the diagnosis and assess for sleep-related epilepsy
M
a
n
a
g
e
m
e
n
t
o
f
s
l
e
e
p
d
i
s
o
r
d
e
r
s
H
e
a
l
t
h
y
s
l
e
e
p
p
r
a
c
t
i
c
e
s
f
o
r
c
h
i
l
d
r
e
n
•
Have a set bedtime and bedtime routine for your child
•
Bedtime and wake-up time should be approximately the same time
on school nights and non-school nights. There should not be more
than about
an hour
difference from 1 day to another
•
Make the hour before bed shared quiet time.
Avoid high-energy
activities
, such as rough play, and stimulating activities, such as
watching television or playing computer games, just before bed
•
Don't send your child to
bed hungry
. A light snack (such as milk and
cookies) before bed is a good idea. Heavy meals within an hour or 2
of bedtime, however, may interfere with sleep
H
e
a
l
t
h
y
s
l
e
e
p
p
r
a
c
t
i
c
e
s
f
o
r
c
h
i
l
d
r
e
n
•
Avoid products containing caffeine (caffeinated sodas, coffee, tea, and
chocolate )
•
Make sure your child
spends time outside
(for exposure to natural
light) every day whenever possible and is involved in regular exercise
•
Keep your child's
bedroom quiet and dark
. A low-level night light is
acceptable for children who find completely dark rooms frightening
•
Keep your child's bedroom at a
comfortable temperature
during the
night (approximately 65°F)
•
Don't use your child's bedroom for time-out or punishmen
H
e
a
l
t
h
y
s
l
e
e
p
p
r
a
c
t
i
c
e
s
f
o
r
c
h
i
l
d
r
e
n
•
Avoid use of electronic media devices
(televisions, laptop, computers ) for at least 1 hour
before bedtime, and keep these devices out of the bedroom. Children can easily develop
the bad habit of using social media after bedtime or "needing" the television to fall
asleep. It's much more difficult to control your child's electronic media if the devices are
in the bedroom
•
Mindell J, Owens J. Sleep Hygiene: Healthy Sleep Habits for Children and Adolescents. In: A Clinical Guide to Pediatric Sleep, 2nd ed,
Lippincott Williams & Wilkins, Philadelphia 2009
Common sleep problems
D
i
f
f
i
c
u
l
t
y
i
n
i
t
i
a
t
i
n
g
o
r
m
a
i
n
t
a
i
n
i
n
g
s
l
e
e
p
r
i
s
k
f
a
c
t
o
r
s
Bedtime routine
•
Stimulating activities (such as television sets, laptop computers or
tablets, cell phones, or video games in the bedroom)
•
Presence of a parent/caregiver as the child falls asleep
•
Siblings or other children in the bedroom
•
Environmental circumstances (eg, a loud or unsafe neighborhood
•
Increased attention from the parent/caregiver in response to a child's
stalling behavior at bedtime
D
i
f
f
i
c
u
l
t
y
i
n
i
t
i
a
t
i
n
g
o
r
m
a
i
n
t
a
i
n
i
n
g
s
l
e
e
p
r
i
s
k
f
a
c
t
o
r
s
Pre-sleep activities
•
Periods of exercise, competitive sports and sedentary activity – One
study suggests that physical activity reduces sleep latency, while
sedentary activity during the day is associated with increased sleep
latency
•
Use of electronic devices and social media are important contributors
to delayed sleep onset, whereas spending time with family may be
protective
•
A meta-analysis of studies in children <5 years of age found an
inverse association between total daily screen time and sleep
duration
D
i
f
f
i
c
u
l
t
y
i
n
i
t
i
a
t
i
n
g
o
r
m
a
i
n
t
a
i
n
i
n
g
s
l
e
e
p
r
i
s
k
f
a
c
t
o
r
s
Response to nighttime awakenings
•
When children experience nighttime awakenings, the
parent/caregiver's response can promote or extinguish the behavior.
As an example, excessive parental attention in response to nighttime
awakenings (including routinely allowing the child to switch beds)
may perpetuate the problem
•
For healthy toddlers and older infants, habitual nighttime feedings
may disrupt sleep and are unnecessary
D
i
f
f
i
c
u
l
t
y
i
n
i
t
i
a
t
i
n
g
o
r
m
a
i
n
t
a
i
n
i
n
g
s
l
e
e
p
•
Delayed sleep-wake phase disorder
•
Restless legs syndrome (RLS)
•
Nightmares
•
Psychosocial dysfunction
•
Anxiety or depression
•
Concomitant medical problems
D
a
y
t
i
m
e
s
l
e
e
p
i
n
e
s
s
The most common causes of daytime sleepiness include :
•
Insufficient nocturnal sleep compared with the average sleep
requirements for the age group
•
Poor sleep hygiene
•
Medication side effects
•
Less common but important causes include narcolepsy, obstructive
sleep apnea (OSA), idiopathic hypersomnia, and periodic limb
movement disorder (PLMD)
O
b
s
t
r
u
c
t
i
v
e
S
l
e
e
p
A
p
n
e
a
•
OSA is characterized by upper airway obstruction, despite respiratory
effort, that disrupts normal sleep patterns and ventilation
Etiology
•
Obesity
•
Excessive soft tissue in the upper airway
•
Decreased upper airway lumen size
•
Failure of pharyngeal dilator muscles
However, in children, the obstruction is primarily due to enlarged
tonsils and adenoids
O
b
s
t
r
u
c
t
i
v
e
S
l
e
e
p
A
p
n
e
a
•
Prevalence: 1% to 5% Onset between 2 and 8 years of age Affects males and females
equally More common in blacks and in persons with craniofacial abnormalities (e.g.,
micrognathia, retrognathia, midfacial hypoplasia), Down syndrome, neuromuscular
diseases, choanal atresia
Clinical presentation
•
Snoring Unusual sleep positions (e.g., hyperextended neck, seated with open mouth)
Sleep-related paradoxical breathing ,Nighttime ,enuresis , diaphoresis, Morning
headaches ,Cognitive/behavioral issues (e.g., depressed mood, poor concentration,
decreased attention) ,Excessive daytime sleepiness (less common) ,Enlarged tonsils and
adenoids ,Pectus excavatum
•
Diagnosis
:PSG is required for diagnosis (apnea-hypopnea index greater than 1.5 per
hour)
•
Treatment
:
First line: Adenotonsillectomy
Other: Continuous positive airway pressure,
nasal steroids, rapid maxillary expansion (i.e., orthodontic device widens the upper jaw)
P
a
r
a
s
o
m
n
i
a
s
S
l
e
e
p
w
a
l
k
i
n
g
(
s
o
m
n
a
m
b
u
l
i
s
m
)
•
Prevalence: 17% in children, 4% in adults
