Evaluation of Acute Scrotum in Children: Clinical Insights and Imaging Findings

Understanding the differential diagnosis of acute scrotum in children is vital, with key considerations for testicular torsion, appendix torsion, epididymitis, orchitis, hematocele, and hernia. Relevant imaging plays a crucial role in ruling out torsion and determining the appropriate management based on clinical presentation and TWIST score assessment.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Acute Scrotum in Children John McCarthy 12/11/2020 RAD 4001 Dr. Tavernier
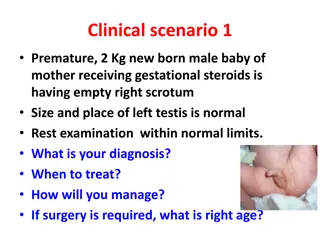
Clinical History Patient is an 11-yo male presenting to the ED with 1 hour of right scrotal pain radiating to RLQ. No trauma, worse when standing. Pain 4/10. PMH of asthma and testicular torsion in 2017, followed by UT Urology Denies nausea/vomiting, patient afebrile, VSS Right testicle TTP, with no visible swelling or erythema, mildly TTP in all four abdominal quadrants, normal bowel sounds, no rebound or guarding Right testicle with vertical lie in scrotum, no appreciable nodules Initial workup: 1. U/A and U C(x) negative Duplex Doppler U/S of Testes
Differential Diagnosis Acute Scrotum in Children DDX: Testicular Torsion: major concern due to PMH. Typically acute in onset with severe pain, high riding testicle, and absent cremasteric reflex. Appendix Torsion: more common than testicular torsion (29% ASP vs 19%). Typically more gradual with less severe pain. Epididymitis: typically 2/2 to UTI Orchitis: 2/2 bacterial or viral infection (mumps) Hematocele: 2/2 trauma Hernia
Relevant Imaging: Anatomy of Testes Anterior: skin Epidydimal head Tunica Albuginea Epidydimal tail RTesticle Cranial Caudal Posterior
Relevant Imaging continued Appendix Epididymis Testicular appendage torsion: appears as an area of low echogenicity adjacent to epididymis with mesh-like echotexture Often not visualized: a diagnosis of exclusion once testicular torsion is ruled out
Clinical Picture & Imaging Findings TWIST Score can be used to assess for testicular torsion in children Testicular swelling: 2 points Hard testicle: 2 points Absent cremasteric reflex: 1 point Nausea/vomiting: 1 point High-riding testicle: 1 point Score of 2-5 requires U/S for assessment Score>5: PPV 100% : requires urgent urologic/surgical consult with possible orchiopexy Our patient: preserved blood flow in both testes, no masses, hernias, or visible signs of infection. Likely R appendix epididymis torsion: round hypoechoic structure adjacent to epididymis with mesh-like echotexture and no flow
Discussion Torsion of Testicular Appendage: Most common between ages of 7 14 Has no effect on fertility or surrounding structures Presents with: More mild scrotal pain than torsion, often localized to one point of testicle Physical exam: Hard, tender, 2-3 mm nodule at upper pole of teste Workup: U/A and ultrasound T(x): scrotal elevation, ice, NSAIDs, resolves between 7-10 days
ACR appropriateness Criteria US duplex Doppler appropriate per ACR criteria Cost at MHH: $1184 per Charge Description Master file
Take Home Points / Teaching points Acute scrotal pain in the pediatric population should be worked up emergently Must assess for blood flow in testes using Duplex Doppler U/S Absent blood flow in unilateral testicle signifies torsion and requires urgent surgical orchiopexy Appendix torsion is a diagnosis of exclusion but can sometimes be visualized on U/S
References Urologic Imaging Without X-rays: Ultrasound, MRI, and Nuclear MedicineAndrew C Peterson, MD, FACS et al in eMedicine Scrotal pathology in pediatrics with sonographic imaging (PubMed).Munden MM, Trautwein LM. in Curr Probl Diagn Radiol. 2000 Nov-Dec;29(6):185-205. Clinical and sonographic criteria of acute scrotum in children. Karmazyn B, Steinberg R, Kornreich L, et al. in Pediatr Radiol 2005;35:302-310. https://wikem.org/wiki/Torsion_of_testicular_appendage https://www.memorialhealthcare.org/patient-information/financial-services/pricing/ https://assets.radiopaedia.org/articles/torsion-of-the-appendix-testis