Culprit Artery Localization in STEMI: Insights from a Cardiology Presentation
Dr. Suneesh K., a Senior Resident in the Dept. of Cardiology at Calicut Medical College, delves into the crucial role of ECG analysis in identifying the culprit artery during ST-elevation myocardial infarction (STEMI). This presentation covers coronary circulation, blood supply of the heart, prevalence of STEMI, and the significance of immediate prognosis based on ECG findings. Explore how surface ECG correlations can guide reperfusion strategies and predict mortality in acute myocardial infarction cases.

Download Presentation

Please find below an Image/Link to download the presentation.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.If you encounter any issues during the download, it is possible that the publisher has removed the file from their server.
You are allowed to download the files provided on this website for personal or commercial use, subject to the condition that they are used lawfully. All files are the property of their respective owners.
The content on the website is provided AS IS for your information and personal use only. It may not be sold, licensed, or shared on other websites without obtaining consent from the author.
E N D
Presentation Transcript
Localization of culprit artery in Localization of culprit artery in STEMI STEMI Topic presentation Speaker Dr.Suneesh.K Senior Resident, Dept. of Cardiology Calicut Medical College
Overview Overview Introduction Coronary circulation and blood supply of the heart AWMI IWMI RVMI PWMI Conduction disturbances Atrial Infarction Exercises 15-09-2024
Introduction Introduction Careful analysis of the surface ECG is highly useful in localizing the culprit vessel and immediate prognostication Helps in deciding the need for an aggressive reperfusion strategy ECG correlation of infarct related artery predict moratlity in acute myocardial infarction
Prevalence of STEMI Prevalence of STEMI Inferior 58% Anterior 39% Other 3% Newby et al, GUSTO Study J Am Coll Cardiol1996;27:625-32
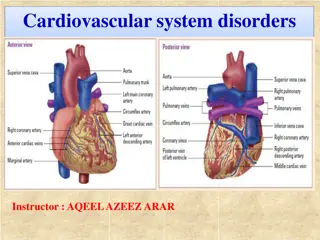
Coronary circulation Coronary circulation Left Main or left coronary artery LAD Diagonal braches (D1, D2) Septal branches Circumflex Marginal branches (M1, M2) Right coronary artery Conus, sinoatrial branch RV branch Acute marginal branch AV nodal branch Posterior descending artery (PDA)
Blood supply of heart Blood supply of heart LAD Supplies the anterior, lateral, anterior two-thirds of septum, and frequently the inferoapical segments of LV, including the proximal part of bundle branches RCA Perfuses SA node (65%), AV node, postero-medial papillary muscle, inferior part of LV, RV, and variably also the posterior and lateral segments
Blood supply of heart (contd..) Blood supply of heart (contd..) Circumflex branch Posterior wall and variably inferior and lateral segments Posterior wall involvement usually underestimated and under treated
Blood supply of heart (contd..) Blood supply of heart (contd..) SA node RCA in 65% AV node RCA in 90% Bundle of His Mainly RCA RBB LAD LBB L Ant branch LAD LBB - L Post branch LAD & PDA
Dominance Dominance Supplies circulation to the inferior wall and inferior portion of the posterior IVS Dominant artery passes crux and IVS, giving rise to posterolateral branches and PDA Dominant artery also gives rise to the AV nodal branch Nondominant artery is usually smaller in size and terminates early in its respective AV groove
Dominance Dominance RCA 70% LCX 10% Co- dominant 20%
Right dominant Right dominant
Left dominant Left dominant
The concept of injury vector: The concept of injury vector: Direct and reciprocal changes Direct and reciprocal changes Injury vector is oriented towards the injured area and generates STE in the leads facing the vector s head ST-segment depression in the leads facing the vector s tail (opposed leads) Leads perpendicular to dominant vector will record an iso- electrical ST segment
Proximal occlusion of long LAD Proximal occlusion of long LAD Distal occlusion of long LAD Distal occlusion of long LAD
Ischemia at a distance Vs reciprocal Ischemia at a distance Vs reciprocal changes changes Patients with ST elevation in one territory often have ST depression in other territories The additional ST deviation may represent acute ischemia due to coronary artery disease in non infarct related arteries (ischemia at a distance) or may represent pure "mirror image" reciprocal changes Most of the common patterns of remote ST depression probably represent reciprocal changes and not ischemia at a distance
AWMI AWMI
Anteroseptal zone: occlusion of the Anteroseptal zone: occlusion of the LAD and its branches LAD and its branches Proximal to 1st septal and 1st diagonal branch (40%) Distal to S and D (40%) Proximal to D1 but distal to S1 (5-10%) Proximal to S1 but distal to D1 (5-10%) Selective D1 D2occlusion Selective S1 S2 occlusion