Peaks between 8 and 12 years of age
More common in
males
Familial history
of sleepwalking: 1 parent = 45% risk 2
parents = 60% risk
•
Ambulation, during sleep Difficult to awaken during episode ,Eyes open
Confusion/agitation ,Unusual or dangerous behaviors ,Rapid return to sleep ,
Usually occurs during the first half of the sleep period, with
no memory
of the
event Patient may have coexisting confusional arousals and/or sleep terrors
•
Diagnosed by history
PSG not require
•
Treatment:
•
Reassurance (usually resolves spontaneously) Increase total sleep time Scheduled
awakenings ,Bedroom/home safety counseling ,Screening for
precipitating factors
(e.g., sleep deprivation, obstructive sleep apnea, gastroesophageal reflux disease,
acute stress, medication or illicit drug use)
•
Hypnosis ,Scheduled awakening ( 15-30 minute ),Benzodiazepines , TCA?
C
o
n
f
u
s
i
o
n
a
l
a
r
o
u
s
a
l
s
•
Prevalence: 17.3% in 3- to 13-year-olds, 2.9% to 4.2% in those older
than 15 years Affects males and females equally Strong familial
pattern
•
“Sleep drunkenness” Inappropriate behavior Slowed responsiveness
Slurred speech Confusion after awakening
•
Usually occurs during the first half of the sleep period, with no
memory of the event
•
Diagnosed by history PSG not require
•
Reassurance (usually resolves spontaneously) Increase total sleep
time Scheduled awakenings, Bedroom/home safety counseling
S
l
e
e
p
t
e
r
r
o
r
s
•
Episodes of sleep terror occur
in 1% to 6% of children
,
•
with a peak between
4 and 8 years of age
; gender differences have not been observed
•
The child may sit up suddenly and scream with a blood-curdling “battle-cry.”
•
intense fear (e.g., screaming, crying, confusion, walking), and this is accompanied by
apparent autonomic activation, including mydriasis, tachycardia, and diaphoresis
•
Difficult to awaken from episode ,Usually occurs during the first half of the sleep period,
with
no memory
of
the event, Considerable overlap with other parasomnia
•
The event may last from a
few minutes up to 20 minutes,
but a longer duration May also
be seen
•
Diagnosed by history PSG not required
•
Reassurance (usually resolves spontaneously) Increase total sleep time Scheduled
awakenings , Bedroom/home safety counseling ,Benzodiazepines
N
i
g
h
t
m
a
r
e
s
•
Prevalence:
10% to 50%
in 3- to 5-year-olds
•
Onset
between 3 and 6 years
of age, peaks between 6 and 10 years of age
Affects males and females equally
•
Unpleasant dreams Increased sympathetic response (increased heart and
respiratory rates, diaphoresis) Usually occurs during the second half of the
sleep period, with
clear memory of the event
•
May be associated with mood disorders or posttraumatic stress disorder
•
Diagnosed by history PSG not required
•
Reassurance (usually resolves spontaneously) Increase total sleep time
Scheduled awakenings , Bedroom/home safety counseling , Cognitive
behavior therapy Medications that suppress rapid eye movement sleep
(selective serotonin reuptake inhibitors ( fluoxetine, citalopram …) ; off-
label use)
R
e
s
t
l
e
s
s
l
e
g
s
y
n
d
r
o
m
e
•
Unpleasant sensation in the legs, with the urge to move the legs starting in
the evening
•
Rest worsens symptoms, and movement provides some relief. Other
symptoms include difficulty falling asleep, bedtime resistance, “growing
pains,” and symptoms similar to those of attention-deficit/hyperactivity
disorder
•
Dopamine dysfunction,
genetics
,
and iron deficiency
are thought to play a
role in the pathogenesis of restless legs syndrome
•
Exacerbated by excessive or inadequate physical activity or the use of
caffeine, nicotine, antihistamines, selective serotonin reuptake inhibitors,
or tricyclic antidepressants
•
Iron replacement should be initiated if ferritin levels are less than 50 mcg
per L, and they should be rechecked in three months
T
r
e
a
t
m
e
n
t
o
f
r
e
s
t
l
e
s
s
l
e
g
s
y
x
•
D
opaminergic medications are widely used and considered first-line treatment
for RLS
•
Carbidopa/levodopa and dopamine agonists (pramipexole and ropinirole) are
commonlused, and
ropinirole
was the first FDA-approved medication for
treatment of moderate to severe primary RLS
•
Another medication not FDA-approved for the treatment aof RLS in children but
used clinically is
clonidine
,
Clonazepam , gabapentine
D
e
l
a
y
e
d
S
l
e
e
p
P
h
a
s
e
D
i
s
o
r
d
e
r
•
The disorder is more common during adolescence when the circadian
rhythm is thought to lengthen and the child becomes more social
•
The prevalence in adolescents is 7% to 16%
Treatment :
•
Avoid bright lights before bedtime
•
Removing all light-emitting devices (e.g., electronics, portable media,
tablet computers, cell phones)
•
Bright light therapy used for the first one to two hours after awakening
•
There is strong evidence that
melatonin
supplementation (0.3 to 5 mg
given 1.5 to 6.5 hours before desired bedtime) is effective
P
h
a
r
m
a
c
o
t
h
e
r
a
p
y
i
n
s
l
e
e
p
d
i
s
o
r
d
e
r
s
•
The decision about whether to initiate pharmacotherapy should be
individualized, based on the above evaluation. Other key considerations include:
•
Child's age
–
Pharmacotherapy is rarely
appropriate for young children (<5 years),
except for unusual circumstances such as significant caregiver physical or mental
health issues or risk of child abuse. This is because behavioral causes and
interventions are particularly common in this age group and also because of the
lack of safety and efficacy data in this age group
•
Acute versus chronic sleep problem
– Children with underlying medical,
psychiatric, or neurodevelopmental conditions, in comparison with otherwise
healthy, typically developing children, are more likely to need longer-term
pharmacotherapy to address sleep issues. For children with these comorbid
conditions, it is particularly important to address behavioral issues and to select
