Diabetes and Pregnancy: Impact, Complications, and Management
This presentation delves into the potential impact of metabolic syndrome and diabetes on women's reproductive health. It covers topics such as preconception counseling for patients with preexisting diabetes mellitus, complications associated with poorly controlled diabetes in pregnancy, baseline evaluations, blood glucose control goals, monitoring recommendations, and the broader implications of diabetes on women's reproductive health. Epidemiological data is also provided, highlighting the prevalence of diabetes in pregnancies and the various types of diabetes affecting pregnant women.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Diabetes and Pregnancy Karen Playforth, MFM Associate Professor, Department of OB/GYN September 14th, 2018
Karen Playforth, MD, MFM I have no conflicts of interest to disclose.
Overarching Objective Upon completion of this activity, participants will be able to: Explain the potential impact of metabolic syndrome or diabetes on the reproductive health of females
Specific Objectives Upon completion of this activity, participants will be able to: Recognize the importance of preconception counseling in patients with preexisting diabetes mellitus and of post-partum testing and counseling of patients with gestational diabetes mellitus; List the complications of pregnancy associated with poorly controlled preexisting diabetes mellitus in the first trimester of pregnancy; Name the complications of pregnancy common to both preexisting and gestational diabetes mellitus; Describe the baseline lab work and evaluations done in pregnancy for preexisting and gestational diabetes mellitus patients and why; Recall the goals for blood glucose control in pregnancy and why; Restate the recommendations for monitoring and delivery timing for pregnancies complicated by diabetes; Explain the bigger picture of diabetes and the reproductive health of women.
Epidemiology Approximately 7% of pregnancies are affected by ANY TYPE of diabetes Preexisting diabetes complicates ~1 % of pregnancies in US Type 1 DM accounts for 5-10% of patients diagnosed with diabetes in the general population Incidence of Type 2 DM is very dependent on the population studied Gestational diabetes (GDM) accounts for 86% of diabetes in pregnancy Yang JE, Cummings EA, O'Connell C, Jangaard K: Fetal and neonatal outcomes of diabetic pregnancies. Obstet Gynecol 2006. ACOG Practice Bulletin Number 190, February 2018. ACOG Practice Bulletin Number 60, March 2005.
Epidemiology Total of 30.2 million people, or 12.2% of the U.S. population, have diabetes 23 million people with diagnosed diabetes 7.2 million people with undiagnosed diabetes 14.9 million, or 11.7 %, of all women age 18 years or older have diabetes Data source: 2011 2014 National Health and Nutrition Examination Survey and 2015 U.S. Census Bureau data.
11.1% of Kentucky women are diagnosed with diabetes Data source: 2011 2014 National Health and Nutrition Examination Survey and 2015 U.S. Census Bureau data.
Epidemiology Risk Factors for Diabetes Obesity Sedentary lifestyle Family history Genetics Ethnicity Age INTRAUTERINE ENVIRONMENT
Epidemiology Exponential rise in numbers of pregnancies affected by diabetes mellitus Diabesity infants of mothers with diabetes (Type 1) diabetes/prediabetes in reproductive age women 5% to 10% of women with GDM develop Type 2 immediately after pregnancy 35% to 60% of women with GDM develop Type 2 within the 10 20 years Among Hispanic women, approximately 50% develop Type 2 within 2 years
GDM and Offspring Obesity ? Child obesity
Complications and Interventions
Complications in 1st Trimester Uncontrolled preexisting DM in first trimester of pregnancy = Maternal hyperglycemia Miscarriage Congenital anomalies Open neural tube defects Heart defects
Interventions in First Trimester (or before) Preconception counseling Risk to fetus for congenital malformations highest often before they know they are pregnant HgbA1c > 8% risk of miscarriage is 26 times baseline risk HgbA1c > 10% confers 25% risk of congenital malformation
Interventions in 1st Trimester Diabetes Re-Education Different rules in pregnancy First trimester Ultrasound to establish dates Baseline labs and evaluations 24 hour urine protein, preeclampsia labs, TSH, maternal echo, ophthalmology exam Start daily low dose aspirin between 12-16 weeks of pregnancy and continue until delivery
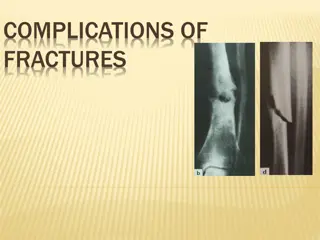
Complications in 2nd and 3rd Trimester Uncontrolled DM in second and third trimester of pregnancy = Hyperglycemia and Hyperinsulinemia Premature delivery Preeclampsia Stillbirth Macrosomia Shoulder dystocia Operative delivery Maternal or fetal trauma NICU admission Childhood obesity and diabetes mellitus
Fractured clavicle Erb s Palsy
Arch Pediatr Adolesc Med. 1998;152(3):249-254. doi:10.1001/archpedi.152.3.249
Interventions in 2nd and 3rd Trimester Strict blood glucose control Fasting < 95mg/dl (I prefer <90mg/dl) Pre-prandial <100mg/dl Post-prandial <120mg/dl Bedtime <100mg/dl Close follow-up Nutritional Counseling and Diabetes Self-Management Education Serial ultrasounds for anatomic survey and then for growth q 4 weeks Antenatal testing Delivery timing
Antepartum Testing Ultrasounds For dating To assess for congenital malformations Growth assessment Fetal echocardiogram Non-Stress Tests begun generally between 32-34 weeks, but individualized based on underlying risk
Delivery Timing Balance the risk of IUFD with risks of preterm birth Poorly controlled delivery between 37-39 weeks Evidence of compromise/elevated risk profile consider delivery before 39 weeks Well-controlled, A1 s may go to EDC Expectant management beyond is not recommended


















")





:249-254.")