Proximal LAD occlusion (Dominance of Basal area) Injury vector is directed anteriorly and upward, and somewhat to the right or left
Proximal LAD occlusion (Dominance of Basal area)
Proximal LAD occlusion (Dominance of Basal area) STE aVR and STE in V1 > 2.5 mm ST depression in inferior leads and in V5 Abnormal Q in aVL ST depression in the inferior wall (III +aVF 2.5 mm) is quite suggestive of a proximal occlusion of LAD above D1
Distal LAD occlusion Distal LAD occlusion (Dominance of inferoapical area) (Dominance of inferoapical area)
Distal LAD occlusion Distal LAD occlusion (Dominance of inferoapical area) (Dominance of inferoapical area)
Distal LAD occlusion Distal LAD occlusion (Dominance of inferoapical area) (Dominance of inferoapical area) Inferior third of the LV & low-lateral involvement (apical infarction) STE is seen in the precordial and inferior leads in the presence of Injury vector is directed forward and left, and downward a STEMI due to the very proximal occlusion of the RCA STE in inferior leads (II > III) in addition to V3-V6 In this case the STE usually is V1>V3 4, while in a STEMI due Slight ST-segment depression in aVR to the distal occlusion of the LAD the opposite occurs Wide Q V4-V6 some times (i.e., the STE is V1<V3 4)
1 1st st Diagonal not involved Diagonal not involved (Dominance of septal area) (Dominance of septal area)- -Proximal to S1 Proximal to S1
1 1st st Diagonal not involved Diagonal not involved (Dominance of septal area) (Dominance of septal area)- -Proximal to S1 Proximal to S1 Injury vector is directed anteriorly, to the right and sometimes downward
1 1st st Diagonal not involved Diagonal not involved (Dominance of septal area) (Dominance of septal area)- -Proximal to S1 Proximal to S1 Antero-septal infarction STE in aVR and > 2.5 mm STE in V1 ST elevation from V1to V3 4and II, III, and aVF ST depression in V6, I and aVL STE in V3R RBBB/ QRBBB
1 1st st Diagonal not involved Diagonal not involved (Dominance of septal area) (Dominance of septal area)- -Proximal to S1 Proximal to S1
First septal branch not included First septal branch not included (Dominance of Lateral area) (Dominance of Lateral area) Prox to D1 Prox to D1 Injury vector is directed anteriorly, upward, and somewhat to the left
First septal branch not included First septal branch not included (Dominance of Lateral area) (Dominance of Lateral area) Prox to D1 Prox to D1 ST elevation lead AVL & lead I Q left lateral leads ST depression in Lead III > Lead II ST depression in (III + aVF) 2.5 mm
First septal branch not included First septal branch not included (Dominance of Lateral area) (Dominance of Lateral area) Prox to D1 Prox to D1
First septal branch not included First septal branch not included (Dominance of Lateral area) (Dominance of Lateral area) Prox to D1 Prox to D1
ECG criteria to identify site of ECG criteria to identify site of occlusion in the LAD occlusion in the LAD
New QRBBB in V1 is a specific but insensitive marker of proX LAD occlusion
Selective occlusion of the D1branch Selective occlusion of the D1branch Area affected -Mid-low anterior wall and part of the mid- and often low-lateral wall Injury vector is directed upward, to the left and forward STE in I, aVL and precordial leads V2 V6 (Variable) ST depression in II, III, and VF (III >II)
Selective occlusion of the D1branch Selective occlusion of the D1branch
Selective occlusion of the S1branch Selective occlusion of the S1branch Septal wall with occasionally certain extension toward the anterior wall Injury vector directed anteriorly, upward, and to the right STE in V1,V2, and aVR ST depression in II, III, aVF (II>III), and V6 No ST elevation in aVL
Selective occlusion of the S1branch Selective occlusion of the S1branch
Algorithm for ECG Identification of the Infarct-Related Artery in AW-STEMI Engelen DJ, Gorgels AP, Cheriex EC et al J Am Coll Cardiol 1999; 34:389-95
IWMI IWMI
Injury vector in RCA and LCX Injury vector in RCA and LCX
Right coronary Right coronary Circumflex coronary Circumflex coronary Inferoseptal ischemia Inferoposterolateral ischemia Vector directed to III Directed to II STE III > II STE II > III ST depression in aVL>I STE I or aVL or both RV can be involved True PWMI can occur V5 and V6 are of little value in differentiating between RCA or Cx occlusion. STE in these leads implies a larger area at risk
Occlusion of the RCA Occlusion of the RCA ST elevation in III > II ST depression in I and aVL - aVL > I ST depression in the right precordial leads is smaller than STE in inferior leads When occlusion is proximal to RV branches ST E in V1 > V3 V4
Occlusion of the RCA (Contd..) Occlusion of the RCA (Contd..) When RCA is dominant, STE is seen in V5 and V6 (Local injury vector) Involvement of posterior wall RCA very dominant or super dominant - STE elevation 2 mm in V5-V6 and ST depression in I and aVL Eskola et al. 2004






")
")









































")