medications that are less likely to have long-term side effects
•
The most realistic immediate goal of treatment may be to improve rather than
eliminate sleep problems
•
The
half-life and duration of action of the medication
is particularly
important and should be appropriate for the presenting complaint
•
For children with
sleep onset problems, a shorter-acting medication
is generally desirable
•
whereas for
sleep maintenance problems, longer-acting medications
may be considered, while at the same time minimizing morning
residual sleepiness
•
Dosing
– The medication should be initiated at the lowest level and titrated up as necessary
•
limited data on the pharmacokinetic and pharmacodynamic properties for hypnotic drugs in the
pediatric
•
For some medications (eg,
zolpidem
)
evidence suggests that younger children may require higher
dosing (per kg) compared with adults due to differences in metabolism
•
For some medications, this difference in metabolism results in a paradoxical reaction
•
Timing
– Drug administration should be tailored to the drug's onset of action and the target time of
sleep onset. Because most hypnotic medications have their
onset of action within 30 minutes
of
administration and
peak within one to two hours,
they should be administered shortly before
bedtime for sleep-onset insomnia, eg, within 30 minutes of lights out
D
u
r
a
t
i
o
n
o
f
p
h
a
r
m
a
c
o
t
h
e
r
a
p
y
•
The duration of pharmacotherapy depends on the
type of sleep problem
and the child's response to medical and behavioral treatment
•
In general, medications should also be used for the shortest possible
duration
•
Avoid abrupt discontinuation
of sleep medication, especially for drugs with
short and intermediate half-lives
•
Failure to wean sleep medications gradually because increased chance of:
•
"
rebound insomnia"
and increase the likelihood of
other sleep disorders
For example, selective serotonin reuptake inhibitors [SSRIs]) may result in a
compensatory increase (rebound) in REM sleep and a subsequent increase
in REM sleep-related phenomena, such as nightmares
D
o
s
i
n
g
a
n
d
a
d
m
i
n
i
s
t
r
a
t
i
o
n
o
f
m
e
l
a
t
o
n
i
n
•
Circadian phase delay
•
(eg, 0.2 to 0.5 mg)
are typically given three to five hours prior to actual sleep
onset time
(or one to two hours before the desired bedtime).
These relatively
small doses and advance administration are more effective for circadian phase
delay than larger doses or those given closer to sleep onset and appear to be safe
•
Sleep-onset insomnia
–
•
1 to 2 mg in preschool children,
•
2 to 3 mg in school-aged children
•
5 mg in adolescents
•
Given 30 minutes before
bedtime
•
Dosing should always begin at the lower range and be titrated up on a weekly
basis as needed. Studies in children with
autism
have reported using doses of
up
to 10 mg
(maximum dose recommended in guidelines for this population
A
d
v
e
r
s
e
e
f
f
e
c
t
s
o
f
m
e
l
a
t
o
n
i
n
•
Studies of melatonin use for durations of
up to four years no
significant adverse effects
in a variety of pediatric populations
•
Potential side effects include suppression of the hypothalamic-
gonadal axis (triggering precocious puberty on discontinuation),
although at least one study found no effects on pubertal
development
•
Increased reactivity of the immune system in children with immune
disorders or on immunosuppressants (ie, corticosteroids) has also
been postulated
•
At least one small study in adults suggested no suppression of
endogenous melatonin with exogenous administration
B
e
n
z
o
d
i
a
z
e
p
i
n
e
s
•
BZDs
reduce sleep latency and may increase total sleep time
; those
BZDs with a longer half-life and duration of action have been more
commonly used to address sleep maintenance
•
BZDs have effects on sleep architecture, most notably, reduction in
slow-wave sleep (SWS). These drugs also have muscle relaxant,
anxiolytic, and anticonvulsant properties
•
BZDs are occasionally used to treat intractable partial arousal
parasomnias such as
sleep terrors
in children
•
Side effects
of BZDs include morning residual sleepiness, daytime
sleepiness, and compromised daytime functioning
A
l
p
h
a
-
a
d
r
e
n
e
r
g
i
c
a
g
o
n
i
s
t
s
•
Alpha-adrenergic agonists (especially
clonidine
) are commonly
prescribed to treat childhood insomnia. Anecdotal clinical experience
suggests that these drugs are generally effective and well tolerated in
children with
ADHD and sleep-onset insomnia
•
Drug is rapidly absorbed with an
onset of action within one hour
and
peak effects at two to four hours
•
Clonidine
has a narrow therapeutic index
. As a result, concerns have
been raised about the potential for accidental or intentional overdose
and associated toxicity, which may include respiratory depression,
hypotension, and bradycardia
A
n
t
i
d
e
p
r
e
s
s
a
n
t
s
•
Use of low- dose
doxepin
and
trazodone
, and that tolerability and
safety of antidepressants for insomnia is uncertain due to limited
reporting of adverse events
•
Antidepressants should be used for insomnia only in the presence of
comorbid mood issues
•
Most antidepressants, especially those with anticholinergic effects,
suppress REM sleep and increase latency to REM sleep; thus, abrupt
withdrawal may lead to increased nightmares as a result of REM sleep
rebound
T
r
i
c
y
c
l
i
c
a
n
t
i
d
e
p
r
e
s
s
a
n
t
s
•
Most TCAs are sedating; the most sedating drugs are
amitriptyline
,
doxepin
,
and
trimipramine
. TCAs decrease SOL (sleep onset latency ) and arousals and
have been used to treat insomnia in adults who have underlying depression
•
The most commonly reported
side effects
of TCAs are anxiety and agitation, as
well as anticholinergic effects such as blurred vision, dry mouth, urinary
retention, and orthostatic hypotension.
