Esophagus Anatomy, Physiology, and Diseases
Explore the anatomy and function of the esophagus, including its layers, innervation, and common disorders like dysphagia, motility disorders, strictures, and rings/webs. Learn about diagnostic methods such as barium swallow studies and endoscopy, as well as treatment options for conditions like achalasia and diffuse esophageal spasm.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Esophagus Anatomy, Physiology, and Diseases Alan Chu March 13, 2013
Anatomy 18 26cm from UES to LES Esophageal wall layers Mucosa, submucosa, muscularis propia, adventitia Proximal 33% skeletal muscle, middle 35-40% mixed, distal 50-60% smooth muscle Smooth muscle innervated by CN X. Auerbach plexus: peristalsis Meissner s plexus: afferent input
Oropharyngeal dysphagia Difficulty initiating swallow followed by choking/coughing Esophageal dysphagia Anatomaic vs neuromuscular defect Solid vs solid+liquid dysphagia
Dysphagia best assessed by MBSS Demonstrates presence of oropharyngeal dysfunction and aspiration
Standard upper endoscope 9mm, transnasal endoscope 4mm Z line = GE junction In barrett s squamocolumnar junction more proximal than GEJ
Esophageal Motility disorder Acalasia Insufficient LES relaxation Dilated distal 2/3 esophagus with bird s beak appearance at LES on esophagram Upper endoscopy to r/o pseudoachalasia 2/2 to GEJ tumor Tx: balloon dilation to disrupt circular muscle fibers at LES; Heller s myotomy via laproscopic approach; Botox/CCB/nitrates
Esophageal Motility Disorder Diffuse Esophageal Spasm Simultaneous and repetitive contraction in esophagus body with normal LES Cockscrew esophagus on esophagram Tx:nitrates/CCB Nutcraker esophagus High-amplitude peristalsis Ineffective esophageal motility High incidence in patients with GERD
Strictures Dysphagia when <15mm Tx: dilators (Bougies, Savary dilator, balloon dilator) Risk of perforation 0.5%, higher in XRT induced strictures Goal >15mm
Rings or Webs Ring Circumferential, muscle or mucosa, at distal esophagus Schatzki s ring Eosinophilic Esophagitis (>15 eosinophils/hpf in mucosa) Web Part of lumen, mucosal, proximal esophagus Plummer Vinson
GERD Chronic symptoms 2/2 abnormal reflux of gastric contents Heartburn, acid regurgitation, dysphagia, odynophagia, belching Tx: lifestyle modification, H2 blockers (60%), PPI (90%), surgery Atypical extraesophgeal symptoms: asthma, chest pain, cough, laryngitis, dental erosion
Barretts esophagus Pale pink squamous mucosa replaced with salmon pink columnar mucosa LSBE vs SSBE (<3cm) Risk of esophageal adenoCA 0.5% per year
Neoplasia AdenoCA Distal esophagus or GEJ Barrett s SCC Mid-esopahgus and proximal esophagus Tobacco, EtOH use in AA
Diverticula Zenker s diverticulum Midesophageal diveticula Epiphrenic diverticula Intramural pseudodiverticulosis
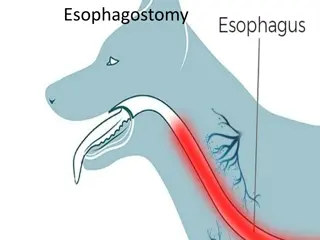
Transnasal Esophagoscopy Alan Chu March 13, 2013
Transnasal esophagoscope 3.1 5.1mm Performed without sedation Shorter procedure time 66% cost of transoral esophagoscope Conventional Transoral esophagoscope 10 - 12mm Performed with sedation Longer procedure time
Transnasal esophagoscope Smaller biopsy size Conventional Transoral esophagoscope
Indications Head and Neck SCC Replaces panendoscopy Barrett s esophagus Surveillence of Barrett s esophagus Stricture dilation Balloon dilation Tracheoesophageal puncture
Technique Topical anesthetic and decongestant Pt s head flexed and swallows as scope approaches cricoid level Z-line (squamocolumnar junction) visualized Retroflex view of gastric cardia