•
There is a risk of cardiotoxicity, especially in prepubertal children,
•
Most TCAs are potent REM sleep suppressants; thus, rapid withdrawal may lead
to
REM sleep rebound and nightmares
•
TCAs also tend to suppress SWS, and
withdrawal may lead to SWS rebound and
an
increase
in partial-arousal parasomnias such as
sleepwalking and sleep terrors
TCAs may also exacerbate
restless legs syndrome
(RLS) symptoms.
S
e
l
e
c
t
i
v
e
s
e
r
o
t
o
n
i
n
r
e
u
p
t
a
k
e
i
n
h
i
b
i
t
o
r
s
•
Selective serotonin reuptake inhibitors (SSRIs) vary widely in their
effects on sleep.
Fluvoxamine
,
paroxetine
, and
citalopram
tend to be
sedating and may be useful for management of insomnia in patients
with
underlying depression
O
t
h
e
r
m
e
d
i
c
a
t
i
o
n
s
•
Other classes of medications that reportedly have been used in clinical
practice for pediatric insomnia, especially in patients with a comorbid
neurodevelopmental or mood disorder, include mood stabilizers and
anticonvulsants (eg,
carbamazepine
, valproic acid, topiramate,
gabapentin
),
atypical antipsychotics (
risperidone
,
olanzapine
,
quetiapine
), and
chloral
hydrate
. In most instances, these medications are prescribed for other
indications such as bipolar disorder, aggression, or pain but may
simultaneously be prescribed for their sleep-promoting properties. Clinical
data for all of these agents in the pediatric population are largely limited to
case reports and case studies, and evidence is also very limited in adults
•
All of these medications should be used with caution
•
chloral hydrate
and
barbiturates
should not be used
to treat insomnia in
children, because of significant side effects.
H
o
m
e
m
e
s
s
a
g
e
•
Up to 50% of children will experience a sleep problem
•
Vast majority of sleep disturbances in children and adolescents are appropriately
managed with
behavioral therapy alone
•
pharmacotherapy is rarely
necessary or appropriate for healthy children with sleep
problems
•
The decision to initiate pharmacotherapy should be made on a case-by-case basis after a
careful assessment of the sleep problem, including behavioral, medical, and psychosocial
contributors
•
Antihistamines
can be considered for short-term situational or occasional use in younger
children, especially those with comorbid atopic disease
•
Melatonin
is most appropriately used in patients with circadian phase delay, sleep-onset
insomnia
•
Alpha-adrenergic agonists
(
clonidine
or
guanfacine
) are commonly used off-label for
treatment of insomnia in children, particularly those with sleep onset delay and ADHD
•
Antidepressants
should be used for insomnia only in the presence of comorbid mood
issues
T
h
a
n
k
y
o
u
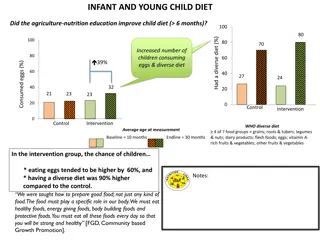
Sleep disorders in children can have significant impacts on their academic performance, behavior, and overall well-being. Identifying these disorders early is essential to prevent negative consequences such as daytime sleepiness, irritability, and learning difficulties. Common disorders like obstructive sleep apnea and parasomnias need to be addressed to ensure children get the quality sleep they need for optimal development.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author. Download presentation by click this link. If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
E N D
Presentation Transcript
Sleep disorders in children and Sleep disorders in children and infant infant Soroor Inaloo Pediatric Neurologist, Shiraz University of Medical Science, 2022
Sleep disorders Sleep disorders Up to 50% of children will experience a sleep problem Early identification of sleep problems may prevent negative consequences, such as daytime sleepiness, irritability, behavioral problems, learning difficulties, motor vehicle crashes in teenagers, and poor academic performance Obstructive sleep apnea occurs in 1% to 5% of children Parasomnias are common in childhood; sleepwalking, sleep talking, confusional arousals, and sleep terrors tend to occur in the first half of the night, whereas nightmares are more common in the second half of the night
Sleep disorders Sleep disorders Sleep disorders in children are very common and can impair academic function and daytime behavior Clinicians should incorporate questions about sleep into their routine health assessment of children High risk groups : children with neurodevelopmental problems, learning problem, or behavior problems Children with sleep disorders may present with different symptoms than do adults, and, within the pediatric age group, the clinical manifestations of sleep problems may vary by age and developmental level
Sleep requirement for children and teenagers Sleep requirement for children and teenagers Infants 4 to 12 months 12 to 16 hours (including naps) Toddlers 1 to 2 years 11 to 14 hours (including naps) 3- to 5-year-old children 10 to 13 hours (including naps) 6- to 12-year-old children 9 to 12 hours Teens 13 to 18 years 8 to 10 hours
Screening test Screening test A variety of checklists and questionnaires are available and may supplement the history. As an example, BEARS is a screening acronym that prompts a clinician to inquire about five sleep areas B Bedtime issues E Excessive daytime sleepiness A Awakenings during the night R Regularity and duration of sleep S Sleep-disordered breathing (or Snoring )
Chief sleep complaint Chief sleep complaint Despite the many ways children may experience sleep problems, most complaints can be distilled into one (or more) of four categories : Difficulty initiating or maintaining sleep Excessive daytime sleepiness Snoring or other breathing problems during sleep Abnormal movements or behaviors before or during sleep
Additional sleep history Additional sleep history Once the chief sleep complaint is identified, the history can focus on details that distinguish among disorders in that category. The history should include: Sleep-wake schedule Duration and frequency of the problem, temporal profile of onset (abrupt, gradual, intermittent), and degree of variability from night to night Interventions or strategies that have been tried, including any medications used for sleep (either over-the-counter, prescription or herbal medications) Daytime symptoms that may be related to insufficient or disrupted sleep, including sleepiness, hyperactivity, inattentiveness, or irritability
Useful tools include Useful tools include Sleep logs Questionnaires Video recordings
Sleep logs Sleep logs Completion of a sleep log (sleep diary) during the two weeks prior to evaluation may provide important information regarding the sleep-wake pattern and nocturnal events Bed time and rise time Time of sleep onset and awakenings Other nocturnal events Perceived quality of sleep Naps Eating/feeding pattern Degree of alertness or sleepiness during the day Observations regarding nocturnal events and medical or psychological stressors
Concomitant medical problems Concomitant medical problems Reactive airways disease, gastro-esophageal reflux, congenital heart disease, arthritis, and other causes of chronic pain Altered craniofacial anatomy Neurologic disorders such as cerebral palsy, intellectual disability, autism spectrum disorder and related disorders, and blindness Attention deficit hyperactivity disorder (ADHD), in which the association with sleep disorders is probably bidirectional Anxiety or depression, which may cause or exacerbate sleep problems such as difficulty initiating or maintaining sleep (insomnia) Medications, caffeine and alcohol
PHYSICAL EXAMINATION PHYSICAL EXAMINATION General physical examination: General Observations include the child's level of alertness during the examination Repetitive yawning, droopy eyelids, blank facial expression, frequent changes in position, overactivity, and irritability may indicate excessive sleepiness Persistent mouth breathing or noisy breathing may suggest nasal obstruction Growth Excessive weight gain and obesity > obstructive sleep apnea (OSA) Failure to thrive > consequence of OSA, or of an underlying chronic medical disorder Dysmorphic features Several syndromes or anomalies are associated with OSA -Down syndrome or Prader-Willi syndrome -Craniofacial anomalies, such as macrocephaly, microcephaly, micrognathia, or Pierre Robin syndrome Clubbing, cyanosis, or edema may suggest heart failure Lung examination may suggest chronic lung disease or reactive airways disease
PHYSICAL EXAMINATION PHYSICAL EXAMINATION Oropharynx/airway examination: Oropharyngeal features associated with OSA include tonsillar or adenoidal hypertrophy, abnormally small upper airway, mandibular hypoplasia, micrognathia, retrognathia, high-arched hard palate, adenoidal facies (elongated face, mouth breathing ) Absent gag reflex, poor movement of the soft palate, or swallowing problems suggest bulbar dysfunction, which is associated with OSA Neurologic examination: Evaluate for signs of neuromuscular disease, including scoliosis and weakness Assess developmental milestones and cognitive function
Sleep disorders Sleep disorders Work up
Polysomnography Polysomnography Polysomnography (PSG) typically consists of an all-night recording performed in the sleep laboratory to characterize sleep architecture and sleep pathology Indications : Assessment for a sleep-related breathing disorder (eg, obstructive sleep apnea [OSA]) Assessment for narcolepsy (in conjunction with a multiple sleep latency test [MSLT]) Assessment for periodic limb movement disorder (PLMD) Titration of continuous positive airway pressure (CPAP) Patients with neuromuscular disorders and sleep-related symptoms Parasomnia with clinical suspicion for a sleep-related breathing disorder or PLMD Selected children with suspected restless legs syndrome (RLS) who require supportive data for the diagnosis
Polysomnography Polysomnography with EEG with EEG PSG with an expanded electroencephalography (EEG montage; typically 16-channels) may be indicated for : Patients with suspected sleep-related epilepsy when the initial clinical evaluation and standard EEG are inconclusive, to help distinguish the disorder from a parasomnia Patients with an atypical or potentially injurious parasomnia, to confirm the diagnosis and assess for sleep-related epilepsy
Management of sleep disorders Management of sleep disorders
Healthy sleep practices for children Healthy sleep practices for children Have a set bedtime and bedtime routine for your child Bedtime and wake-up time should be approximately the same time on school nights and non-school nights. There should not be more than about an hour difference from 1 day to another Make the hour before bed shared quiet time. Avoid high-energy activities, such as rough play, and stimulating activities, such as watching television or playing computer games, just before bed Don't send your child to bed hungry. A light snack (such as milk and cookies) before bed is a good idea. Heavy meals within an hour or 2 of bedtime, however, may interfere with sleep
Healthy sleep practices for children Healthy sleep practices for children Avoid products containing caffeine (caffeinated sodas, coffee, tea, and chocolate ) Make sure your child spends time outside (for exposure to natural light) every day whenever possible and is involved in regular exercise Keep your child's bedroom quiet and dark. A low-level night light is acceptable for children who find completely dark rooms frightening Keep your child's bedroom at a comfortable temperature during the night (approximately 65 F) Don't use your child's bedroom for time-out or punishmen
Healthy sleep practices for children Healthy sleep practices for children Avoid use of electronic media devices (televisions, laptop, computers ) for at least 1 hour before bedtime, and keep these devices out of the bedroom. Children can easily develop the bad habit of using social media after bedtime or "needing" the television to fall asleep. It's much more difficult to control your child's electronic media if the devices are in the bedroom Mindell J, Owens J. Sleep Hygiene: Healthy Sleep Habits for Children and Adolescents. In: A Clinical Guide to Pediatric Sleep, 2nd ed, Lippincott Williams & Wilkins, Philadelphia 2009
Difficulty initiating or maintaining sleep Difficulty initiating or maintaining sleep risk factors risk factors Bedtime routine Stimulating activities (such as television sets, laptop computers or tablets, cell phones, or video games in the bedroom) Presence of a parent/caregiver as the child falls asleep Siblings or other children in the bedroom Environmental circumstances (eg, a loud or unsafe neighborhood Increased attention from the parent/caregiver in response to a child's stalling behavior at bedtime
Difficulty initiating or maintaining sleep Difficulty initiating or maintaining sleep risk factors risk factors Pre-sleep activities Periods of exercise, competitive sports and sedentary activity One study suggests that physical activity reduces sleep latency, while sedentary activity during the day is associated with increased sleep latency Use of electronic devices and social media are important contributors to delayed sleep onset, whereas spending time with family may be protective A meta-analysis of studies in children <5 years of age found an inverse association between total daily screen time and sleep duration
Difficulty initiating or maintaining sleep Difficulty initiating or maintaining sleep risk factors risk factors Response to nighttime awakenings When children parent/caregiver's response can promote or extinguish the behavior. As an example, excessive parental attention in response to nighttime awakenings (including routinely allowing the child to switch beds) may perpetuate the problem For healthy toddlers and older infants, habitual nighttime feedings may disrupt sleep and are unnecessary experience nighttime awakenings, the
Difficulty initiating or maintaining sleep Difficulty initiating or maintaining sleep Delayed sleep-wake phase disorder Restless legs syndrome (RLS) Nightmares Psychosocial dysfunction Anxiety or depression Concomitant medical problems
Daytime sleepiness Daytime sleepiness The most common causes of daytime sleepiness include : Insufficient nocturnal sleep compared with the average sleep requirements for the age group Poor sleep hygiene Medication side effects Less common but important causes include narcolepsy, obstructive sleep apnea (OSA), idiopathic hypersomnia, and periodic limb movement disorder (PLMD)
Obstructive Sleep Apnea Obstructive Sleep Apnea OSA is characterized by upper airway obstruction, despite respiratory effort, that disrupts normal sleep patterns and ventilation Etiology Obesity Excessive soft tissue in the upper airway Decreased upper airway lumen size Failure of pharyngeal dilator muscles However, in children, the obstruction is primarily due to enlarged tonsils and adenoids
Obstructive Sleep Apnea Obstructive Sleep Apnea Prevalence: 1% to 5% Onset between 2 and 8 years of age Affects males and females equally More common in blacks and in persons with craniofacial abnormalities (e.g., micrognathia, retrognathia, midfacial hypoplasia), Down syndrome, neuromuscular diseases, choanal atresia Clinical presentation Snoring Unusual sleep positions (e.g., hyperextended neck, seated with open mouth) Sleep-related paradoxical breathing ,Nighttime ,enuresis , diaphoresis, Morning headaches ,Cognitive/behavioral issues (e.g., depressed mood, poor concentration, decreased attention) ,Excessive daytime sleepiness (less common) ,Enlarged tonsils and adenoids ,Pectus excavatum Diagnosis :PSG is required for diagnosis (apnea-hypopnea index greater than 1.5 per hour) Treatment :First line: Adenotonsillectomy Other: Continuous positive airway pressure, nasal steroids, rapid maxillary expansion (i.e., orthodontic device widens the upper jaw)
Parasomnias Parasomnias Sleepwalking (somnambulism) Sleepwalking (somnambulism) Prevalence: 17% in children, 4% in adults Peaks between 8 and 12 years of age More common in males Familial history of sleepwalking: 1 parent = 45% risk 2 parents = 60% risk Ambulation, during sleep Difficult to awaken during episode ,Eyes open Confusion/agitation ,Unusual or dangerous behaviors ,Rapid return to sleep , Usually occurs during the first half of the sleep period, with no memory of the event Patient may have coexisting confusional arousals and/or sleep terrors Diagnosed by history PSG not require Treatment: Reassurance (usually resolves spontaneously) Increase total sleep time Scheduled awakenings ,Bedroom/home safety counseling ,Screening for precipitating factors (e.g., sleep deprivation, obstructive sleep apnea, gastroesophageal reflux disease, acute stress, medication or illicit drug use) Hypnosis ,Scheduled awakening ( 15-30 minute ),Benzodiazepines , TCA?
Confusional Confusional arousals arousals Prevalence: 17.3% in 3- to 13-year-olds, 2.9% to 4.2% in those older than 15 years Affects males and females equally Strong familial pattern Sleep drunkenness Inappropriate behavior Slowed responsiveness Slurred speech Confusion after awakening Usually occurs during the first half of the sleep period, with no memory of the event Diagnosed by history PSG not require Reassurance (usually resolves spontaneously) Increase total sleep time Scheduled awakenings, Bedroom/home safety counseling
Sleep terrors Sleep terrors Episodes of sleep terror occur in 1% to 6% of children, with a peak between 4 and 8 years of age; gender differences have not been observed The child may sit up suddenly and scream with a blood-curdling battle-cry. intense fear (e.g., screaming, crying, confusion, walking), and this is accompanied by apparent autonomic activation, including mydriasis, tachycardia, and diaphoresis Difficult to awaken from episode ,Usually occurs during the first half of the sleep period, with no memory of the event, Considerable overlap with other parasomnia The event may last from a few minutes up to 20 minutes, but a longer duration May also be seen Diagnosed by history PSG not required Reassurance (usually resolves spontaneously) Increase total sleep time Scheduled awakenings , Bedroom/home safety counseling ,Benzodiazepines
Nightmares Nightmares Prevalence: 10% to 50% in 3- to 5-year-olds Onset between 3 and 6 years of age, peaks between 6 and 10 years of age Affects males and females equally Unpleasant dreams Increased sympathetic response (increased heart and respiratory rates, diaphoresis) Usually occurs during the second half of the sleep period, with clear memory of the event May be associated with mood disorders or posttraumatic stress disorder Diagnosed by history PSG not required Reassurance (usually resolves spontaneously) Increase total sleep time Scheduled awakenings , Bedroom/home safety counseling , Cognitive behavior therapy Medications that suppress rapid eye movement sleep (selective serotonin reuptake inhibitors ( fluoxetine, citalopram ) ; off- label use)
Restless leg syndrome Restless leg syndrome Unpleasant sensation in the legs, with the urge to move the legs starting in the evening Rest worsens symptoms, and movement provides some relief. Other symptoms include difficulty falling asleep, bedtime resistance, growing pains, and symptoms similar to those of attention-deficit/hyperactivity disorder Dopamine dysfunction, genetics, and iron deficiency are thought to play a role in the pathogenesis of restless legs syndrome Exacerbated by excessive or inadequate physical activity or the use of caffeine, nicotine, antihistamines, selective serotonin reuptake inhibitors, or tricyclic antidepressants Iron replacement should be initiated if ferritin levels are less than 50 mcg per L, and they should be rechecked in three months
Treatment of restless leg Treatment of restless leg syx syx Dopaminergic medications are widely used and considered first-line treatment for RLS Carbidopa/levodopa and dopamine agonists (pramipexole and ropinirole) are commonlused, and ropinirole was the first FDA-approved medication for treatment of moderate to severe primary RLS Another medication not FDA-approved for the treatment aof RLS in children but used clinically is clonidine, Clonazepam , gabapentine
Delayed Sleep Phase Disorder Delayed Sleep Phase Disorder The disorder is more common during adolescence when the circadian rhythm is thought to lengthen and the child becomes more social The prevalence in adolescents is 7% to 16% Treatment : Avoid bright lights before bedtime Removing all light-emitting devices (e.g., electronics, portable media, tablet computers, cell phones) Bright light therapy used for the first one to two hours after awakening There is strong evidence that melatonin supplementation (0.3 to 5 mg given 1.5 to 6.5 hours before desired bedtime) is effective
Pharmacotherapy in sleep disorders Pharmacotherapy in sleep disorders The individualized, based on the above evaluation. Other key considerations include: Child's age Pharmacotherapy is rarely appropriate for young children (<5 years), except for unusual circumstances such as significant caregiver physical or mental health issues or risk of child abuse. This is because behavioral causes and interventions are particularly common in this age group and also because of the lack of safety and efficacy data in this age group Acute versus chronic sleep problem Children with underlying medical, psychiatric, or neurodevelopmental conditions, in comparison with otherwise healthy, typically developing children, are more likely to need longer-term pharmacotherapy to address sleep issues. For children with these comorbid conditions, it is particularly important to address behavioral issues and to select medications that are less likely to have long-term side effects The most realistic immediate goal of treatment may be to improve rather than eliminate sleep problems decision about whether to initiate pharmacotherapy should be
The half-life and duration of action of the medication is particularly important and should be appropriate for the presenting complaint For children with sleep onset problems, a shorter-acting medication is generally desirable whereas for sleep maintenance problems, longer-acting medications may be considered, while at the same time minimizing morning residual sleepiness
Dosing The medication should be initiated at the lowest level and titrated up as necessary limited data on the pharmacokinetic and pharmacodynamic properties for hypnotic drugs in the pediatric For some medications (eg, zolpidem ) evidence suggests that younger children may require higher dosing (per kg) compared with adults due to differences in metabolism For some medications, this difference in metabolism results in a paradoxical reaction Timing Drug administration should be tailored to the drug's onset of action and the target time of sleep onset. Because most hypnotic medications have their onset of action within 30 minutes of administration and peak within one to two hours, they should be administered shortly before bedtime for sleep-onset insomnia, eg, within 30 minutes of lights out
Duration of pharmacotherapy Duration of pharmacotherapy The duration of pharmacotherapy depends on the type of sleep problem and the child's response to medical and behavioral treatment In general, medications should also be used for the shortest possible duration Avoid abrupt discontinuation of sleep medication, especially for drugs with short and intermediate half-lives Failure to wean sleep medications gradually because increased chance of: "rebound insomnia" and increase the likelihood of other sleep disorders For example, selective serotonin reuptake inhibitors [SSRIs]) may result in a compensatory increase (rebound) in REM sleep and a subsequent increase in REM sleep-related phenomena, such as nightmares
Dosing and administration of melatonin Dosing and administration of melatonin Circadian phase delay (eg, 0.2 to 0.5 mg) are typically given three to five hours prior to actual sleep onset time (or one to two hours before the desired bedtime). These relatively small doses and advance administration are more effective for circadian phase delay than larger doses or those given closer to sleep onset and appear to be safe Sleep-onset insomnia 1 to 2 mg in preschool children, 2 to 3 mg in school-aged children 5 mg in adolescents Given 30 minutes before bedtime Dosing should always begin at the lower range and be titrated up on a weekly basis as needed. Studies in children with autism have reported using doses of up to 10 mg (maximum dose recommended in guidelines for this population
Adverse effects of melatonin Adverse effects of melatonin Studies of melatonin use for durations of up to four years significant adverse effects in a variety of pediatric populations Potential side effects include suppression of the hypothalamic- gonadal axis (triggering precocious puberty on discontinuation), although at least one study found no effects on pubertal development Increased reactivity of the immune system in children with immune disorders or on immunosuppressants (ie, corticosteroids) has also been postulated At least one small study in adults suggested no suppression of endogenous melatonin with exogenous administration no
Benzodiazepines Benzodiazepines BZDs reduce sleep latency and may increase total sleep time; those BZDs with a longer half-life and duration of action have been more commonly used to address sleep maintenance BZDs have effects on sleep architecture, most notably, reduction in slow-wave sleep (SWS). These drugs also have muscle relaxant, anxiolytic, and anticonvulsant properties BZDs are occasionally used to treat intractable partial arousal parasomnias such as sleep terrors in children Side effects of BZDs include morning residual sleepiness, daytime sleepiness, and compromised daytime functioning
Alpha Alpha- -adrenergic agonists adrenergic agonists Alpha-adrenergic agonists (especially clonidine) are commonly prescribed to treat childhood insomnia. Anecdotal clinical experience suggests that these drugs are generally effective and well tolerated in children with ADHD and sleep-onset insomnia Drug is rapidly absorbed with an onset of action within one hour and peak effects at two to four hours Clonidine has a narrow therapeutic index. As a result, concerns have been raised about the potential for accidental or intentional overdose and associated toxicity, which may include respiratory depression, hypotension, and bradycardia
Antidepressants Antidepressants Use of low- dose doxepin and trazodone, and that tolerability and safety of antidepressants for insomnia is uncertain due to limited reporting of adverse events Antidepressants should be used for insomnia only in the presence of comorbid mood issues Most antidepressants, especially those with anticholinergic effects, suppress REM sleep and increase latency to REM sleep; thus, abrupt withdrawal may lead to increased nightmares as a result of REM sleep rebound
Tricyclic antidepressants Tricyclic antidepressants Most TCAs are sedating; the most sedating drugs are amitriptyline, doxepin, and trimipramine. TCAs decrease SOL (sleep onset latency ) and arousals and have been used to treat insomnia in adults who have underlying depression The most commonly reported side effects of TCAs are anxiety and agitation, as well as anticholinergic effects such as blurred vision, dry mouth, urinary retention, and orthostatic hypotension. There is a risk of cardiotoxicity, especially in prepubertal children, Most TCAs are potent REM sleep suppressants; thus, rapid withdrawal may lead to REM sleep rebound and nightmares TCAs also tend to suppress SWS, and withdrawal may lead to SWS rebound and an increase in partial-arousal parasomnias such as sleepwalking and sleep terrors TCAs may also exacerbate restless legs syndrome (RLS) symptoms.
Selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) vary widely in their effects on sleep. Fluvoxamine, paroxetine, and citalopram tend to be sedating and may be useful for management of insomnia in patients with underlying depression
Other medications Other medications Other classes of medications that reportedly have been used in clinical practice for pediatric insomnia, especially in patients with a comorbid neurodevelopmental or mood disorder, include mood stabilizers and anticonvulsants (eg, carbamazepine, valproic acid, topiramate, gabapentin), atypical antipsychotics (risperidone, olanzapine, quetiapine), and chloral hydrate. In most instances, these medications are prescribed for other indications such as bipolar disorder, aggression, or pain but may simultaneously be prescribed for their sleep-promoting properties. Clinical data for all of these agents in the pediatric population are largely limited to case reports and case studies, and evidence is also very limited in adults All of these medications should be used with caution chloral hydrate and barbiturates should not be used to treat insomnia in children, because of significant side effects.
Home message Home message Up to 50% of children will experience a sleep problem Vast majority of sleep disturbances in children and adolescents are appropriately managed with behavioral therapy alone pharmacotherapy is rarely necessary or appropriate for healthy children with sleep problems The decision to initiate pharmacotherapy should be made on a case-by-case basis after a careful assessment of the sleep problem, including behavioral, medical, and psychosocial contributors Antihistamines can be considered for short-term situational or occasional use in younger children, especially those with comorbid atopic disease Melatonin is most appropriately used in patients with circadian phase delay, sleep-onset insomnia Alpha-adrenergic agonists (clonidine or guanfacine) are commonly used off-label for treatment of insomnia in children, particularly those with sleep onset delay and ADHD Antidepressants should be used for insomnia only in the presence of comorbid mood issues